 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
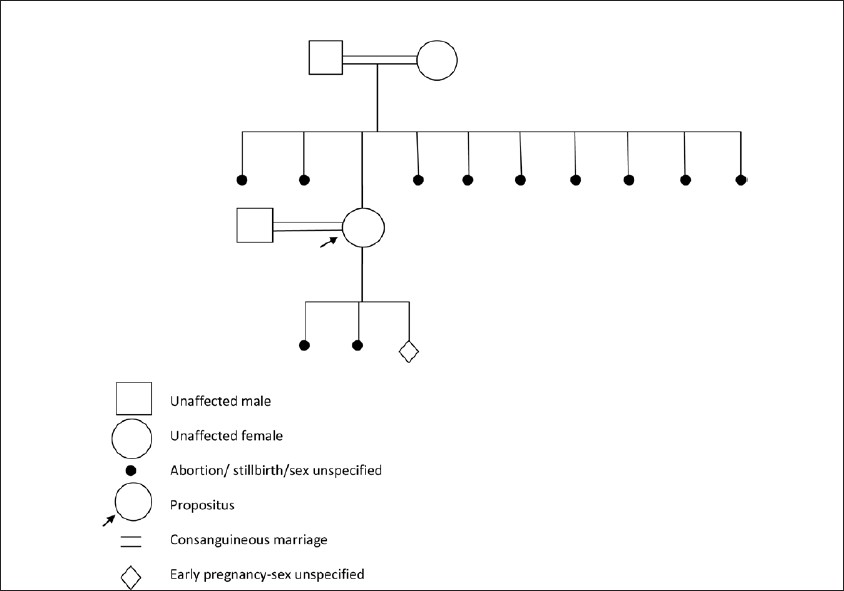
Indian Journal of Human Genetics, Vol. 18, No. 1, January-April, 2012, pp. 122-124 Methylenetetrahydrofolate reductase mutations, a genetic cause for familial recurrent neural tube defects Laxmi V Yaliwal, Rathnamala M Desai Department of Obstetrics and Gynaecology, SDM College of Medical Sciences and Hospital, Dharwad, Karnataka, India Code Number: hg12024 DOI: 10.4103/0971-6866.96680 Abstract Methylenetetrahydrofolate reductase (MTHFR) gene mutations have been implicated as risk factors for neural tube defects (NTDs). The best-characterized MTHFR genetic mutation 677C→T is associated with a 2-4 fold increased risk of NTD if patient is homozygous for this mutation. This risk factor is modulated by folate levels in the body. A second mutation in the MTHFR gene is an A→C transition at position 1298. The 1298A→C mutation is also a risk factor for NTD, but with a smaller relative risk than 677C→T mutation. Under conditions of low folate intake or high folate requirements, such as pregnancy, this mutation could become of clinical importance. We present a case report with MTHFR genetic mutation, who presented with recurrent familial pregnancy losses due to anencephaly/NTDs. Keywords: Folate, methylenetetrahydrofolate reductase gene mutation, neural tube defects Introduction Congenital malformations are the leading cause of infant mortality in developing countries and a major cause of health problems in surviving children. Neural tube defects (NTDs) are common group of central nervous system anomalies affecting 0.5-2 per 1000 pregnancies worldwide. [1] Despite the high prevalence and traumatic consequences for affected individuals and their families, causes of NTD are poorly understood. Identification of the causative factors is confounded by the fact that the majority of these malformations appear to result from a combination of genetic and environmental factors. A strong genetic component is indicated by the high recurrence risk for siblings of affected individuals. [2] Methylenetetrahydrofolate reductase (MTHFR) mutations are commonly associated with hyperhomocysteinemia. Through defects in homocysteine metabolism, they have been implicated as risk factors for NTDs and unexplained recurrent embryo losses in early pregnancy. Folate sufficiency is thought to play an integral role in phenotypic expression of MTHFR mutations. [3] The best-characterized MTHFR genetic polymorphism is a common missense mutation consisting of 677C→T transition, resulting in thermolabile enzyme variant that has reduced catalytic activity. [4] Another common genetic polymorphism of MTHFR is a missense mutation consisting of nucleotide 1298A→C transition, resulting in decreased MTHFR activity, which is more pronounced in homozygous than heterozygous state. [5]Case Report A 19-year-old lady, gravida - 3, abortion - 2 with history of 2 months amenorrhoea presented to our obstetric outpatient department. She had a consanguineous marriage, married to her maternal uncle. Her past obstetric history revealed that both of her previous pregnancies were terminated during early second trimester in the view of anencephaly.It was interesting to note from patient′s family history that her mother also had consanguineous marriage, married to her maternal uncle. She had nine pregnancy losses due to anencephaly/NTDs as shown in the family pedigree chart [Figure - 1]. Patient and her husband were referred to a geneticist and were subjected to gene mutation studies, karyotyping, and biochemical analysis. Karyotyping of both the partners were normal. Genotypes of MTHFR gene were isolated and determined. Genotype of patient was identified to have CC and CC genotypes, suggesting a wild status at 677 and homozygous mutant status at 1298, respectively, of the MTHFR gene. Genotype of husband was identified to have CT and AA, suggesting a heterozygous status at 677 and wild status at 1298, respectively, of the MTHFR gene. Patient′s biochemical analysis revealed:
Discussion MTHFR is essential for homocysteine metabolism. Mutations in MTHFR and other genes associated with homocysteine metabolism have been reported as causes of hyperhomocysteinemia. [4] Folate deficiency remains the primary cause of hyperhomocysteinemia. MTHFR gene mutation are by far the most common etiology of mild to moderate form of hyperhomocysteinemia. [3]Homozygocity for the common 677C→T mutation, which produces an alanine to valine amino acid substitution within the predicted catalytic domain of MTHFR enzyme causing thermolability of the enzyme, is a risk factor for NTDs. Folate acts to stabilize this thermolabile enzyme. Homozygosity for thermolabile MTHFR variant predisposes individuals to development of hyperhomocysteinemia, especially during times of folate insufficiency. [4],[5] Another mutation in the same gene, the 1298A→C mutation which changes a glutamate into alanine residue. This mutation destroys an MboII recognition site, results in decreased MTHFR activity, which is more pronounced in the homozygous than heterozygous state. Neither the homozygous nor the heterozygous state is associated with higher plasma homocysteine or a lower plasma folate concentration, phenomena that are evident with homozygosity for 677C→T mutation. However, there appears to be an interaction between these two mutations. When compared with heterozygosity for either the 677C→T or 1298A→C mutations, the combined heterozygosity for the 1298A→C and 677C→T mutations was associated with reduced MTHFR specific activity, higher homocysteine levels and decreases plasma folate levels. Combined heterozygosity for both MTHFR mutations results in similar features as observed in homozygotes for 677C→T mutation. [5] Elevated plasma homocysteine levels are present in mothers of children with NTDs. [5] Several studies have shown that folate levels in mothers of children with NTDs are not deficient but are in the lower range of control levels. [5],[6] 1298A→C mutation is also a risk factor for NTDs, but with a smaller relative risk than the 677C→T mutation. Indeed, the frequency of the 1298A→C mutation in NTD-affected children tended to be increased, which also suggests that this mutation is a genetic risk factor for this developmental anomaly. Especially under conditions of low intake of folates or during high requirements of folate, like pregnancy, this mutation could become of clinical importance. [5] By analyzing the frequency distribution of the 677TT and 677CT/1298AC genotypes among NTD patients and their mothers, the protective role of folate in the etiology of NTD is 36%-50%. In order to obtain high enough methylenetetrahydrofolate levels for an adequate homocysteine metabolism, individuals with a decreased MTHFR activity obviously need a higher dietary intake of folate. [5] Several studies have pointed out that folate intake high enough to prevent NTDs cannot be achieved by a diet of folate nutrition. [7] Only intake of folate supplements or fortified foods such as flour and cereals can achieve these daily recommended values. [5] Since periconceptional folate administration reduces the risk for NTD for >72%, [8] there may still be other defective genes present in the folate, vitamin- B12, or homocysteine metabolism associated with an increased risk of NTD offspring. Acknowledgement We thank the geneticist Dr. Shridevi Hegde, Ph.D. (Genetics), and Centre for Cellular and Molecular Biology, Hyderabad, for the gene mutation studies, karyotyping, and biochemical analysis.References
Copyright 2012 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg12024f1.jpg] |
| |||||||||

{kind=link}