 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Human Genetics, Vol. 18, No. 1, January-April, 2012, pp. 87-90 SRY sequence in maternal plasma: Implications for non-invasive prenatal diagnosis: First report from India Edna D'Souza, Sona Nair, Anita Nadkarni, Kanjaksha Ghosh, Roshan B Colah National Institute of Immunohaematology (ICMR), New Multistoried Building, K.E.M. Hospital Campus, Parel, Mumbai, India Code Number: hg12015 DOI: 10.4103/0971-6866.96661 Abstract Aim: The presence of circulatory cell-free fetal DNA in maternal plasma has found new applications in non-invasive risk-free prenatal diagnosis.
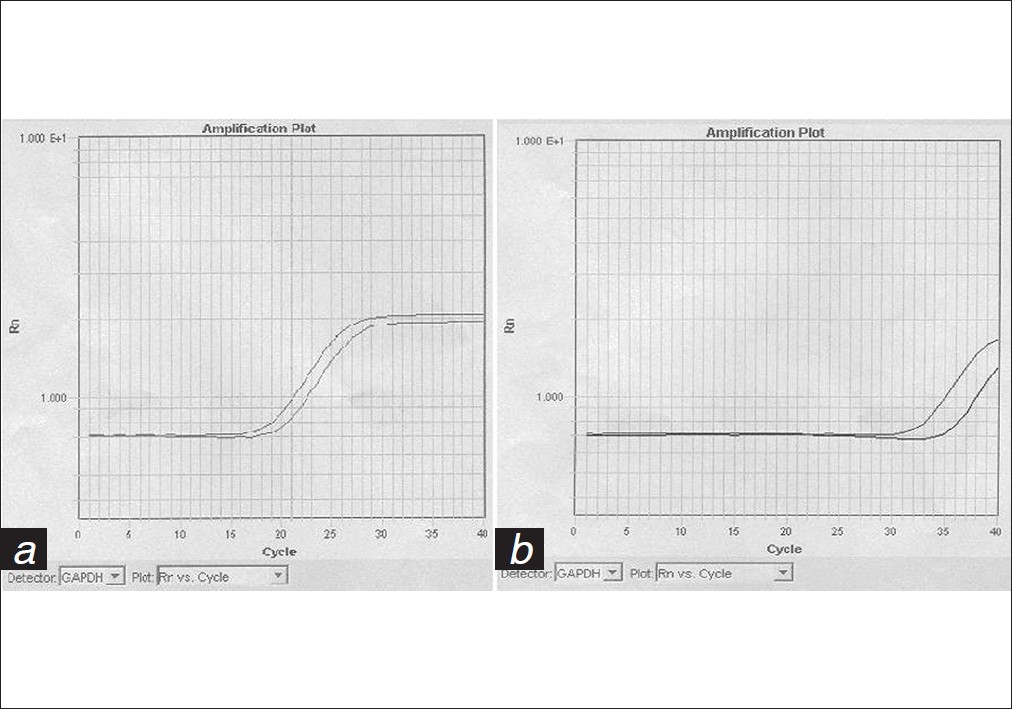
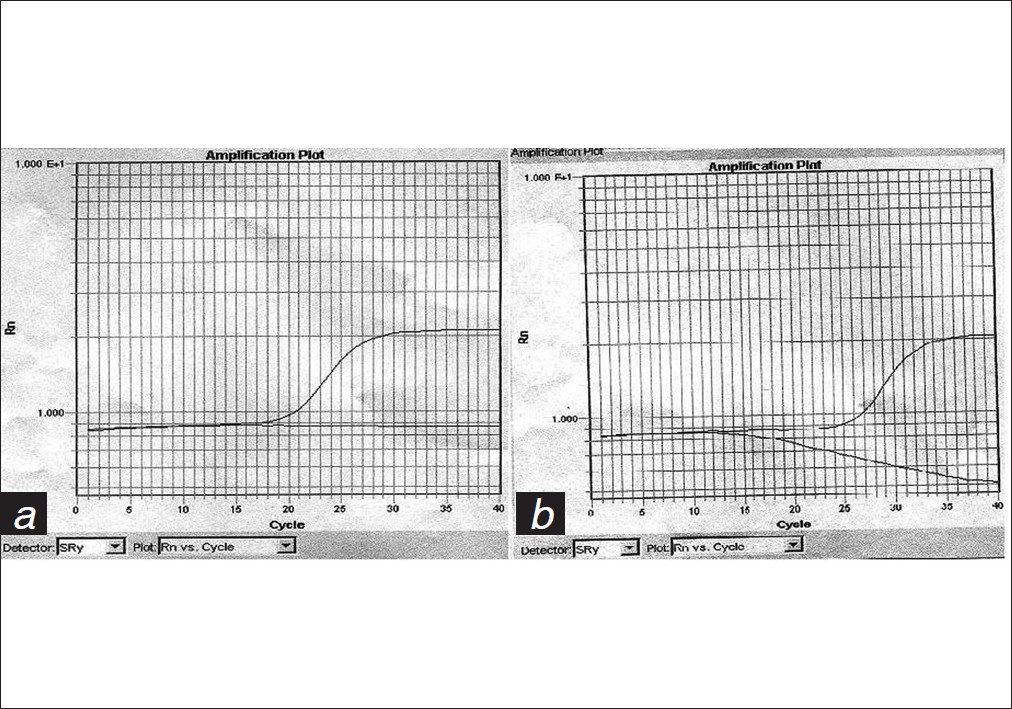
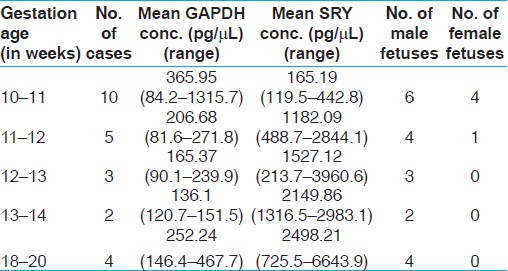
Keywords: Circulatory cell-free DNA, maternal blood, non-invasive prenatal diagnosis, real time PCR, Y chromosome Introduction With the evidence that fetal cells circulate in maternal blood, the roots of which were laid down by Schmorl et al., researchers began using these cells as a tool for non-invasive prenatal diagnosis. Of the various cell types studied, trophoblasts, lymphocytes and granulocytes and nucleated erythrocytes, the latter were found to be the most feasible. However, the numbers of fetal cells circulating are small in number and, for diagnosis, one would require to develop labor-intensive enrichment, isolation and mutation identification techniques. [1] Thus, in the hunt for a simple yet robust technique, it was in the 1990s that the focus was shifted from nucleated fetal cells to circulatory cell-free DNA in the maternal plasma or serum. The first milestone was achieved by Lo et al., when they showed the presence of Y chromosomal sequences in the plasma of pregnant women with male fetuses. [2] Since then, various groups have explored the possibilities of utilizing this circulatory fetal DNA for non-invasive diagnosis of various disorders like fetal sex identification, Rh D status determination, [3] congenital adrenal hyperplasia, [4] achondroplasia, [5] Huntington disease [6] and others. In an attempt to detect cell-free DNA in maternal plasma, we used a real time polymerase chain reaction (PCR)-based approach to detect the SRY sequence in the plasma samples, which would be truly of fetal origin. This approach has never been tried earlier in an Indian set up and we wanted to see if the results generated would help benefit the women who have to undergo the invasive procedures for prenatal diagnosis of sex-related genetic disorders. Materials and Methods The study was conducted at the National Institute of Immunohaematology, Mumbai, where couples were referred for invasive prenatal diagnosis for β-thalassemia and hemoglobinopathies like sickle cell anemia and Hb E-β thalassemia. Five milliliters of maternal peripheral venous blood sample in EDTA was drawn for the analysis from 30 women following which the invasive procedures were performed. The sex of the fetus was not known at the time of blood sampling. Informed consent of the couple was obtained. Sample processing The sample was taken in Eppendorf tubes and spun at 1600 g for 10 min in a microcentrifuge. The plasma was separated and respun at 16000 g for 10 min. Care was taken to see that no cells or buffy coat were aspirated along with the sample. The samples were stored at -20°C until being used further. Size separation approach Eight hundred microliters of plasma was thawed before use to extract the DNA using the Qiagen Blood Mini Kit Qiagen, Valencia, CA, USA according to the manufacturer′s instructions. The DNA was taken in 50 μl AE buffer. To ensure that we picked up fetal DNA, we used a size separation approach. Here, the entire DNA sample was loaded on a 1% agarose gel along side a 100 bp ladder and run at 80 V for about 90 min. Using a sterile scalpel, the gel slice of 300 bp or less was excised and the DNA was reextracted using the Qiagen Gel Extraction Kit Qiagen, Valencia, CA, USA. The sample was extracted using the manufacturer′s instructions and dissolved in 30 μl EB buffer. [7] Real time PCR The PCR was performed using the Real time 7900 HT PCR system (Applied Biosystem, Foster City, CA, USA). The PCR reaction was based on the TaqMan Chemistry. Here, we made use of two most commonly used sequences; one the sex-determining Region Y (SRY) sequence and the other glyceraldehyde 3-phosphate dehydrogenase (GAPDH). As is the requirement of TaqMan Chemistry along with the primers, the fluorescent-labeled probes were also synthesized (Applied Biosystem) [Table - 1]. The primer probe mix was prepared using 300 nm of primer and 200 nm of the probe. The PCR reaction was performed in a 20-μl reaction mix containing 10 μl 2 X TaqMan Universal master mix (Applied Biosystem), 1 μl each of the primer probe mix, 5 μl distilled water (RNase free) and 4 μl of the plasma DNA. This was set up for both GAPDH and SRY. The samples were run in duplicate. The PCR programme used was 95°C for 10 min, 40 cycles of 95C for 15 s and 60°C for 1 min. For the standard calibration curve, we used a human control genomic DNA of 10 ng/μl and made a double dilution of 5 points each for GAPDH and SRY. The dilutions were 10000 pg, 1000 pg, 500 pg, 250 pg and 125 pg. Along with the control sample, we ran positive controls - known as male genomic DNA - and negative controls - known as female genomic DNA - and control without the template. Along with these, we screened 24 plasma DNA samples. Ethical clearance The study was approved by the ethics committee of the Institute. Informed consent was taken from the couples and the sex of the child was not revealed as per the prenatal diagnostic techniques act of 1994 of the Government of India. Results Of the 30 women screened in this study, only six women were in their second trimester of pregnancy (gestation age of 14-20 weeks). The other 24 women were in their first trimester, with a gestational age of 10-12 weeks. We used GAPDH as an endogenous control to check the quality of the DNA sample to assess the PCR efficiency. When there was no amplification in the GAPDH reaction, the samples were not included in the study. There were six such samples where there was no amplification, and these were not used in further analysis. [Figure - 1]a and b shows the amplification for GAPDH in the human genomic male and female DNA control samples and two maternal plasma DNA samples; one carrying a male and the other carrying a female fetus. As is evident due to the lower concentrations of DNA in the plasma DNA samples, the amplification occurs late and hence a comparatively higher Ct value is obtained. To detect whether we obtained correct results with regards to the sex of the fetus, we acquired the information from the follow-up data sent to our Institute on the birth of the child. Of the 24 fetuses, 19 were males and five were females. These results were consistent with the findings from our SRY PCR reaction too. Thus, the real time PCR reaction for SRY sequence gave us 100% accurate results in the samples where we could obtain significant levels of DNA for analysis. However, considering all the 30 cases, the diagnosis was accurate in only 24 cases and hence the accuracy would be 80%. The results of the controls and plasma DNA samples are shown in [Figure - 2]a and b. As is evident, there will be no amplification in the sample where the woman is carrying a female fetus. The calibration curve was constructed on the basis of the concentrations of the human genomic control DNA. Two calibration curves were made, one for GAPDH and the other for SRY, and the concentrations for the 24 plasma DNA samples were calculated. The GAPDH concentration ranged from 81 to 1315 pg/μL. The mean concentrations of GAPDH and SRY at each gestation age are shown in [Table - 2]. We observed that there was a steady increase in the concentrations of the SRY product with increasing gestational age. The mean concentration ranged from 164 to 2498 pg/μL, which indicates that the increase from 10 weeks to 20 weeks is nearly 15-fold. Discussion Real time PCR is a technique with a very high sensitivity and accuracy. Lo et al. have stated that detection of a single copy of the Y-chromosome can be done in a surrounding population of 12,800 female cells. [6] Apart from SRY, there are several Y chromosome-specific sequences, e.g. DYZ1, DYZ3, DYS14, amelogenin-like gene on Y (AMELY), zinc finger protein Y encoded (ZFY), etc. Cell-free fetal DNA has been shown to have a half-life of less than 30 min post-partum in maternal plasma. In women carrying female fetuses, having a previous male child, no SRY amplification was detected by Lo et al., implicating the usefulness of cell-free DNA as a tool for non-invasive prenatal diagnosis. [6] Using cell-free fetal DNA from maternal plasma, we have been able to show an 80% accuracy in the detection of the sex of the fetus. These results were obtained on taking a lot of precautions. For the separation of the fetal DNA using the size separation approach, we made use of sterile scalpels. Only one sample was run per gel. The buffer was replaced following every sample. The setting up of the entire PCR reaction was carried out in a separate area. Aerosol-resistant sterile filter tips were used. Extreme care was taken while loading the sample in the 96-well plate; also, the plate was covered with an optical adhesive that prevented any carry over contamination. We also ran control samples without template during the analysis to check for non-specific amplification. We observed an increase in the concentration of the fetal DNA with an increase in the gestation age. Our results show that for up to 11 weeks, the mean concentration of the SRY product was 164 pg/μL and by the 20 th week there was nearly a 15-fold increase in the concentration of fetal DNA. Although there has been no specific data to explain this phenomenon, it is postulated that as the gestation age increases the contact at the fetomaternal interphase increases. Also, apoptosis of fetal cells circulating in the maternal blood leads to an increase in the liberation of cell-free DNA. [8] The presence of cell-free fetal DNA in maternal plasma opens up a new avenue in non-invasive prenatal diagnosis. The use in detection of the sex of the fetus as early as 9 weeks can avoid all the complications associated with the invasive procedures. [8] For sex-linked disorders, in a marriage between a carrier mother and a normal father, there is a 50% chance that the male child will be affected with the disorder or be born a carrier whereas a female child will only be a carrier or be completely normal. Hence, for this couple, prenatal diagnosis will not be required if the fetus is a female. Thus, non-invasive sex determination is very useful for X-linked disorders like hemophilia, where the females are carriers and the males are affected with the disease. Thus, in a pregnancy where the fetus is at risk of hemophilia, there will be no need of an invasive procedure if the fetus is a female. Using non-invasive diagnosis to detect the sex of the fetus even before the completion of the first trimester will reduce the number of invasive procedures drastically. In autosomal-recessive disease like congenital adrenal hyperplasia, intrauterine detection of fetal sex could help in the initiation of early treatment with dexamethasone. [4] Apart from its usefulness in sex-linked disorders, today, cell-free fetal DNA has found its application in the RhD status determination, detection of trisomy 21, pre-eclampsia, etc. The size separation approach has been shown to be useful in detecting autosomal-recessive disorders like β thalassemia. [7] This is the first study in India for non-invasive detection of the sex of the fetus from maternal plasma using real time PCR. The applications of using cell-free fetal DNA is not restricted to a particular genetic disorder. A non-invasive prenatal sex determination procedure will help reduce the numbers of invasive procedures to nearly half the number in X-linked disorders and also the risk of fetal loss (up to 2%) associated with the invasive procedures will be highly reduced. Thus, the scope of cell-free fetal DNA as a non-invasive tool is tremendous. References
Copyright 2012 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg12015t1.jpg] [hg12015f1.jpg] [hg12015t2.jpg] [hg12015f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}