 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
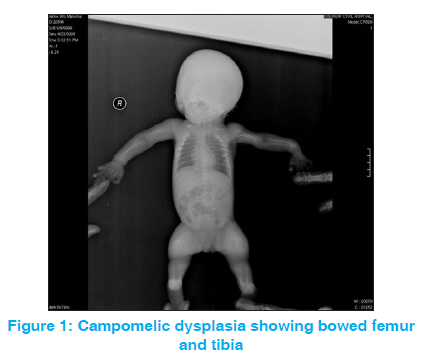
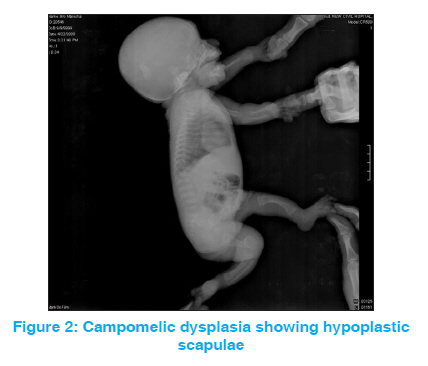
Indian Journal of Human Genetics, Vol. 17, No. 3, September-December, 2011, pp. 247-248 Letter to the Editor Campomelic dysplasia Jagdish P Goyal1, Anshul Gupta2, Vijay B Shah1 1 Department of Pediatrics, Government Medical College, Surat, Gujarat, India Code Number: hg11054 DOI: 10.4103/0971-6866.92085 Sir, Campo (bent)-melia (limbs) is a rare (incidence 0.05-1.6 per 10,000), usually lethal congenital skeletal dysplasia with near total mortality in neonatal period. [1] Our case was a 1.75 kg, small-for-gestational age (SGA) female child delivered to a third gravida mother by lower segment cesarean section (LSCS). Apgar scores at 1 and 5 min were 7 and 8 respectively. Antenatal USG at eight months of gestation was suggestive of skeletal dysplasia and oligohydroamnios. There was no history of consanguinity. Karyotype for female was normal, 46XX. Other two siblings were also normal. Further genetic studies were not done due to financial constraints. On examination, the baby had respiratory distress, short birth length (45 cm), macrocephaly (head circumference 39 cm), micrognathia, low set ear, flat nasal bridge, hypertelorism, short and bowed lower limbs and pretibial skin dimpling on anterior side of tibia. Radiograph of the patient revealed bowed femur and tibia, hypoplastic scapula, absent parietal bone and large fontanelle [Figure - 1] and [Figure - 2]. USG of abdomen was normal. Septic screen was also negative. Baby expired on third day of life due to respiratory complications. Campomelic dyslasia is diagnosed on the basis of clinical and radiological features. [2],[3] Our patient fulfilled both clinical and radiological criteria. Exact mode of inheritance is controversial (autosomal recessive/dominant), but the chromosomal abnormality in17q resulting in abnormality in cartilage formation. In two-thirds of affected individuals with a 46, XY karyotype, male-to-female sex reversal had been described. [4] Most of the patients of campomelic dysplasia died in neonatal period due to severe respiratory distress which might be due to traceomalacia. [5] Campomelic dyslasia should be differentiated from thanatophoric dysplasia in which X-ray had the classical curved telephone receiver shaped femur. As in the case of other neonatal lethal autosomal dominant disorders that have been thought to be autosomal recessive (e.g., osteogenesis imperfecta congenita), parents of infants with campomelic dysplasia had probably been often dissuaded from having further children as it results from new mutational event and has low risk of recurrence in subsequent pregnancies. References
Copyright 2011 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg11054f2.jpg] [hg11054f1.jpg] |
| |||||||||

{kind=link}
{kind=link}