 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Human Genetics, Vol. 18, No. 1, January-April, 2012, pp. 66-70 Karyotypic findings in chronic myeloid leukemia cases undergoing treatment Anupam Kaur1, Simran Preet Kaur1, Amarjit Singh2, Jai Rup Singh3 1 Centre for Genetic Disorders, Guru Nanak Dev University, Amritsar, India Code Number: hg12011 DOI: 10.4103/0971-6866.96654 Abstract Background: Chronic myeloid leukemia (CML) is a clonal myeloproliferative expansion of primitive hematopoietic progenitor cells.
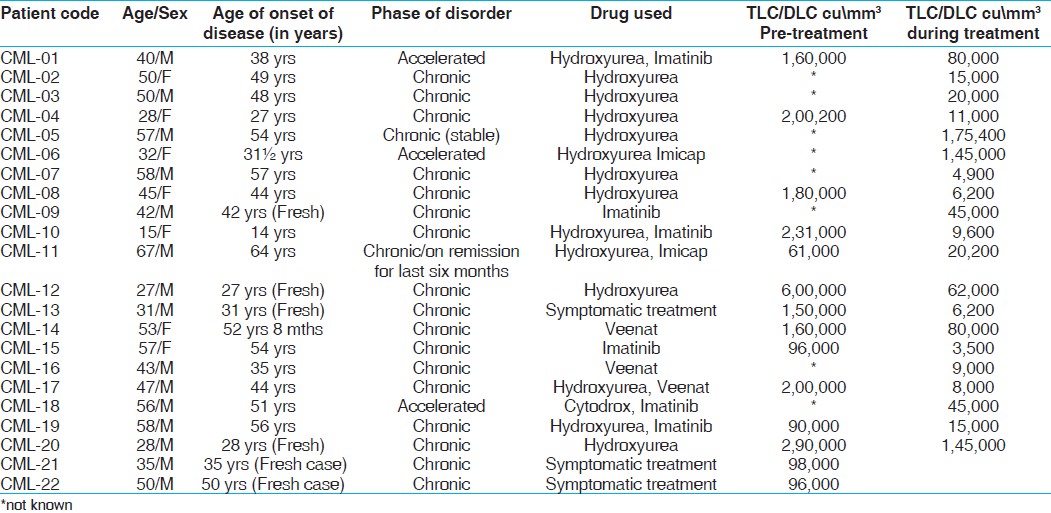
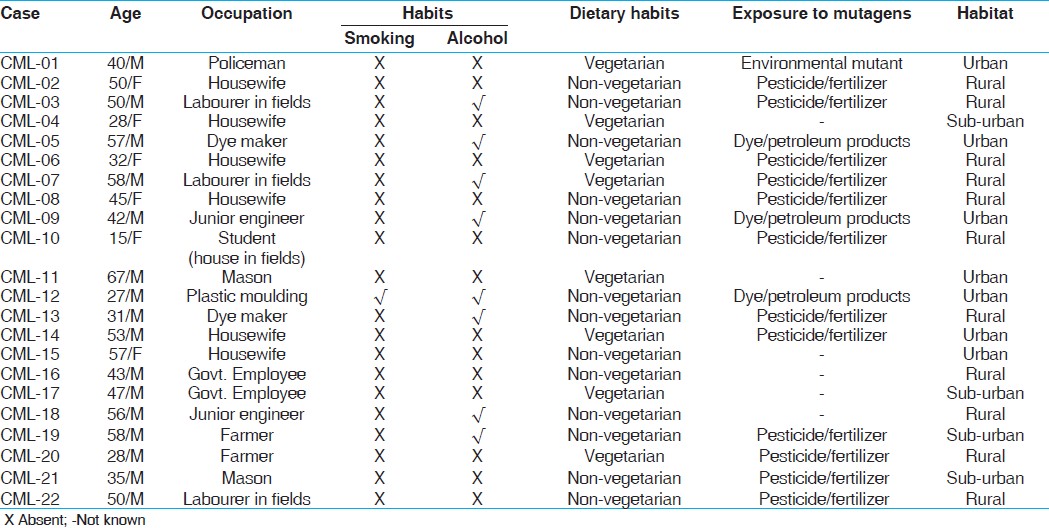
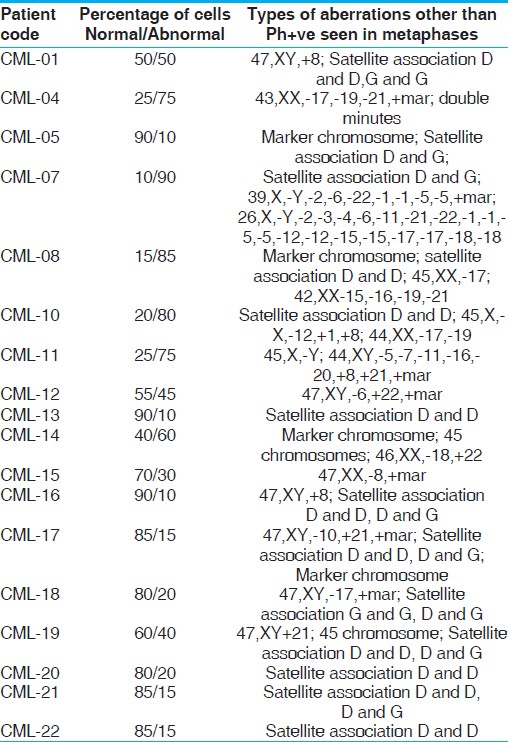
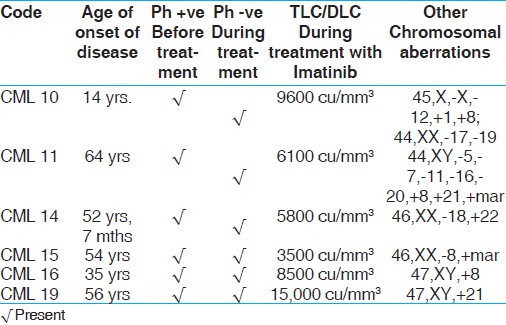
Keywords: Imatinib, myeloid leukemia, philadelphia chromosome Introduction Chronic myeloid leukemia (CML) is a clonal myeloproliferative (clone of multiplicating bone marrow cells) expansion of primitive hematopoietic progenitor cells involving myeloid, erythroid, megakaryocytic, B-lymphoid, and occasionally T-lymphoid lineages. CML was the first human disease in which specific abnormality of the karyotype the Philadelphia (Ph) chromosome could be linked to pathogenetic events of leukemia. The Ph chromosome is a shortened chromosome 22 resulting from a reciprocal translocation, t(9;22) (q34;q11). [1] CML has an incidence of 1-2/100000 people per year and accounts for 15% of the total leukemias occurring in adults. [2] Leukemia can be caused by ionizing radiations, radium, X-ray, cobalt, asbestos, use of permanent dyes, carcinogenic drugs, improper nutrition, deficiency of micronutrients like folic acid, vitamins B12, and B6, etc. [1],[3]The present study was carried out to find out cytogenetic aberrations in 22 CML patients prior to any treatment and also those being treated with Imatinib mesylate, with Hydrea/Hydroxyurea or drugs in combination. Materials and Methods The cytogenetic investigations were undertaken in 22 individuals of chronic myeloid leukemia (15 males, 7 females) and 10 age and sex matched controls from various hospitals of Amritsar, Jalandhar and Ludhiana. The present study was carried out to find out cytogenetic aberrations in CML patients being treated with Imatinib mesylate, or Hydrea/Hydroxyurea and in patients prior to any treatment (fresh cases). Informed written consent was obtained prior to the investigations. The general information like name, age, sex, phase of disease, total leukocyte count, differential leukocyte count, duration of disease, eating habits, habitat, occupation and exposure to mutagens were recorded [Table - 1] and [Table - 2]. In all the cases, chromosome culturing from peripheral venous blood was done using RPMI1640 for standard chromosome investigations. [4] The lymphocytes were treated with 0.075 M KCl at room temperature for 12 minutes and fixed with Carnoy's fixative (1 part glacial acetic acid and 3 parts methanol). Air dried and aged slides were GTG banded. Fifty well spread metaphases with relatively elongated G banded chromosomes were studied for each case and controls under the microscope. Ten metaphases from each case and control were karyotyped using automated karyotyping system (Cytovision, Applied Imaging).Results and Discussion The incidence of CML rises slowly with age until the mid forties when it starts to rise more rapidly, resulting in a median age of sixty years at diagnosis. There is no geographical or ethnic background that predisposes to CML. In the present study, age group of patients was between 14 and 67 years. The age of onset of disease in males was between 27 and 67 years and in females was between 14 and 57 years. One patient was a case of juvenile CML with the age of 14 years. Out of the 22 patients, 19 patients were in chronic phase of CML and 3 were in accelerated phase. These cases were under treatment with imatinib mesylate, Hydrea/Hydroxyurea, drugs in combination and three on symptomatic drug treatment [Table - 1].Out of 22 patients, good quality metaphases were observed in 18 cases. Metaphases were analyzed and no aberrations were seen in control samples. In the present study six cases (27.2%) were studied before any treatment. They were Ph+ve before the treatment and during a follow-up study (1-3 years of treatment with imatinib mesylate) they were Ph-ve but showed number of other chromosomal aberrations [Table - 3] and [Table - 4]. In our study, six fresh cases (CML-09, 12, 13, 20-22) were Ph-ve [Table - 1]. In patients with leukemia, increased percentage of aberrant cells, chromosomal aberrations like satellite association, double minutes, loss of chromosomes, monosomy, trisomy of various chromosomes and presence of marker chromosome were seen [Table - 3]. Satellite associations were present in half of the cases and are an indicator of tendency of the acrocentric chromosomes to be involved in Robertsonian translocation. No aberrations were observed in age- and sex-related control samples. In a similar report, among the 164 reported cases, 53 (32.3%) showed a normal karyotype, while in 111 (67.7%) abnormal cases, 96 cases (86.5%) showed the presence of Ph chromosome with translocation t(9;22); Ph+ve along with secondary aberrations was detected in 9 (8.1%) cases. Variants of Ph chromosome were detected in only one case (0.9%). Ph-ve CML with other chromosomal aberrations were detected in 5 (4.5%) cases, including +8, del 20q, del 11q and marker chromosome. [5] In present study, trisomy of chromosome 1, 8, 21, 22 were seen in 9 cases: CML 1, CML 10, CML 11, CML 12, CML 14, CML 16, CML 17 and CML 19. Trisomy 8, 21 and 22 were more common in these cases. Trisomy 8, loss of Y chromosome and abnormalities of chromosomes #5, #7 have been reported in literature. [6] As disease progresses from CML chronic to acute/blastic phase of myeloid or lymphoid phenotype, it is accompanied by recurring secondary chromosomal abnormalities such as +Ph, +8, +19, i(17q). These abnormalities occur as sole or in combination. Less common abnormalities are monosomy 7, monosomy 17, trisomy 21, t(3;21), loss of chromosome Y and patients with myeloid blast crisis frequently show occurrence of extra Ph, +8 and i(17q). [7] We observed monosomy of chromosome 17 in 3 cases CML 8, CML 10, and CML 18. Monosomy of chromosome 7 and 17 have been reported as secondary chromosomal abnormality which occur when disease progresses from chronic CML to acute/blastic phase of myeloid or lymphoid phenotype. [7] Other monosomies observed were of chromosome 1, 2, 3, 4, 5, 6, 7, 8, 10, 11, 15, 16, 19, 20, 21, 22 in the following cases CML 4, CML 7, CML 8, CML 10, CML 11, CML 12, CML 14, CML15, and CML 17 [Table - 3] and [Table - 4]. Loss of chromosome pair 1 and 5 was seen in 35% of the metaphases in CML 7. Loss of chromosome Y was observed in CML 7 and CML 11. Loss of Y chromosome has also been reported in patients with myeloid blast crisis. [7] In CML, loss of Y chromosome is generally considered as a secondary event of non-added clinical significance. Speculative loss of Y chromosome could provide a proliferative advantage because it tends to replicate late in ′S′ phase. Its loss might therefore shorten the cell cycle slightly. The chromosomal instability in the genome may be responsible for this secondary event. [8] Long term exposure to dyes, pesticides, herbicides, fertilizers increases the risk of developing leukemia. [9] In the present study, seven cases (31.8%) [Table - 2] had direct contact with fertilizers/pesticides/herbicides. A case of juvenile CML (CML 10) also had contact with pesticides/fertilizers due to their storage in the house. In the present study, 14 patients (59%) were non-vegetarian, which might lead to DNA damage and chromosomal breaks [Table - 2]. Hydroquinone mainly ingested from non-vegetarian diet is also known to cause DNA damage and leukemia. [10] In our study, CML 10 showed a large number of aberrations, i.e., loss of X chromosome, trisomy 1, 8 and monosomy 12, 17, 19 but was Ph-ve. The loss of X chromosome is due to evolution of malignant clone but how does it influence the malignant process is not known. It has been shown that age is not clearly related to the loss of X chromosome and X chromosome that are lost, reappeared after therapy and during clinical remission. [11] CML 11 showed trisomy 8 and 21, monosomy of chromosomes 5, 7, 11, 16, 20 and maker chromosome but no Ph+ve chromosome. CML 14, a bcr-abl positive case showed number of chromosomal aberrations other than Ph translocation. Monosomy 18 and trisomy 22 were seen in one patient. CML-15, showed a variable chromosomal constitution; there was monosomy of C group chromosome. CML 16, showed trisomy 8 in 10% of cells and 90% of cells had normal chromosomal constitution. CML 19 showed trisomy 21 in 40% of cells. All of these patients were in chronic phase of CML [Table - 4]. Similar observations were made by Karrman et al., [12] after allogeneic stem cell transplantation; major route abnormalities (i.e., +8, +Ph, i(17q), +19, +21, +17, and -7) were present. Information regarding the impact of specific types of additional cytogenetic abnormalities is still limited. Surprisingly, non-random karyotypic abnormalities have also been noted in the Ph-negative cells of some patients in cytogenetic remission. [13] It appears from [Table - 1] that Hydroxyurea and Imatinib both show encouraging results in reducing Ph count. Druker et al., [14] followed up five hundred fifty-three patients receiving Imatinib and same number of patients receiving interferon alpha plus cytarabine and their results showed best cytogenetic response in 69% of patients receiving Imatinib. Dutta et al., [15] investigated twenty patients receiving Imatinib mesylate therapy for hematological and cytogenetic responses and concluded that Imatinib mesylate showed better clinical activity in CML patients. Treatment of CML with Imatinib (Gleevec) induces a much higher rate of partial and complete cytogenetic response and in long-term follow-up studies it was associated with a single best complete cytogenetic response rate and survival rate. [16] Conventional wisdom suggests that elimination of the Ph +ve cells will lead to re-establishment of normal Ph-negative hematopoiesis but karyotypic abnormalities were detected in the Ph-negative cells of some patients treated with Imatinib. [17] The targeted therapy of CML with Imatinib favors the manifestation of Ph-clonal disorders in some patients [18] and it was indicated that patients on Imatinib should be followed with conventional cytogenetics even after induction of complete cytogenetic remission. High frequency of aberrations involving specific chromosomes in peripheral blood lymphocytes indicated that CML patients probably have chromosomal instability that arose due to effect of drugs on the patient. A systematic study of a larger patient cohort will be required. The chromosomal aberrations observed in our study are similar in all the patients either treated with Hydrea/Hydroxyurea or Imatinib mesylate. The availability of more advanced molecular techniques like fluorescent in situ hybridization (FISH) can be used as a supportive tool in CML diagnosis, even though it cannot fully replace the classical cytogenetics. References
Copyright 2012 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg12011t2.jpg] [hg12011t3.jpg] [hg12011t1.jpg] [hg12011t4.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}