 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Human Genetics, Vol. 17, No. 3, September-December, 2011, pp. 229-231 Case Report Ross operation in a neuro-cardio-facial-cutaneous syndrome patient Keyhan S Zanjani1, Ali Akbar Zeinaloo1, Hassan Radmehr2 1 Department of Pediatrics, Pediatric Center of Excellence, Children's Medical Center, Tehran, Iran Code Number: hg11047 DOI: 10.4103/0971-6866.92097 Abstract Congenital heart diseases are a major part of Costello and cardio-facio-cutaneous syndromes. Subaortic stenosis was reported rarely and Ross operation never in these syndromes.
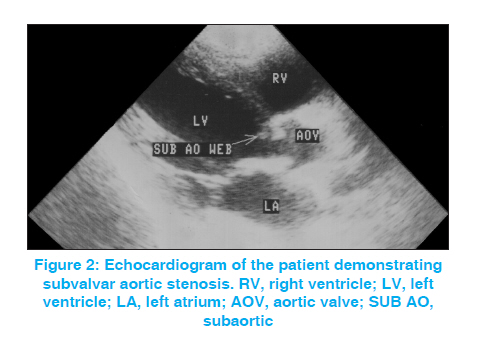
Keywords: Cardio-facio-cutaneous syndrome, Costello syndrome, Ross operation, Subaortic stenosis Introduction The neuro-cardio-facial-cutaneous syndromes consist of neurofibromatosis type 1, Noonan, LEOPARD, Costello and cardio-facio-cutaneous (CFC) syndromes. Genetic alterations in the RAS-MAPKinase pathway produce these syndromes. Regulation of cellular proliferation, differentiation and survival is the task of this pathway. [1] Psychomotor retardation, congenital heart diseases (CHD), facial abnormalities, short stature, skin problems and cancer predisposition are common findings in these syndromes. [1] However, the responsible genetic mutations are different. HRAS gene mutations are responsible for Costello syndrome while those in several others (BRAF, KRAS, MEK-1 or MEK-2) cause CFC syndrome. [1] We reported on a patient with characteristics in favor of Costello or CFC syndromes. Differentiation between these two entities in this patient was not possible solely on the clinical findings. Unfortunately, genetic testing was not performed before her death. However, Ross operation was reported neither in patients with Costello syndrome nor in those with CFC syndrome to the best of our knowledge. Case Report The patient was a girl with subaortic stenosis, keratosis pilaris, growth retardation, nail dystrophy, bitemporal hollowing, macrocephaly and sparse scalp hair [Figure - 1]. At 5 years of age, her weight was 14 kg (below 5 th percentile), height 91 cm (below 5 th percentile) and head circumference 54 cm. At 9 years, her weight was 16.5 kg (below 5 th percentile) and height 110 cm (below 5 th percentile). She was well developed and had no mental problem. Mild food aversion in infancy was reported by her mother. There was no history of maternal polyhydramnios. Her biopsy-proven keratosis pilaris was widespread, involving almost all parts of her body. Nail dystrophy was more announced on the toes than on the fingers. Abdominal ultrasonography suggested mild splenomegaly. Teeth abnormalities, webbed neck and cubitus valgus were not found. She was born to relative parents (first cousins). Her only sibling was healthy. The heart disease was diagnosed since 4 years of age. A grade III/VI systolic murmur was heard at the upper chest. Electrocardiogram showed left ventricular hypertrophy. Echocardiography revealed a subaortic obstructive web [Figure - 2]. At 5 years, pressure gradient (PG) between the left ventricle (LV) and the aorta was 50 mmHg on echocardiography and 30 during catheterism. She also had mild aortic regurgitation. The subaortic obstructive tissue was resected surgically 2 weeks later. Because of the progressive aortic insufficiency and subaortic restenosis (PG = 70 mmHg echocardiographically, ST segment depression on electrocardiogram), Ross operation was carried out at the age of 9 years. The pulmonary valve is translocated to the aortic valve position (neoaortic valve) and a homograft is implanted in the pulmonary valve position. Two and a half years after the Ross operation, she returned complaining of shortness of breath and easy fatigability. Echocardiography showed complete absence of the autograft function with free regurgitation. Aortic root (2.84 mm) and LV (5.3 mm end-diastolic diameter) had greatly increased dimensions. A decision of surgical aortic valve replacement was made. A 19-mm St. Jude valve (St. Jude Medical Inc., St. Paul, MN, USA) was implanted 4 months later. After the operation, a stormy course occurred with low cardiac output leading to renal and hepatic failures, severe coagulation abnormality, progressive loss of consciousness and, finally, death of the patient at the age of 11 years and 10 months. Discussion The presented case had certain manifestations such as failure to thrive, CHD, widespread hyperkeratotic skin lesions, sparse hair and relative macrocephaly, which are consistent with both the diagnosis of Costello and CFC syndromes. However, differentiation between these two entities was difficult based only on the clinical findings. Genetic testing was not performed for this patient. CHD is common in both syndromes. Cardiac abnormalities were found in 63% of the patients with Costello syndrome, consisting of structural defects in 30% (most commonly pulmonic stenosis), myocardial hypertrophy in 34% and arrhythmias in 33%. [2] Subaortic stenosis was reported in these patients, although only in a few cases. [2] CFC syndrome is accompanied by a cardiac abnormality in around 76% of the patients. [3] Pulmonary valvar stenosis is the leading abnormality in this syndrome as well, being seen in 47%. Hypertrophic cardiomyopathy (40%) and atrial septal defects (23%) follow that abnormality. As far as the authors know, subaortic stenosis as the cardiac manifestation of CFC syndrome was reported only once. [4] Ross operation consists of autografting pulmonary valve in place of the aortic valve and putting a homograft in place of the pulmonary valve. This operation is used when the aortic valve should be replaced and a prosthetic valve is not desirable. Severe autograft dysfunction with free regurgitation 2.5 years after the Ross operation, like that seen in our patient, is rare. In the cohort of Böhm et al., severe autograft regurgitation occurred in 14 of 467 patients (3%), requiring reoperation after a mean of 39.3 months. [5] In that of de Kerchove et al., the autograft was reoperated due to severe regurgitation in 18 of 218 patients (8.3%). Mean delay to reoperation was 8.7 and 6 years in the two studied subgroups. [6] We did not see such an occurrence in our patients after Ross operation, as well. As far as the authors know, this patient is the first patient with either CFC or Costello syndrome on whom a Ross operation was carried out. Relatively rapid destruction of the neoaortic valve (2.5 years) in spite of echocardiographical normality before the operation may be due to a subtle structural pathology in the pulmonary valve. Although it is difficult to come into conclusion based only on one patient, it may be advisable to avoid Ross operation in these patients even if the pulmonary valve seems to be normal echocardiographically. References
Copyright 2011 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg11047f2.jpg] [hg11047f1.jpg] |
| |||||||||

{kind=link}
{kind=link}