 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
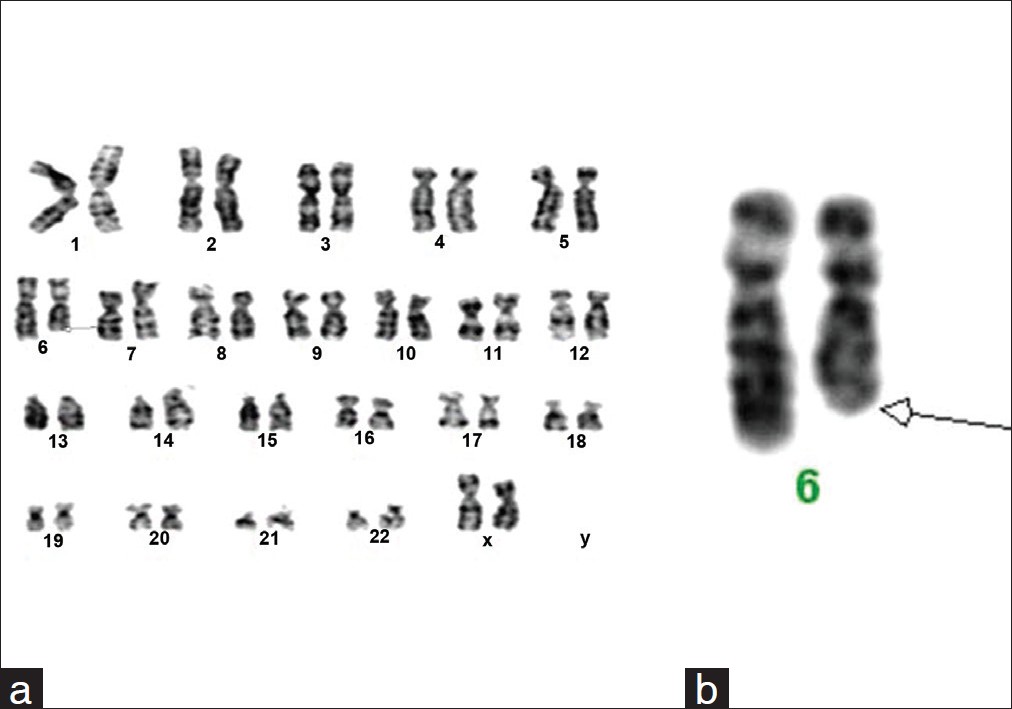
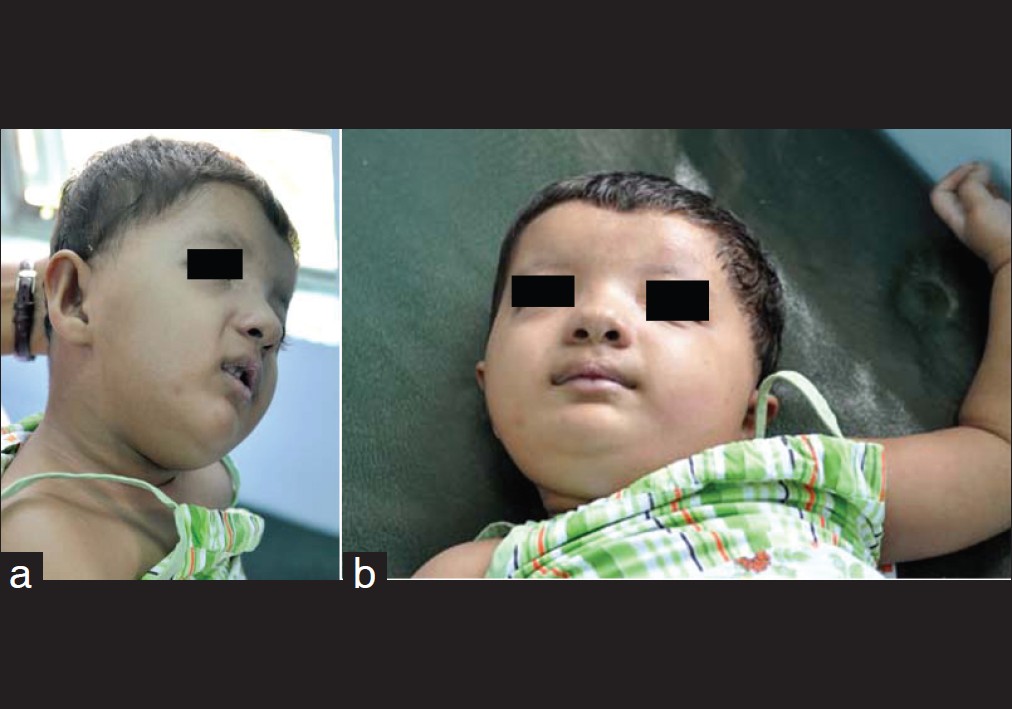
Indian Journal of Human Genetics, Vol. 18, No. 1, January-April, 2012, pp. 127-129 Dysmorphic features and congenital heart disease in chromosome 6q deletion: A short report Sreelata Nair, Rini Varghese, Sajeed Hashim, Pappachan Scariah Department of Fetal Medicine, Lifeline Genetics and Research Centre, Lifeline Super Specialty Hospital, Adoor, Pathanamthitta, Kerala, India Code Number: hg12026 DOI: 10.4103/0971-6866.96682 Abstract In this report, we describe a one and a half year old girl showing terminal deletion of long arm of chromosome 6q. The associated abnormalities such as congenital heart disease, mental retardation, and dysmorphic features are described. Cytogenetic studies with GTG banding showed 46,XX,del(6)(q24→qter). Karyotype of the parents was normal suggesting a denovo event. Keywords: Chromosome, deletion, dysmorphism, genetic counseling, karyotype Introduction Chromosomal deletions may arise denovo as well as from unbalanced translocations. Denovo deletions may affect the terminal part of a chromosome or an interstitial region, and usually affect a fairly large number of genes and produce recognizable syndromes. Microscopically visible deletions generally involve multiple genes, and the consequences of losing this much genetic material from even one of the chromosome pair can be severe. [1] If the missing part contains important instructions, it can lead to congenital malformations, development delay, or mental retardation.Case Report A one and a half year old girl child born of non-consanguineous marriage to a 27-year-old primi mother was referred to the genetic clinic. The child was born at term by elective cesarean section because of symmetric IUGR and oligohydramnios. Birth weight was 2.0 kg and length was 48 cm with head circumference 30 cm. The baby was admitted to NICU in view of respiratory distress soon after birth. There was no significant family history, no evidence of teratogenecity, and no other pregnancy associated complications.Clinical examination of the new born revealed grade 3 pansystolic murmurs in the left lower sternal border. ECHO was suggestive of congenital acyanotic heart disease VSD, ASD, PDA with moderately severe pulmonary hypertension. USG abdomen was normal. The first genetic consultation was at the age of 1 year 6 months for dysmorphic features and congenital heart disease. Facial dysmorphism included microcephaly, brachycephaly, hypertelorism, upslanting palpebral fissures, strabismus, broad nasal bridge, wide anterior fontanalle, anteverted nares, high arched palate, microretrognathia, low set dysmorphic ears, and short neck. Clitoromegaly with prominent labia minora was seen. Congenital acyanotic heart disease with vsd,0 ASD, and pda0 was noted. Pallor was seen along with cyanosis and nail bed clubbing of the finger and toes. Psychomotor development was extremely delayed and marked hypotonia was seen. MRI (brain) showed partial agenesis of corpus callosum, bilateral mildly enlarged subarchanoid space, and mildly dilated third and lateral ventricles. Cytogenetic findings Cytogenetic analysis from the proband was carried out by peripheral blood lymphocyte culture [2] and GTG banding. Twenty metaphase were analyzed after GTG banding at 500 band resolution. Karyotype of the proband showed deletion in the terminal region of the long arm of chromosome 6 in all the metaphase analyzed. The karyotype of the child was 46,XX,del(6)(q24→qter) [Figure - 1]a and b. Discussion Here, we describe a case with deletion in the terminal region of long arm of chromosome 6 with break point at q 24 region. Chromosome 6q deletion is associated with dysmorphic features and multiple anomalies, which were seen in the index case also. The more frequently observed clinical features in 6q deletion are congenital heart defects, [3] which were also seen in our case. The child had VSD, ASD, and PDA with moderately severe pulmonary hypertension. Other features like brachydactyly, clinodactyly along with peripheral clubbing and cyanosis were also seen [Figure - 2]a, b and [Figure - 3]. Literature search with chromosome 6q24 deletion showed few reports with varying other anomalies like nuchal cyst, diaphragmatic hernia, multicystic kidney, etc, which was not seen in our case. [4],[5] Caselli et al., [6] have reported a similar case with deletion of 6q24.3-25.1 in an 8-year-old with growth failure, cardiac septal defects, mental retardation, and dysmorphic features.The region involved in our case is q24 to terminal and therefore explains the neurodevelopmental delay and peculiar facial features. This critical region has a 2.6 Mb deletion. More than twenty two genes are present in this deleted region, [6] which might be important in the normal development of cardiovascular and central nervous system. The karyotype of parents were normal, which further suggests that this must be a denovo event and not due to unbalanced product of familial translocation. As the parental karyotype was normal and the child had a denovo deletion, the chance of recurrence is very low. Nevertheless, prenatal diagnosis by amniocentesis and fetal karyotyping has been offered to the couple, in case of future pregnancies. Genetic counseling was given in detail. Hence, chromosome analysis should be offered to every child with mental retardation and dysmorphism as in this case. FISH studies and array-CGH analysis may be useful to delineate the size of the deletion and the genes involved, which in our case was not affordable by the patient. References
Copyright 2012 - Indian Journal of Human Genetics The following images related to this document are available:Photo images[hg12026f3.jpg] [hg12026f1.jpg] [hg12026f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}