 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 23, No. 1, March, 2005, pp. 6-15 Aetiology and Clinical Presentation of Pneumonia in Hospitalized and Outpatient Children in Northeast Brazil and Risk Factors for Severity Luis C. Nacul1; Betty R. Kirkwood1; Araci C. Carneiro2; Claudio S. Pannuti3; Marcelo Magalhaes4; Paul Arthur5; 1Department
of Epidemiology and Population Health, London School of Hygiene & Tropical
Medicine, London, 2St. George's NHS Trust, London, UK, 3Instituto de Medicina
Tropical de São Paulo, Departamento de Doenças Infecciosas, Faculdade de
Medicina da Universidade de São Paulo, São Paulo, 4Universidade Federal de
Pernambuco, Departmento de Microbiologia, Recife, Brazil, and 5Department
of Epidemiology and Population Health, London School of Hygiene & Tropical
Medicine, London, UK (in memoriam)
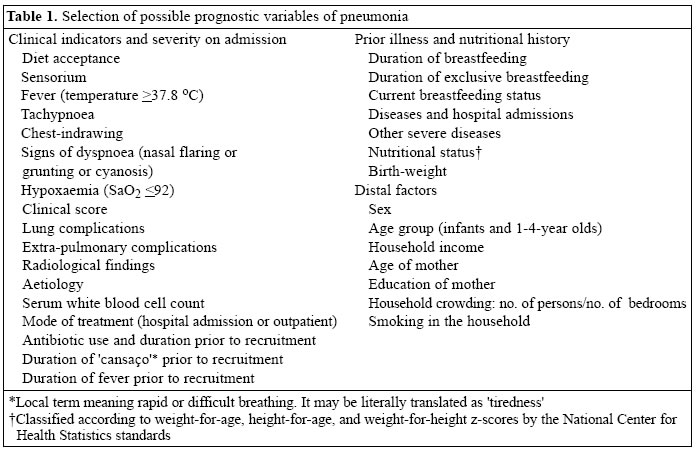
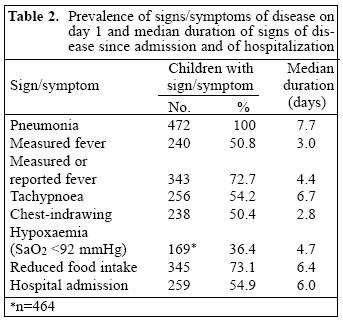
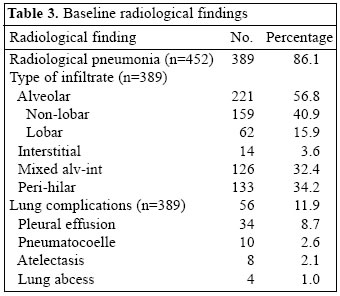
Code Number: hn05002 ABSTRACT Data on presentation, aetiology, and prognostic indicators of childhood pneumonia, which can help design strategies for controlling the disease, are generally scarce in developing countries. In this paper, the distribution of aetiologic agents, clinical presentation, and evolution of pneumonia cases are described, and the factors associated with duration of pneumonia episode and of hospital admission examined. During June 1994-June 1995, 472 children, aged 6-59 months, with clinical diagnosis of pneumonia, who were admitted to hospital or treated as outpatients, were investigated in Recife, Northeast Brazil. Pneumonia, in most cases, was confirmed by radiology. A combination of methods was used for investigating the aetiology of pneumonia. Data obtained on a large number of clinical, socioeconomic and biological variables were analyzed to determine the prognostic factors for the severity and outcome of pneumonia. Bacteria were identified in 26.7% of the cases, while viruses and mixed infections accounted for 8.4% and 2.7% respectively. Haemophilus influenzae (18.9%), Streptococcus pneumoniae (6.4%), and respiratory syncytial virus (5.0%) were most often identified. The pneumonia case-fatality rate was 0.8%. The best clinical predictors of severity were: lung complications at baseline, tachypnoea (for duration of episode), and chest-indrawing (for duration of hospital admission). Young age, low birth-weight, and prolonged fever prior to admission to the study also predicted a more prolonged illness, and under-nutrition was a predictor of longer hospital stay. While the development of new vaccines is an important measure for reducing morbidity and mortality due to pneumonia, emphasis on appropriate case management needs to be maintained, with particular attention to children who show the identified risk factors for a poor prognosis. Key words: Pneumonia; Haemophilus influenzae; Streptococcus pneumoniae; Epidemiology; Aetiology; Risk factors; Brazil Introduction Acute lower respiratory infections (ALRIs) are the main cause of mortality among children aged less than five years in developing countries, resulting in about 1.9 million deaths every year (1). Most of these deaths occur due to pneumonia (2). ALRIs are also a major cause of morbidity among children, resulting in a large proportion of clinic attendance and hospital admissions (3). The estimated median incidence rate of ALRIs is 0.45 episode per child per year in the developing world, although there is a considerable geographic variation in its occurrence (4). At present, appropriate case management, as part of integrated management of childhood illness (IMCI), is the cornerstone of the control of mortality due to pneumonia (5,6). Immunizations against measles, diphtheria, and pertussis and, more recently, against Haemophilus influenzae type b are also a recognized strategy for the prevention of ARI due to these causes. Data on aetiology, clinical presentation, and prognostic indicators of severity of pneumonia are relevant for designing and evaluating pneumonia-control strategies. Data on aetiology also enable more accurate modelling of the impact of new interventions, such as vaccines. However, there are few such data in developing countries. This report describes the clinical presentation and aetiology of pneumonia among 472 children admitted to or treated as outpatients at the Barão de Lucena Hospital, Recife, Northeast Brazil. This public hospital serves children mainly from the poor areas of the city. Pneumonia is the main cause of mortality among children aged 1-4 year(s) in Recife, and the estimated incidence rate is 0.26 episode per child per year (7). In this paper, we describe the distribution of aetiologic agents, clinical presentation, and evolution of pneumonia cases. We also examined the factors associated with duration of pneumonia episode and of hospital admission. Materials and Methods The study was conducted during June 1994-June 1995 as part of a randomized, double-blind, placebo-controlled trial of vitamin A in the treatment of childhood pneumonia; its detailed design has been described previously (8). In total, 472 consecutive children, aged 6-59 months, with clinically-diagnosed pneumonia, who were either admitted to or treated as outpatients at the study hospital, were included in the study. The study excluded children with clinical diagnoses of xerophthalmia, measles, septicaemia (with clear systemic organ involvement), meningitis, other active lung diseases, such as tuberculosis and asthma attacks, renal failure, and previous admission to hospital due to the current illness. Patients with bacteraemic pneumonia were included unless they had another criterion for exclusion. Children with wheezing were included only if lung involvement was confirmed by chest X-ray. Written consent was obtained from all participants. The ethical committees of the London School of Hygiene & Tropical Medicine and Barão de Lucena Hospital granted ethical clearance. Diagnosis and baseline evaluation The experienced study paediatricians diagnosed pneumonia based on history and clinical examination and by chest radiography, following the guidelines of Barão de Lucena Hospital (9). At admission, baseline data on a large number of clinical, socioeconomic and biological variables relating to the outcome of pneumonia were obtained. All children had a chest X-ray in the posterior-anterior position, which was read by an experienced study radiologist, according to the WHO guidelines (10). Blood samples of the hospitalized children were also collected for routine haematological tests. Aetiologic diagnosis Aetiology was investigated using a combination of procedures, which were applied on admission and before initiation of antibiotic treatment in the hospital. A positive result in any of the tests applied was considered diagnostic for that particular aetiology. Viral infections: Antigens for respiratory syncytial virus (RSV), influenza virus A and B, parainfluenza type 1, 2, and 3, and adenovirus were detected by direct immunofluorescence from nasopharyngeal swab (NPS) samples, employing commercial monoclonal antibodies conjugated with fluorescein isothiocyanate (IMAGEN, Dako, Denmark). A positive result was indicated by the finding of at least one cell showing a typical fluorescence pattern, provided that at least 20 respiratory cells were available in the sample. Bacterial infections: Diagnosis involved cultures of blood and pleural fluid when available and puncture clinically indicated. Positive cultures were identified using standard procedures (11). Antigen of H. influenzae type b and Streptococcus pneumoniae was detected by latex agglutination (Wellcogen, Murex Diagnostics, UK) from urine samples, after concentration of the urine with a disposable concentrator (Minicon B-15 concentrator, Amicon, USA). Development of a typical agglutination pattern within three minutes of mixing the latex with the sample, with lack of agglutination in the control latex, indicated a positive result for the latex agglutination test. Infections due to Chlamydia and Mycoplasma : A direct immunofluorescence test was employed to detect genus-specific Chlamydia antigen (IMAGEN Chlamydia, DAKO, Denmark) from NPS samples. The identification of positive results was similar to that for viruses. Serology for detection of antibody of Mycoplasma pneumoniae was performed by an indirect agglutination test (Serodia-Myco II, Fujirebio Inc, Japan). The serum samples were collected on admission to the study and 10 days later. A four-fold or larger increase in titre from the first to the second sample was considered diagnostic for acute infection due to Mycoplasma. Treatment of pneumonia All patients were treated according to the standard protocol of Barão de Lucena Hospital (9), which follows the current practices in the study area. Benzylpenicillin (100 mg/kg/day IV) and benzathine penicillin G (50,000 IU/kg IM at recruitment and repeated at day 3) were used as the first-line antibiotics in uncomplicated cases for inpatients and outpatients respectively. The main rationale for using benzathine penicillin was economic as most outpatients in this hospital cannot afford to buy antibiotics and would have a high risk of otherwise remaining untreated. This treatment scheme has been used locally with good results (Rodrigues R. Personal communication, 1994). Chloramphenicol (50 mg/kg/day IV [intravenous] or orally) was introduced, normally after 48 hours, in patients who failed to respond to the first-line antibiotics. Treatment failure was defined as persistence of fever and/or aggravation of the respiratory parameters or development of any complications. Other antibiotics were used as needed. Evaluation and follow-up of patients Patients were followed up daily for a minimum of 11 days, or until discharge when hospital admission lasted for longer than 11 days. The clinical evaluation focused on the observation of signs and symptoms of disease, severity, and occurrence of adverse outcomes. The study paediatricians made daily evaluation of all children during admission and evaluation of all outpatients on admission to the trial and on day 3 and 11. The trained field workers assessed children who were at home on any other days during the first 11 days of study, using a similar but simplified protocol. The field workers obtained temperature, respiration rate, weight and, by pulse oximetry, SaO2 in all cases. The study team carried out all the evaluations once daily, except that temperature was measured four times daily in patients admitted to the hospital. Fever was defined as a temperature equal to or greater than 37.8 oC, hypoxaemia as SaO2 equal to or under 92%, and tachypnoea by two respiratory-rate counts over 50 per minute in infants, and over 40 per minute in the 1-4-year olds. Nutritional status was assessed using the National Center for Health Statistics reference standards (12). Although half of the study children received vitamin A in addition to antibiotics, they were included in all analyses, since we found that vitamin A did not influence the evolution or outcome of pneumonia (8). Data analysis Data were double-entered and analyzed using the SPSS software version 5.0 (SPSS, USA). Potential prognostic variables (Table 1) were tested for associations with the outcomes (duration of pneumonia episode and of hospital admission) by univariate analysis and Cox's proportional hazards regression analysis (13). For univariate analysis, the prognostic variables were compared in respect to the outcome by chi-square test (14). For Cox's regression analysis, the variables were divided into three subgroups: those immediately related to the outcomes (i.e. present clinical condition, duration of symptoms until recruitment, and previous treatment), those related to the child's previous health, and distal factors, such as socioeconomic indicators. The variables in each subgroup, which were associated with the outcome using a cut-off point of p= 0.2, were included in the regression model; those whichremainedsignificant(p<0.05) were kept in the final model. The assumption of proportional hazards was checked by comparing plotted cumulative hazards functions against time for subjects in both the treatment groups (which should be reasonably parallel on a log scale) and by formally testing the heterogeneity of the treatment effect over equally-divided time periods. The duration of pneumonia was counted from the first evaluation (day 1) until the last day with symptoms/signs of pneumonia (with no recurrence for at least 48 hours), including tachypnoea, fever, and low oxygen saturation, and of any sign of severity or evidence of lung complications. Infants and children were divided into two age groups: infants (6-12 months) and 1-4-year olds. Quality control The quality of data was assured by extensive staff training, standardization of procedures, a three-week pilot study, regular checking of equipment, manual and computer checking of all assessments, blind repetition of assessments, and monitoring of comparability of data obtained from different observers. Blood and urine samples were sent to the laboratory as soon as possible after collection. The nearby reference laboratory, situated about four miles from the study hospital, was visited at least daily. Urine samples were kept refrigerated when not immediately sent to the laboratory and were always transported in thermal boxes with ice. For all tests conducted for aetiologic diagnosis, six healthy consenting children of the same age group (two infants and four 1-4-year olds), who attended the hospital without any infectious or respiratory disease in the previous two weeks, were used as controls. Members of the laboratory staff were not aware of their clinical status, and all tests on the controls yielded negative results. In the tests involving detection of antigen and serology, positive controls were tested whenever a new batch was opened. In addition, a randomly-selected number of duplicate slides was blindly resubmitted either to the Laboratory of Virology of the Institute of Tropical Medicine, São Paulo, or to the Laboratory of Virology of the Evandro Chagas Institute (Dr. Wyller, Belem, Brazil) or the Virology Laboratory of The Middlesex Hospital (Mr. Steve Rice, London, UK). RESULTS History and baseline clinical evaluation The median age of children recruited to the trial was 19 months. One hundred twenty-two (25.8%) infants were aged 6-12 months, and 350 (74.2%) children were aged 1-4 year(s). The typical child had been ill for a median period of six days and presented with a history of cough (98.9%) and fever (97.8%). 'Cansaço', a local term used by mothers to report respiratory distress, which may be literally translated as 'tiredness', was present in 84.6% of the children. The use of antibiotics for the current sickness episode before recruitment into the study was reported in 123 (27.2%) of 453 children. The median period of antibiotic use before recruitment to the study was three days. The main signs and symptoms present at baseline and their median duration are presented in Table 2. Most children (n=456, 96.6%) had cough on day 1. Nasal flaring, grunting, and cyanosis were present in 46 (9.7%), 42 (8.9%), and 3 (0.6%) children respectively. One hundred sixty-six (35.2%) children were found to be irritable when examined, while 15 (3.2%) had depressed sensorium. Three hundred and forty-three (72.7%) had fever, 133 (28.2%) vomiting, and 66 (14.0%) diarrhoea, and 58 (12.3%) were either refusing the diet or were prescribed nil by mouth. Ten (2.1%) were considered to be very severe by the study paediatrician. Extra-pulmonary findings, such as infections in sites other than the lungs, heart, and other organ failures, and 'seizures' were present in 79 (16.7%) patients. The sensitivity of tachypnoea for radiologically-confirmed pneumonia was 57.3% (54.2% for clinical pneumonia) and that of chestindrawing was 51.4% (50.4% for clinical pneumonia). The nutritional assessment showed, on average, negative z-scores. The mean z-scores for weight-for-height, height-for-age, and weight-for-age were -0.74, -0.71, and -1.09 respectively. The prevalence of children with z-scores under -2.0 was 55/409 (13.4%), 73/440 (16.6%), and 96/429 (22.4%) for weight-for-height, height-for-age, and weight-for-age respectively. Past health Hospital admission in the preceding 12 months was reported for 159 (33.8%) of 470 children, and previous admission due to pneumonia in the same period was reported for 78 (16.7%) of 466 children. One hundred eighteen children (n=464, 25.4%) had pneumonia in the preceding 12 months, and 182 children (n=472, 38.6%) reported previous asthma or recurrent wheezing (3 episodes or more in the previous 12 months, or since birth in infants). Chest radiology and laboratory findings The radiological findings on admission are presented
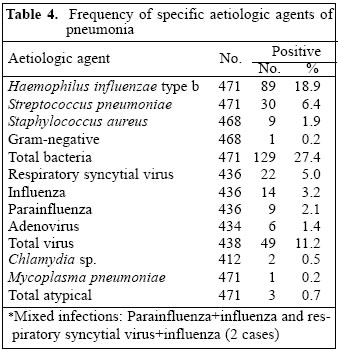
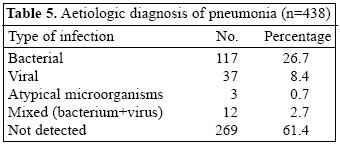
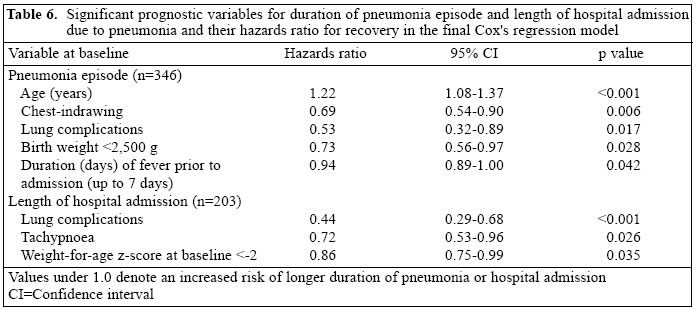
in Table 3. A confirmatory infiltrate on the chest X-ray was present in 389 (86.1%) of 452 patients and in 228 The routine haematological tests showed a median haematocrit of 28.3%. The haematocrit was under 30% in 132 (56.9%) of 232 patients. The median white cell count was 12,600*106/L. The count was under 6,000*106/L in 15 (6.5%) children, between 6,000 and 14,900*106/L in 122 (52.6%), and 15,000*106/L or over in 94 (40.5%) patients. Aetiology of pneumonia Bacterial pneumonia was investigated in 471 children; results of the latex agglutination test were not available for three of them, but only from blood culture. H. influenzae (18.9%) was the most common agent, followed by S. pneumoniae (6.4%). Of S. pneumoniae cases, 14 were diagnosed by latex agglutination, 4 by culture, and 12 by both culture and latex agglutination. All the cases of H. influenzae were diagnosed by latex agglutination. RSV (5.0%) and influenza (3.2%) were the viruses most frequently found (Table 4). Over half of the RSV cases occurred in winter (July-September), with over 35% of all the cases in August. Table 5 shows the results of aetiologic diagnosis according to categories of infectious agents (bacterial, viral, or mixed infections) obtained from 438 cases. Bacteria were responsible for most positive cases (26.7%), while viruses and mixed infections accounted for 8.4% and 2.7% of cases respectively. Chlamydia and Mycoplasma accounted for less than 1% of cases. Of those with viral or a typical infections, 79% had radiological abnormalities. Radiological pneumonia was present in 87% of cases of confirmed bacterial infections and in 90% of those with confirmed mixed infections (p=0.2). Outcome of illness and risk factors for severity Two hundred and fifty-nine (54.9%) children were initially admitted to the hospital. The episode of pneumonia lasted for a median of 7.7 days, and the hospitalized children remained admitted for a median of six days (Table 2). Fourteen (6.6%) of those initially treated as outpatients subsequently needed to be hospitalized. The study paediatrician who admitted the cases classified 289 (61.2%) patients as severe. One hundred and two (21.6%) patients did not respond to the firstline treatment and needed a change in the antibiotic scheme. New lung complications developed in eight (1.7%) patients despite treatment. Four children died, yielding a case-fatality rate of 0.8%. Several prognostic variables, assessed at baseline, were significantly associated with duration of pneumonia episode in univariate analyses. These were: young age (infants), refusal of diet, presence of lung complications, tachypnoea, signs of dyspnoea, leukocytosis over 15,000*106/L, low birth-weight, weight-for-age z-score under -2, height-for-age z-score under -2, weight-forheight z-score under -2, chest-indrawing, clinical score [(a score between 1 (less severe) and 5 (more severe)] based on the paediatrician's general impression of the disease severity, and hypoxaemia. In multivariate analysis, young age, chest-indrawing, lung complications, low birth-weight, and duration of fever prior to arrival in hospital were significant variables (Table 6). Duration of hospitalization was strongly associated with several clinical indicators and tended to be longer for episodes with bacterial aetiology compared to those of viral aetiology (hazards ratio for recovery=0.32; 95% confidence interval 0.09-1.83). However, the final regression model included only lung complications, tachypnoea, and weight-for-age z-score (Table 6). Discussion Information on clinical presentation and prognostic indicators of childhood pneumonia cases treated with standard antibiotics are relevant for the planning and evaluation of public-health control strategies and treatment of individual patients. This study reports the characteristics and outcome of community-acquired pneumonia cases in children of Northeast Brazil. General lack of information in this respect, particularly in the study area, justifies the importance of the study. One in every four children in the study reported another pneumonia episode in the preceding 12 months, which indicates an obvious high burden of pneumonia in this population. Although this information comes from retrospective data, not confirmed by medical records, and refers to high-risk children, i.e. those recruited to the study because of pneumonia, it is consistent with the previous incidence estimated from population-based studies of 0.26 episode per child per year (7). This constitutes a considerable burden to health services, especially taking into account that a high proportion of these children (55% during the study and 49% in the preceding year) needed to be hospitalized and remained so for a median period of six days. We used clinical diagnosis supported by radiology. We believe our cases represent well those with actual lung infection, which forms a particularly important sub-group of all the ALRI cases. Although the majority of the patients reported cough, fever, and 'cansaço' (respiratory distress), almost half of them did not have tachypnoea or chest-indrawing at ad-mission. The low sensitivity of these signs for diagnosis of pneumonia in these children raises the question of their validity for diagnosis of the disease in areas of wide-spread use of non-prescribed antibiotics. This may reflect treatment attempts before arrival to hospital, which, in some cases, may alter the clinical presentation. Self-medication and purchase of non-prescribed medicines, which may easily be obtained from and even recommended by pharmacy attendants, are highly prevalent in Recife, as reported from other areas of Brazil (15). The reported previous use of antibiotics in 25% of the study children is probably an underestimate, given the expected low correlation between maternal report and actual antibiotic use, confirmed by laboratory tests (16). The design and expected efficacy of pneumonia-control programmes relying on case management and immunization strategies depends on information on the pattern of aetiology, which may show a considerable geographic variation. We found only one study on bacterial aetiology of pneumonia in hospitalized children in this region of Brazil (17). This study showed a similar prevalence of S. pneumoniae and H. influenzae in lung aspirates and confirms that bacteria are the most frequently-identified pathogens in pneumonia in hospitalized children. This is consistent with the findings of other studies in hospital settings (18). At the same time, however, the positive bacterial culture, yielded in this study, was relatively low, which may be due to prior antibiotic use, or restriction to non-invasive methods for aetiologic diagnosis in this study. The unusual predominance of H. influenzae over S. pneumoniae in our study probably reflects higher sensitivity of the latex test for urine samples for the diagnosis of this agent compared to the latter (19,20) and may also have been influenced by age distribution of the study children. Also, as the latex agglutination of urine samples specifically tested for H. influenzae and S. pneumoniae, this may well have overestimated the contribution of both the pathogens, particularly H. influenzae, compared to other agents. On the other hand, des-pite reports of low test specificity in healthy populations with high carriage rates of S. pneumoniae (21), its specificity is likely to be high in the selected group of patients with confirmed lung infection, The high incidence of prior antibiotic use further contributed to the negativity of blood cultures, especially for agents, such as S. pneumoniae and the lack of isolation of a wider range of agents, which must also give some contribution to cases of community-acquired pneumonia. Nevertheless, the role of H. influenzae in childhood pneumonia cases should not be underestimated in an area where H. influenzae type b vaccines had not been introduced in a large scale. Investigation for viral aetiology was possible in 438 children, whose nasopharyngeal secretions produced adequate material for the diagnosis of at least one of the agents. Lack of enough epithelial cells and, in some cases, an excess of mucus were the main reasons for not doing the tests. Clinical diagnosis of pneumonia by experienced paediatricians, confirmed mostly by chest radiology, and time-delay for children to arrive at hospital after development of symptoms and exclusion of other ALRIs may account for the relatively low contribution of viruses in this series. Swabs were used instead of washes, due to local experience with this technique, but its lower sensitivity compared to washes may also help explain the low viral contribution to aetiologic diagnosis in this study. Viruses are more important in the aetiology of non-pneumonia ALRI. The distribution of viruses, with the predominance of RSV, followed by influenza, parainfluenza, and adenovirus, is consistent with results of other studies (18). Mycoplasma and Chlamydia, not important agents of pneumonia in this age group, were identified in only three children. Although the test for Chlamydia is genus-specific, we assume that C. pneumoniae was the most likely species involved in the two cases identified. The prognosis was favourable in the majority of the cases. The pneumonia case-fatality rate of only 0.8% was well below the average for developing countries, which has been estimated to be 10% for bacterial infections, 1.5% for viral infections, and 11.6% for mixed infections in children aged less than five years (18). It is important to note that these patients come mostly from urban areas where access to health services is relatively good, and the prevalence of HIV infection in this age group is very low. All patients were managed according to a standard protocol and were carefully followed up for a minimum of 11 days, providing additional evidence for the success of the case management strategy for the control of pneumonia in children. Other factors, which may have contributed to the low case-fatality rate, were the exclusion of infants aged less than six months and of some very severe cases, such as those with septicaemia. The study was not powered to look directly at risk factors for mortality due to pneumonia, and we used the duration of episode and of hospital admission as indicators of severity. Multivariate analysis allowed us to determine the best predictors of severe illness, based on the variables ascertained at baseline. These were lung complications, chest-indrawing (for duration of episode), and tachypnoea (for duration of hospital admission) at baseline. Young age, low birth-weight, and prolonged fever prior to admission to the study also predicted a more prolonged illness, and weight-for-age z-scores under -2 was a predictor of longer hospital admission. These findings are not surprising. An association between age and mortality due to pneumonia is well-recognized, as immunologic immaturity and anatomical features predispose the young child to more severe infections (22). The same applies to low birth-weight, which is associated with impaired immune response (23,24), lung function (25,26), and mortality due to ALRI (27). Children with a longer duration of symptoms prior to arrival at hospital tended to present with a more severe disease. The association between the case-fatality rate of pneumonia in children aged less than five years and the duration of fever and longer period of illness before contact with health services has been shown in Papua New Guinea (28) and Tanzania (29). The most important criterion for discharge from hospital is clinical improvement, with disappearance of signs of severity. Not surprisingly, a longer duration of admission was observed among malnourished children with weight-for-age z-scores under -2. The synergism between malnutrition and infection is widely acknowledged, and various studies in developing countries have shown that malnourished children have an increased case-fatality rate of pneumonia (30-32). Impaired local and systemic immunity in malnourished children is a likely explanation for the increased severity of pneumonia in these children (33-34). While appropriate case management and development and implementation of new vaccines are important measures for reducing childhood morbidity and mortality due to pneumonia in developing countries, particular attention should be placed on children likely to have a worst prognosis. These include those with more severe clinical findings on admission (notably with lung complications, rapid breathing, or chest-indrawing) and presenting with a history of fever of long duration, the younger, malnourished, and those with low birth-weight. Acknowledgements We are grateful for the grants provided by the Wellcome Trust, UK and CNPq, Brazil and for all staff members who made this study possible. In particular, we thank Dr. Ramilson A. Rodrigues, Dr. Regina W.S. Carneiro, Dr. Leonel Campos (Hospital Barão de Lucena, Recife, Brazil), and Mrs. Adriana F. Benjamin (Univer-sidade Federal de Pernambuco, Recife, Brazil) for participation in data collection and Ms Maria C.D.S. Fink (Universidade de São Paulo, São Paulo, Brazil), Mr. Steve Rice (Middlesex Hospital, London, UK) and Dr. Wyller (Instituto Evandro Chagas, Belem, Brazil) for laboratory support for aetiologic diagnosis. We dedicate this work to the late Paul Arthur, whose early departure has been greatly missed. References
© 2005 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn05002t4.jpg] [hn05002t1.jpg] [hn05002t3.jpg] [hn05002t6.jpg] [hn05002t5.jpg] [hn05002t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}