 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
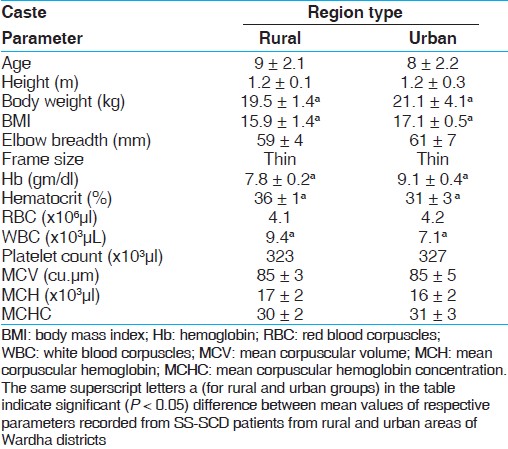
Indian Journal of Human Genetics, Vol. 18, No. 1, January-April, 2012, pp. 40-42 An anthropometric and hematological comparison of sickle cell disease children from rural and urban areas HS Nikhar1, SU Meshram2, GB Shinde3 1 Department of Microbiology, R.T.M. Nagpur University, L.I.T. Premises, Nagpur, India Code Number: hg12006 DOI: 10.4103/0971-6866.96643 Abstract Background: Sickle cell disease (SCD) is a prevalent genetic disorder in India and the rural and urban areas experience distinctly different healthcare facilities. In view of this, a comparative study of SCD-SS pattern children of age 8-15 years from rural and urban areas of Wardha district of Central India was carried out using anthropometric and hematological parameters.
Keywords: Body mass index, hemoglobin, rural and urban area, sickle cell disease Introduction Sickle cell disease (SCD), a genetic disorder, is prevalent in many areas of India. [1] However, the reported prevalence estimates show an enormous variation (i.e., 0-40%). [2],[3],[4] So far, the initiatives of Indian Government have not shown great results of improving the quality of life of SCD sufferers. The disparity in nutritional intake in rural and urban areas may affect the physical development of SCD children. [5] In this report, we present the results of the comparative assessment of selected anthropometric and hematological parameters of SCD sufferers (SCD-SS) belonging to rural and urban areas of Wardha district of Central India. Materials and Methods Following purposive sampling method, 55 and 50 samples (SCD affected SS pattern) from rural and urban areas of Wardha districts were selected for this study. The SCD condition was confirmed by conducting solubility test method, [6] followed by SCD pattern (AS and SS) confirmation using cellulose acetate electrophoresis at pH 8.9. [7] Only SS pattern SCD children of age 8-15 years were selected for this study. The hematological parameters included hemoglobin, red blood corpuscles (RBC), white blood corpuscles (WBC), mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), and mean corpuscular hemoglobin concentration (MCHC) and the anthropometric measurements for height-weight [for body mass index (BMI) determination] were recorded by standard methods. Frame size was determined from height and measuring the breadth of elbow. Statistical analysis of the data was done using SPSS 18.0 software. Results and Discussion The results presented in [Table - 1] indicate the hematological and anthropometric measurements of SCD (SS pattern) children from rural and urban areas of Wardha district, respectively. The SCD children (from rural and urban areas) exhibited statistically significant (P < 0.05) lower values for all the measurements. The comparative assessment of the hematological and anthropometric parameter values of SCD children belonging to rural and urban areas revealed remarkable difference. Specifically, hemoglobin, hematocrit, RBC, WBC, weight, and BMI parameters showed statistically significant (P < 0.05) difference in the mean values. However, there was no significant difference between SS-SCD children with respect to platelet count, MCV, MCH, MCHC, height mean values, and the frame size for children belonging to both the areas. SCD is prevalent in India and often considered to be associated with specific communities. However, the demotechnique growth along with social change in this century is largely responsible for certain changes in the prevalence of SCD. This view can be corroborated with the large number of studies pertaining to prevalence of SCD in different regions as well as communities. [8] Although the SCD is considered to be a clinically benign condition, the past studies show that the pathophysiology is distinctly different than that is observed with the normal people. [9] In addition to this, most of the studies carried out in India and elsewhere have reported comparison of SCD patients with normal population with respect to various anatomical, hematological, and anthropometric parameters of normal and SCD populations. A reasonable amount of literature [10] has now indicated that the SCD patients experience adverse effect upon the physical growth and development; however, more data are needed, especially from India to confirm this view. In the backdrop of above information, this study made an attempt to compare the anthropometric and hematological parameters from SS-SCD patients from rural and urban backgrounds. Growth delay starts in early childhood but becomes more apparent during adolescence when the growth spurt of normal children separates them from the patients with SCD. [11] Apparently, the adequate nutritional supplement at young age thus is a prerequisite for relatively less difficult adolescence and higher age. [12] It is in this context, the comparative assessment of rural (compromised nutrition) and urban children with respect to nutrition is critical, which can provide a more clear picture to healthcare professional for delineating therapies (preventive and prophylactic) for SCD patients vis-à-vis various infectious diseases. It is often considered that anemia plays a critical role in the pathophysiology of SCD. However, to rectify this problem, therapies such as transfusion and nutritional supplements [13] may act effective. In this study, very low Hb levels were associated with the SCD-SS children from rural as well as urban areas of Wardha district and indicated their mean hemoglobin levels to be 7.8 ± 0.2 and 9.1 ± 0.4 g/dl, respectively. From this result, it is evident that SCD-SS children from both the regions need additional nutritional supplements, such as vitamins [folic acid, vitamin B (12), and vitamin B (6)]. However, it is interesting to note that the comparative assessment between SCD-SS indicated that the children from rural area had significantly (P < 0.0.5) lower Hb than those from the urban areas. Similar results were observed with other parameters, such as weight, BMI, hematocrit, and WBC. Though the physical growth of SCD children could be maintained at normal levels through repeated transfusions, however, this may not be a sustainable therapeutic measure, especially due to transfusion reactions. The BMI is a good indicator of nutritional status, and the study results indicate that the children from rural as well as urban areas have less than desired, i.e., 18.5. [14] Hence, it would be more fruitful to carry out studies than can pin-point the specific causes for inadequate nutrition and the primary causes associated for under nutrition, which is reflected in low body weight as well as BMI. Although similar results have been reported elsewhere, [15] however, the identification of the cause is not mentioned in the published literature. In conclusion, this study highlights the need for conducting a more comprehensive study by integrating the clinical, nutritional, and social aspects to determine the cause and effect on relationships between various factors associated with SCD. Besides, a dedicated monitoring programme for assessing hematological parameters of SCD-SS needs to be initiated for effective management. Education for patients with SCD should focus on specific food intake which can increase the nutritional value through various foods. Acknowledgement We authors are thankful to PG Department of Microbiology, R.T.M. Nagpur University, Nagpur, India. References
Copyright 2012 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg12006t1.jpg] |
| |||||||||


{kind=link}