 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 23, No. 1, March, 2005, pp. 25-33 Introducing Hepatitis B Virus Vaccine into the Expanded Programme on Immunization in Bangladesh: A Proposed Method to Evaluate Whether the Existing Infrastructure Has the Capacity Annalisa Trama1; Damian Walker2; Julia Fox-Rushby2; 1Health Services/Systems Research,
2Health Policy Unit, and Health Policy Unit,
London School of Hygiene & Tropical Medicine,Keppel Street, London
WC1E 7HT, UK
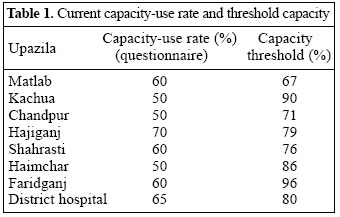
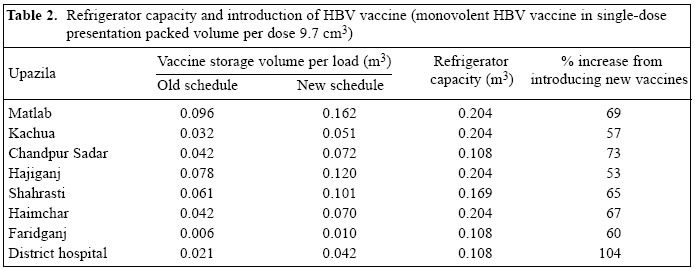
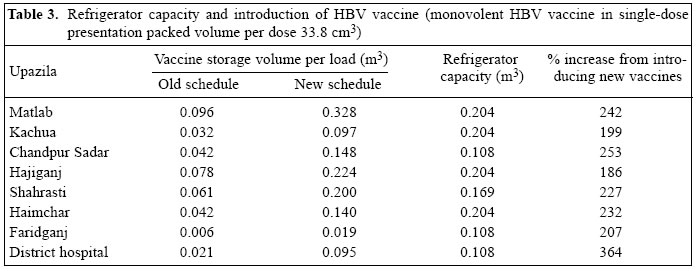
Code Number: hn05004 ABSTRACT To determine whether the existing Expanded Programme on Immunization (EPI) in Bangladesh has the capacity to introduce the hepatitis B virus (HBV) vaccine, this study was carried out in all the nine health facilities, which maintain a cold-chain, in Chandpur district of Bangladesh. The research, focusing specifically on cold-chain equipment, aimed at developing and applying an indicator of the use of cold-chain equipment. A structured questionnaire, developed and field-tested, was used for collecting information on cold-chain equipment and their use-rate. Data were used for estimating the resources needed to introduce the HBV vaccine and for increasing the coverage of measles and DPT vaccines. The findings of the study showed that the use-rate of cold-chain equipment in this district was low, suggesting that the district has sufficient spare capacity to introduce and sustain the storage of an increased quantity of vaccines. This paper suggests an approach to study capacity in relation to infrastructural facilities. By measuring the capacity of capital equipment, the study has illustrated that the measurement of resource-use rates provides useful information about the burden that a new vaccine places on the EPI. Key words: Refrigeration; Hepatitis B virus; Hepatitis B vaccine; Vaccines; Expanded Programme on Immunization; Bangladesh Introduction In developing countries, over 11 million children, aged less than five years, die each year, and nearly three-quarters of these deaths result from infectious diseases. The World Health Organization (WHO) estimates that the death of at least four million of these children is linked to their lack of access to vaccines (1). Vaccines are highly effective against childhood diseases preventing an estimated three million deaths a year (2). Although, since the mid-1970s, the global immunization coverage for the six preventable diseases - diphtheria, measles, pertussis, polio, tetanus, and tuberculosis - originally targeted by WHO, has improved significantly, the rates of coverage of children in the poorest countries are still low. The Expanded Programme on Immunization (EPI) in Bangladesh was launched nationwide in 1974 aimed at reducing morbidity, mortality, and disability associated with tuberculosis, tetanus, diphtheria, measles, pertussis, and poliomyelitis. The EPI experienced four phases of development. Phase one was started in 1979; phase two, learning and experimentation, lasted from 1985 to 1993; phase three, carried out during 1993-1995, expanded the coverage of the EPI at a rapid rate; and phase four is characterized by well-established infrastructure and knowledge of mothers about the need for childhood and maternal immunizations. The national EPI coverage remained stable during the 1990s. A survey in June 2001 reported a coverage of 93.7% for BCG, 65.4% DPT3, 65.5% OPV3, and 64.2% measles. A general concern is that, while the coverage rates have not declined, they appear to have reached a plateau. Despite the extensive infrastructure of the EPI, especially in the rural areas, and the heavy use of outreach activities, an estimated 53% of children are fully immunized by 12 months of age. This is because many children do not complete their vaccination series - drop-out rates have been rising since 1995 and are currently estimated at 25% from DPT1 to measles and 15% from DPT1 to DPT3 (3,4). However, as shown by the high BCG coverage rate, access to the EPI is quite good. The Government of Bangladesh is currently preparing a proposal to both improve the overall EPI and introduce the hepatitis B virus (HBV) vaccine into the EPI, aimed at increasing the EPI coverage from the current 68% for DPT3 to 90% by 2006 and to introduce the HBV vaccine in phases reaching nationwide coverage by 2004. Improving the coverage for the six basic vaccines - tuberculosis (Bacillus Calamette Guerin, BCG), diphtheria, pertussis, tetanus (DPT3), measles, and poliomyelitis (OPV3) - is fundamental because an estimated 20,000 deaths per year still occur each from neonatal tetanus and measles. A related priority is, thus, to improve the cold-chain system. The burden that a new vaccine places on the EPI in terms of cold-chain requirements and procurement was mentioned by several policy-makers as an important factor in deciding whether to consider the introduction of the vaccine. Some mentioned it as the second most important constraint, after cost, to the introduction of new vaccines (3). According to the priorities of the Government of Bangladesh, there is a need to assess whether the existing infrastructure has the capacity to sustain the expansion of the EPI. Based on the introduction of the HBV vaccine and the proposed increase in the coverage of measles and DPT vaccines in the existing EPI, the study describes a technique employed to quantify current EPI resources and assesses their capacity to determine whether they will be sufficient in sustaining the implementation of the EPI in these circumstances. Capacity is discussed in terms of use-rate of the required resources, such as personnel, equipment, infrastructure, etc., to accommodate the delivery of additional vaccines and supplies. The study focuses on cold-chain equipment, as an example, with the following specific objectives: (a) develop an instrument to assess the capacity-use rate of cold-chain equipment; (b) measure the capacity-use rate of cold-chain equipment in selected vaccine-storage centres; (c) evaluate the capacity of cold-chain equipment to accommodate the introduction of the HBV vaccine; (d) measure the capacity of cold-chain equipment to accommodate an increase in the coverage of measles and DPT vaccines; and (e) analyze the quality of cold-chain equipment. Materials and Methods Study site The study was carried out in Chandpur district of Bangladesh. Bangladesh is administratively divided into six divisions, 64 districts, 507upazilas (sub-districts), and 4,484 unions. Each union has, on average, three wards, and each ward comprises a number of villages. Chandpur district has seven upazilas: Haimchar, Faridganj, Kachua, Shahrasti, Matlab, Hajiganj, and Chandpur Sadar, 91 unions, and 273 wards. This district was selected after ranking all the 64 districts from best to worst according to three indices: the Khulna Poverty Index, the Human Development Index, and a third index specifically developed by a larger project, of which this study is a sub-component. The last index is based on four indicators: spread of relevant diseases/symptoms, access to healthcare, socioeconomic and geographic variables. The availability of data, particularly concerning the local policy plans, about the introduction of the HBV vaccine, the possibility of using an already-settled infrastructure (ICDDR,B: Centre for Health and Population Research), and time constrains were other parameters that helped in the final selection. EPI service-delivery along the health system In Bangladesh, the EPI is run under two different systems: one for rural areas and the other one for urban areas. The Ministry of Health and Family Welfare (MoHFW) is responsible for the EPI in the rural areas. The EPI vaccines are delivered on a quarterly basis from the EPI headquarters (EPI HQ) in Dhaka to the Civil Surgeon's Office, which is the biggest vaccine-storage centre in the district. The next largest vaccine-storage centres at the district level are the district hospitals and the Upazila Health Complexes (UHCs). The Civil Surgeon's Office supplies vaccines on a monthly basis to both, and the UHC then distributes the vaccines to non-governmental organizations (NGOs), outreach clinics, and fixed clinics in unions. Unlike many countries, the programme relies heavily on outreach activities, in addition to the fixed sites (3). In Chandpur district, there are one district hospital, seven UHCs, and three NGOs: Society for Project Implementation Research Evaluation & Training (SOPIRET), BRAC, and Urban Family Health Partnership (UFHP), all of which contribute to the mobilization process of the EPI and administration of the EPI vaccines and pro-vide personnel for the routine outreach activities. Moreover, in Matlab, an important satellite centre of ICDDR,B provides various health services to almost a quarter of this upazila's population and is involved in the administration of the EPI vaccines and disease surveillance. Design and development of tools Measurement of EPI cold-chain capacity According to WHO (5), vaccine-storage capacity is a measure of net space in a refrigerator, a freezer, a cold-box, or a vaccine carrier for the storage of vaccines. According to such measurement, the indicator of capacity-use rate of cold-chain equipment has been defined as the percentage of space used for the storage of vaccines after their delivery to the health centres. Since the vaccines are delivered every three months to the Civil Surgeon's Office and monthly to the district hospital and UHCs, the capacity-use rate is measured quarterly and monthly respectively. The capacity threshold has been defined as the highest capacity-use rate that would accommodate the introduction of the HBV vaccine without increasing the number of pieces of equipment for the storage of vaccines. It has been measured by subtracting from the capacity of the cold-chain equipment that proportion required for the storage of the HBV vaccine. The capacity of the cold-chain equipment reported in the WHO product information sheet has been used for defining the maxi-mum space available for the storage of vaccines. The volume of the HBV vaccine has been calculated for each upazila considering different parameters, e.g. number of doses per child, vaccine-wastage rates, vaccine pack volume per dose, and annual number of livebirths. Development of data-collection instrument: the questionnaire A structured questionnaire was developed and administered to the EPI technician by way of a face-to-face interview enabling the interviewer (a Bangla speaker) to clarify any ambiguous or complicated questions and to check information of greater depth. The questionnaire was designed in accordance with the one used by Edmunds et al. (6), also closely following the WHO guidelines (7), WHO product information sheets, and other WHO forms relating to the introduction of the HBV vaccine, provided by the WHO Medical Officer based at the EPI headquarters in Dhaka. Additional information, e.g. type and make of refrigerator, its maxi-mum capacity, the procedures for vaccine distribution, etc., was collected by interviewing the Senior Cold-Chain Engineer and the Manager of the EPI Central Store at the EPI headquarters in Dhaka. The questionnaire was translated and piloted before being used in the study area. The questionnaire has three sections. The first section provides an inventory of cold-chain equipment avail-able in the health centres, describes the rules for vaccine request and delivery, and explores the usual requirements of vaccine storage. A series of questions were included and asked on additional equipment needed for the introduction of the HBV vaccine. To help, the respondents were informed that the HBV vaccine requires three doses, like DPT, and an estimation of the vaccine pack volume per dose was given as well. The second section aims at collecting information about the quality of cold-chain equipment. The third section looks into two important records: the vaccine vials stock record and the EPI immunization report. Since this section provides recorded data about the number of vaccines delivered and used, it has been added with the specific purpose of checking the validity of the answers obtained from the EPI technician in the first section. Vaccine volume calculator of WHO To check for the results of the questionnaire, besides the comparison with the formal EPI record, a more objective method, suggested by WHO, was carried out to assess the capacity use of cold-chain equipment in relation to the introduction of the HBV vaccine. The Department of Vaccines and Biologicals of WHO, in collaboration with the Bill and Melinda Gates Children's Vaccine Program, has developed and published a vac-cine volume calculator to assist countries in planning for space requirements when introducing new vaccines. The vaccine volume calculator estimates the net storage requirements per fully-immunized child and woman of childbearing age with selected immunization schedules. It also provides an estimate of the percentage change in storage volume required for introducing a new vaccine (8). Information on the capacity of equipment is avail-able from the product information sheet. Comparison of the capacity of equipment with the new net storage volume required by the new immunization schedule has been possible to assess whether the current capacity could accommodate the new vaccine. Results obtained through the WHO calculator were then compared with those obtained by interviewing the EPI technicians. Different types of information that should be recorded on the pre-defined WHO calculator sheet (8) include: (a) Number of doses per child for each vaccine in the existing immunization schedule; (b) Number of doses per child for all vaccines in the new immunization schedule, i.e. existing vaccines plus new vaccines, such as HBV vaccine; (c) Wastage rates of existing vaccines and estimated or predicted wastage rate of new vaccines; (d) Vaccine pack volume per dose; and (e) Annual number of livebirths. Information on the number of doses per child for each vaccine in the existing and new immunization schedules was collected according to the EPI schedule in Bangladesh. Since the HBV vaccine will be administered in a three-dose schedule as is the case with the DPT vac-cine, the wastage calculation used for the DPT vaccine has been applied to it. The wastage of DPT vaccine was calculated using data collected from the vaccine vial stock record and EPI immunization report (section 3 of the questionnaire). Activities of a year were checked, and the following formula for vaccine wastage (f) was used (8): f=((v+c) x d)/n where, v=number of vials opened for use, c=number of closed vials discarded because of cold-chain failure or vaccine vial monitor (VVM) indication, d=number of doses per vial, and n=number of doses administered. The vaccine pack volume per dose differed according to the number of doses per vial and manufacturers. The WHO-recommended vaccine pack volume was used for all EPI vaccines in the current schedule; for HBV vaccine pack volume, estimates of Glaxo/SmithKline and LG, manufacturers in Korea were used. Information on the number of livebirths for each upazila was obtained from a demographic report available at the Civil Surgeon's Office. Results The questionnaire was administered in the Civil Surgeon's Office, one district hospital, and seven UHCs; there was no refusal to participate. Cold-chain equipment in Chandpur Cold-chain equipment was almost the same in each UHC, i.e. each upazila had a freezer, a refrigerator, and a variable number of cold-boxes and vaccine carriers. The Civil Surgeon's Office had the most equipment, although 10 of 22 refrigerators were out of order and seven were not currently in use, despite being in good condition. The latter were at the disposal of the Civil Surgeon's Office and any UHC in the case of necessity. Moreover, although four freezers were working, only two were available in the Civil Surgeon's Office. In the district hospital, no cold-boxes were available. Capacity-use rate of cold-chain equipment All the UHCs stored vaccines in refrigerators; freezers were used for storing ice-packs only. Because of this, capacity-use was assessed only for refrigerators; data showed that the capacity-use rate ranged from 50% to 70% (Table 1). In the Civil Surgeon's Office and in the district hospital, TT, BCG and DPT vaccines were stored in refrigerators, while measles and OPV vaccines were kept in freezers together with ice-packs. In the Civil Surgeon's Office, the refrigerator capacity-use rate was 80%; in addition, another seven refrigerators were avail-able for use if needed. Space in the freezers was fully used for storing ice-packs (50%) and vaccines (50%). In the district hospital, the refrigerator capacity-use rate was 65%. For freezers, pre-determined 80% of space was reserved for ice-packs, although only 60% of it was used; the remaining 20% of space was meant for the storage of vaccines; of this, only 12% was routinely used for storing vaccine vials. The Hajiganj upazila had the highest capacity-use rate (70%). These data suggest that abundant free space was available in cold-chain equipment in all the UHCs, district hospital, and Civil Surgeon's Office, after the delivery of vaccines, to accommodate additional vaccines. Capacity threshold The capacity threshold varied among the different UHCs. The lowest value was registered in Matlab (67.5%), while Faridganj reached the highest value (96%) (Table 1). However, no current capacity-use rate in UHC reached the threshold. Impact of cold-chain capacity-use rate on introduction of HBV vaccine: questionnaire results The answers of the EPI technician were used as the basis to confirm whether the spare space available would be enough to store the HBV vaccine when introduced in the EPI and/or to store an increased quantity of DPT and measles vaccines. Similar questions were asked about cold-boxes and vaccine carriers. According to the answers provided by the EPI technicians, six UHCs had enough spare space in refrigerators to accommodate the introduction of the HBV vaccine, with Hajiganj being the only exception. One additional refrigerator would be needed for the Hajiganj UHC. These answers support the previous estimate which revealed the capacity-use rate being far below 100% and the Hajiganj UHC being the one with the highest capacity-use rate (Table 1). In all the UHCs, except the one at Hajiganj, the number of cold-boxes, necessary to support the delivery of the HBV vaccine, was considered sufficient; in the Hajiganj UHC, three more cold-boxes would be required. Eight more vaccine carriers would be needed for the Haimchar UHC and 30 more for the Hajiganj UHC. The district hospital and the Civil Surgeon's Office stored DPT vaccines in refrigerators and measles vaccine in freezers, and it was, therefore, necessary to provide results for both the types of equipment. In the district hospital, the spare space in refrigerators was not enough to store the HBVvaccine but there was no apparent space problem either for freezers or for vaccine carriers (cold-boxes were not available in the district hospital). In the Civil Surgeon's Office, since seven refrigerators were available in the case of necessity, there were no problems in storing an increased quantity of vaccines, including the introduction of the HBV vaccine; how-ever, as already pointed out, there was no spare capacity in the freezers. The answers did not change when questioned about increasing the quantity of DPT and measles vaccines. Regarding the storage of DPT and measles vaccines, the EPI technicians estimated that the refrigerators had enough space to store an increasing quantity of DPT and measles vaccine vials. Also the number of cold-boxes and vaccine carriers was considered adequate in six of the seven UHCs. Only the Hajiganj UHC needed more cold-chain equipment, specifically one more refrigerator, four more cold-boxes, and 30 more vaccine carriers, to accommodate the increasing quantity of DPT and measles vaccine vials. The respondents gave consistent answers regarding their capacity to accommodate the HBV vaccine and DPT or measles vaccine. Apart from the Hajiganj UHC, all of the other six had enough capacity to accommodate either the HBV vaccine or the increased quantity of measles and DPT vaccines. In Hajiganj, there were also problems regarding the number of cold-boxes and vac-cine carriers. In the district hospital, there was no spare capacity in the refrigerator, whereas in the Civil Surgeon's Office, problems existed mainly with freezers. Impact of cold-chain capacity-use rate on introduction of HBV vaccine: results of the WHO vaccine volume calculator Tables 2 and 3 show the capacity of refrigerators according to the WHO product information sheets and the vaccine-storage volume of the old and new EPI schedules, including the HBV vaccine, calculated according to the WHO vaccine volume calculator. Calculations were performed according to two different estimations of the HBV vaccine pack volume per dose. Since the volume of multi-dose vials of DTP-HBV vaccines will be the same as that for multi-dose vials of DPT vaccines that are currently used (3 cm3), the different and higher volumes of monovalent HBV vaccine in single-dose presentation were considered: 9.7 cm3 and 33.8 cm3. No calculations were done for the Civil Surgeon's Office since the capacity of refrigerators was deemed to be enough with the presence of seven extra refrigerators not currently in use. It was evident from the comparison of the vaccine-storage volume of the new schedule with the refrigerator capacity that, estimating a pack volume per dose of 9.7 cm3, the refrigerator capacity was higher than the storage volume required (Table 2) and, therefore, the new vaccine could be accommodated in the existing refrigerators at the UHCs. However, with the increase in the pack volume per dose up to 33.8 cm3, the capacity of the refrigerator is less than the storage volume needed (Table 3) and, therefore, the refrigerators that are already used in the UHCs cannot be used for the introduction of the HBV vaccine. These results were constant for all the UHCs and for the district hospital. Capacity of refrigerator and introduction of HBV vaccine: questionnaire vs vaccine volume calculator of WHO The responses to the questions and the results of the WHO vaccine volume calculator for the introduction of the HBV vaccine, when compared, were consistent with regard to the availability of spare space to accommodate the HBV vaccine; the results differed only for the Hajiganj UHC and district hospital. Accordingly to the WHO calculator, both Hajiganj UHC and the district hospital had enough capacity to store the HBV vaccine; on the contrary, the EPI technicians estimated that the capacity was not enough to store the vaccine. Quality of cold-chain equipment The study was able to assess a few points concerned with the quality of cold-chain equipment available at the UHCs. The results showed that the refrigerators and free-zers currently in use were all working. Although some of them have been used for more than 10 years, they had not broken down in the last year, and most of them were dry and clean. The EPI technicians were well-in-formed of the rules relating to their maintenance and had good knowledge about the temperature needed to be maintained for the storage of vaccines and the correct positioning of EPI vaccines in the refrigerator. All refrigerators and freezers in the UHCs, district hospital, and Civil Surgeon's Office had a thermometer inside, and the temperature was maintained in the correct range when checked. The major problems concerned with the temperature record sheet were that quite often they were either not available or incomplete. Concerning vaccine carriers, the main maintenance problem was the lack of rope change that facilitates their carriage. DiscussionThe findings of the study provide an accurate description of the cold-chain equipment available in different health facilities in Chandpur district. Different models of refrigerators and freezers - the main equipment - were used in the UHCs, but there was no difference in their quantity. The number of cold-boxes and vaccine carriers varied among the UHCs, with higher quantities in more crowded upazilas or in upazilas where the population is concentrated in rural areas. Since the EPI delivery system is the same in all the districts and the EP headquarters in Dhaka is the main provider of cold-chain equipment nationwide, it is reasonable to assume that all the districts in Bangladesh have the same kind of equipment as identified in Chandpur district and is very similar in distribution of equipment across the UHCs. According to the findings of the study, all the UHCs, district hospital, and Civil Surgeon's Office had a very similar low use-rate of cold-chain equipment. This result is more difficult to generalize nationwide because, although the study was carried out in the entire district, it looked into only one of 64 districts, and the number of health centres visited was low (n=9). Moreover, according to all the different indices used for selecting the district, Chandpur was ranked in the 'best' third which suggests that Chandpur is not entirely representative. These results may not reflect the situation in a context different from Bangladesh. In many other countries, the current capacity varies considerably with the administrative level, where spare capacity in refrigerators is relatively great but is often smaller at the district and provincial levels (7). In this study, the spare capacity was relatively great but it did not change significantly according to the administrative level, and it is at the higher administrative level (Civil Surgeon's Office and district hospital) that more problems about capacity arose. The study reports enough capacity in the cold-chain equipment of the district to accommodate the introduction of the HBV vaccine or the increasing coverage of DPT and measles vaccines. However, looking at the example of HBV vaccine, the type of vaccine selected may have a considerable impact on the cold-chain storage capacity. The storage requirements for multi-dose vials of DTP-HBV vaccines are the same as those for multi-dose vials of DPT vaccines that are currently used (3 cm3). Yet, if the monovalent HBV vaccine in single-dose presentation is used, the storage requirement will increase (9). The study assessed the effect of this storage volume capacity for different types of vaccines: if a package volume of maximum 9.7 cm3 is selected, the capacity of existing equipment will be enough to accommodate the introduction of the HBV monovalent vaccine. If a bigger package is used (up to 33.8 cm3), the capacity will not be enough, and additional equipment leading to additional cost will be required. This important information could be useful also in guiding which formulation and package would be better for procurement. Available evidence suggests that technical inefficiencies arising from under-use of equipment due to lack of spare parts reduce the cost-effectiveness of EPI strategies (10,11). The capacity-use rate is a determinant of quantity of inputs needed for an intervention, and it, therefore, mainly influences the costs of an intervention. According to what has been discussed so far, measurement of equipment capacity-use appears to be fundamental to assess efficiency, to evaluate implications of programme expansions, and to provide correct information for a costing exercise in cost-effectiveness analysis. As has been already pointed out, the study was undertaken in one district only and nine health centres, which limits the generalizability of the results. How-ever, the choice of the study area was mainly influenced by the budget and time constraints, and this analysis should be viewed more as a starting point for further work. The main weakness of the study is the fact that a restricted perspective was adopted. Measuring the capacity-use rate of cold-chain equipment does not portray the full-blown picture of the EPI capacity. To analyze it, all the main resources should be assessed, and conclusions should be based on this wider approach. If the introduction of a new vaccine has to be considered, it is possible to state that, since cold-chain equipment is not used to full capacity, it is not necessary to purchase more equipment to store new vaccines. However, this on its own is not sufficient, and further information should be collected also about the capacity of vehicles to transport it and about the spare time of existing personnel to administer the new vaccine and other related issues. Considering that capacity should be assessed to define the technical efficiency of a service, only by measuring the capacity of all the different inputs involved will it be possible to provide appropriate information about their most efficient use. Although the study results do not appear very significant in the wider context of the EPI, its main strength lies in the development of different tools that can be widely used as examples. The structured interview questionnaire can yield highly accurate data (12) with regard to the measurement of the capacity of cold-chain equipment. This was clearly demonstrated also from the comparison with the WHO calculator which showed consistent results regardless of the methods used for obtaining them (the WHO form or the questionnaire). The questionnaire is simple and fast to administer and can be easily integrated with other instruments used for the collection of primary data. Moreover, because EPI resources are similar all over the world, the elaborated and tested instrument for cold-chain equipment can be easily tested and adapted to other contexts. The questionnaire used in the study was rather lengthy because many questions were incorporated to confirm or gather information that was impossible to attain prior to the study. Based on these considerations and also on the experience gained in carrying out the study, it is possible to develop a definitive and shorter version of the questionnaire. The indicator used for assessing the capacity-use rate of cold-chain equipment is objective, it is easy to estimate the rate with extensive experience in the field and to measure given standard information about vaccines and equipment. This model can be effectively applied to other equipment and any other resources that have specific spatial limits, e.g. rooms, buildings, vehicles, etc. The study has evaluated the quality of cold-chain equipment since this is an important pre-requisite for its use. If the equipment is in bad shape or too old, new equipment has to be sought, and therefore, the main concern would not be related to the space available. More-over, if the equipment is not properly working, it can reduce vaccine potency and increase wastage leading to more serious problems. The study assessed the quality of equipment through physical check-ups and indirectly by asking questions about maintenance and performance during the last year. The vaccine potency according to the Vaccine Vial Monitor Card has not been verified, although it is recognized and used as the main cold-chain quality indicator (13-15). The study suggested a general approach to assess the capacity based on the identification of all different resources involved in a programme and on the definition of a specific and measurable capacity indicator for each of them. By doing so, it is plausible and more appropriate to account for the differences that exist among resources. Applying this approach to the EPI in Bangladesh, the study sets the first steps to identify and develop specific instruments for measuring the capacity of cold-chain equipment. The study described the main cold-chain equipment (refrigerator, freezers, cold boxes, and vaccine carriers) available in the selected health facilities of a district, evaluated their efficient use, and measured their use-rate. The results of the study suggest that the existing cold-chain equipment could ccommodate the introduction of the HBV vaccine in the district and an increased quantity of DPT and measles vaccines. With an abundance of capacity of cold-chain equipment, the EPI can be expanded at a low cost. Higher capacity-use rates, over the capacity threshold-use rate estimated, would have lead to a radically different situation: expansion of cold-chain equipment, increase in capital costs (in the form of additional refrigerators, freezers, and cold-boxes), increase in recurrent costs (in terms of electricity, gas, ice-packs, kerosene, spare parts, and workshop costs), and a consequent expansion of the EPI at higher costs. This study measured the capacity of cold-chain equipment and its implication for programme delivery and expansion. Putting forward an example of capacity-measurement feasibility, it encourages people to evaluate the capacity of their cold-chain equipment. The questionnaire, in the simplified form obtained after its validation, represents an easy and user-friendly tool that can be always used locally. It proposed few questions suitable for making people think about the existing capacity of equipment used daily. The questions tested could be incorporated in general and in routine assessment of cold-chain equipment helping both EPI technicians in their routine activities and researchers or managers in further thinking about implication of the role of capacity when deciding about new policy/strategies relating to vaccine introduction or expansions. In conclusion, the vaccine-storage capacity appears to be a very critical issue for allocation and efficient use of resources and for cost estimation and its implications on the implementation of a programme. Considering the scarce availability of literature on this topic and the lack of capacity measurement in present economic analysis, further research is needed to develop appropriate indicators and to make their application a general and common rule for economic evaluation. Acknowledgements This research project has benefited from the contributions of many people. Dr. Md. Shahadat Hossain and Dr. Kuntal Kumar Saha of ICDDR,B: Centre for Health and Population Research helped in the organization of the fieldwork. Dr. Pierre Claquin of the Immunization and Other Child Health Project provided support in Bangladesh and kindly shared his knowledge and work. Mr. Mohammad Kamrul Islam, Senior Cold Chain Engineer of the EPI and Mr. Helal Uddin Tarafder, Manager of EPI Central Store provided fundamental information for the development of different tools of the study. Mr. Manu Md alamgir made tremendous effort to collect data and all the EPI technicians interviewed gave vital answers for the study. References
The following images related to this document are available:Photo images[hn05004t3.jpg] [hn05004t1.jpg] [hn05004t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}