 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 23, No. 1, March, 2005, pp. 52-57 Low Osmolar Oral Rehydration Salts Solution in the Treatment of Acute Watery Diarrhoea in Neonates and Young Infants: A Randomized, Controlled Clinical Trial A.M. Khan1, S.A. Sarker1, N.H. Alam1, M.S. Hossain1, G.J. Fuchs2, A.M. Khan1, S.A. Sarker1, N.H. Alam1, M.S. Hossain1, G.J. Fuchs2,
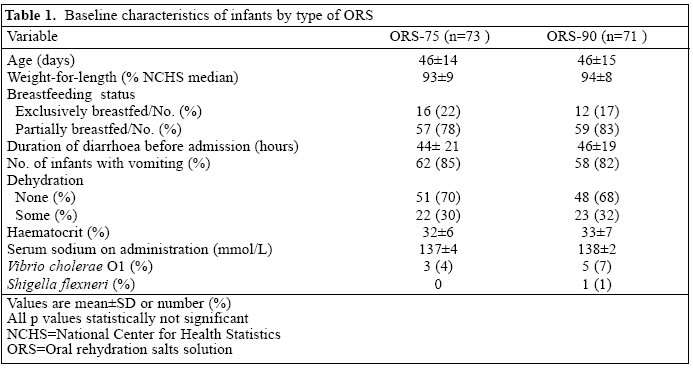
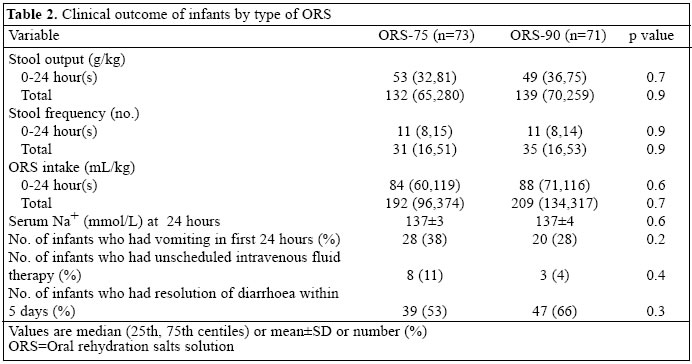
and M.A. Salam1 Code Number: hn05007 ABSTRACT To compare the efficacy and safety of low osmolar oral rehydration salts solution (ORS-75) (mmol/L: Na+ 75, osmolarity 245) with that of World Health Organization-recommended ORS (ORS-90) (mmol/L: Na+ 90, osmolarity 311 ) in the treatment of acute watery diarrhoea in neonates and very young infants, a randomized double-blind, controlled clinical trial was carried out at the Clinical Research and Service Centre of ICDDR,B: Centre for Health and Population Research, Dhaka, Bangladesh, during January 1998-December 1999. Infants, aged <2 months, presenting with a history of watery diarrhoea of <72 hours, with no or some dehydration and without any systemic illness, were randomly assigned to receive either ORS-75 or ORS-90 for the correction and subsequent prevention of dehydration. Infants were studied for a maximum of five days. Total stool output, stool frequency, and requirement for ORS were outcome measures. Serum electrolytes were measured at 24 hours after admission to monitor serum sodium imbalance. Seventy-three infants received ORS-75, and 71 received ORS-90. Both the groups were comparable in their baseline characteristics. Diarrhoea resolved within five days in 53% and 66% of infants receiving ORS-75 and ORS-90 respectively (p=0.3). Total stool volume [median (inter-quartile range) 132 (65-280) vs 139 (70-259) g/kg, p=0.9], during the study period, was not significantly different between the two groups. Total stool frequency [31 (16-51) vs 35 (16-53), p=0.9] and total ORS intake [192 (96-374) vs 209 (134-317) mL/kg, p=0.7] were similar between the groups. No infants developed late evidence of hypernatraemia, irrespective of treatment. The results of the study indicate that ORS-75 is as safe as standard ORS-90 in the treatment of acute watery diarrhoea in neo-nates and very young infants and is effective in correcting and preventing dehydration. Key words: Diarrhoea, Acute; Diarrhoea, Watery; Oral rehydration solution; Oral rehydration therapy; Osmolarity; Randomized controlled trials; Double-blind method; Clinical trials; Bangladesh Introduction Oral rehydration salts solution (ORS) recommended by the World Health Organization (WHO), popularly known as WHO-ORS recently labelled as ORS-90 (mmol/L: Na+ 90, osmolarity 311), has saved the lives of millions of children with diarrhoea, worldwide (1-2). But the optimal sodium concentration and osmolarity of ORS for neonates and very young infants need to be elucidated. Results of a few studies conducted are contradictory. Pizzaro et al. reported that neonates, aged up to 28 days, can be treated successfully with ORS-90 (3). Bhargava et al., in India, found a high incidence of hypernatraemia among young infants treated with this solution (4-5). In Turkey, Martin et al. compared the effect of ORS in the treatment of neonates and young infants aged 1-2 month(s) with that of older infants and concluded that neonates and young infants with infectious diarrhoea run a greater risk of developing abnormal fluid and salt retention during oral rehydration therapy because of immature renal function that is unable to excrete salt and water efficiently (6-7). To select an ideal composition of ORS formulation for clinical use, a few perfusion studies have been conducted in animal and humans (8-10). One of the major conclusions from these studies was that osmolarity and sodium glucose ratio have a dominant role in determining water absorption (8-10). Substantially higher water and optimum sodium absorption has been observed from a solution containing sodium 60 mmol/L and osmolarity 220-260 mmol/L compared to that with 90 mmol/L sodium and 311 mmol/L osmolarity (8-10). Based on these observations, further clinical trials with low osmolar ORS were conducted in different settings (11-13). The encouraging results of these studies were reviewed in a Joint Consultative Meeting of WHO and ICDDR,B in December 1994 (14), and the meeting recommended ORS with (in mmol/L) glucose 75, sodium 75, potassium 20, chloride 65, citrate 10, and osmolarity 245 for further clinical trial. We, therefore, conducted a randomized double-blind, controlled clinical trial with ORS of this new formulation to evaluate its efficacy and safety in neonates and very young infants with acute watery diarrhoea. Materials and Methods The study was carried out at the Clinical Research and Service Centre of ICDDR,B: Centre for Health and Population Research during January 1998-December 1999. The Research Review Committee and the Ethical Review Committee of ICDDR,B approved the protocol for the study. Patients Male neonates and young infants, aged up to two months, with a history of watery diarrhoea of <72 hours and with no or some dehydration, were enrolled in the study. Infants with a history of passage of bloodymucoid stool, or severe dehydration, or with any medical complications, including clinically-suspected sepsis, pneumonia, etc., were excluded from the study. Infants who had received an antibiotic for current illness were also excluded. Female babies were excluded from the study because of difficulties in separating urine from stool. Before enrollment, a written informed consent was taken from the parents or legal guardian of each participating infant after explaining the nature of the study. Randomization procedure Randomization of eligible children into treatment groups was performed using the random number table of permuted blocks of variable lengths and serially arranged to correspond to admission sequence of patients. The numbers in sequential order were kept in sealed envelopes. A trained and responsible person, who was not involved in the study, prepared the randomization list and sealed envelopes. The sealed envelope was opened only when the patient was ready for enrollment. According to the randomization number inside the envelope, the pharmacist on duty, who was not aware of the nature of the study, prepared ORS from contents packaged in identical polyethylene packets in a clean bottle marked with the patient's name and study number with-out identification of the solution. The contents of each packet of ORS were dissolved in one litre of clean water. The two prepared ORSs were identical in appearance. It was then supplied from the pharmacy to the staff who were involved in the administration of ORS for the study subjects. The codes in the form of A and B identifying the type of ORS were opened after data analysis and before writing the final report. Determination of sample size In a previous clinical trial conducted in our setting, children had a 10% reduction of stool volume with low osmolar ORS (mmol/L: Na+ 67, osmolarity 249) when compared with ORS-90 (12). Based on this study, the sample size was calculated to be 62 in each group to detect a 20% difference at the 5% significance level with 90% power. Considering approximately 15% drop-outs, we aimed to recruit 72 subjects in each group. Case management After fulfillment of the study criteria, infants were admitted and enrolled in the study. A physician took demographic and medical history and also performed physical examinations, including assessment of dehydration according to the WHO criteria (15). Findings were recorded on appropriate forms. After enrollment in the study, infants were randomly assigned to one of the two ORSs: ORS-75 (mmol/L: Na+ 75, K+ 20, Cl- 65, citrate 10, glucose 75, and osmolarity 245) or ORS-90 (mmol/L: Na+ 90, K+ 20, Cl- 80, citrate 10, glucose 111, and osmolarity 311). Infants were placed on diapers, and mothers were provided with a plastic container with cups and spoons. Infants with some dehydration were hydrated with ORS (75 mL/kg) over a six-hour period under the supervision of the nursing staff. After the correction of dehydration as assessed by a physician, ongoing loss of stool was replaced by the as-signed ORS on a volume-for-volume basis. Loss of stool in infants with no dehydration was similarly replaced by the assigned ORS. In both the groups, breastmilk was given freely from the beginning of the study and continued thereafter. Infants, partially breastfed and used to receiving infant formula, were given it as a supplement in addition to breastfeeding after the initial hydration until they could switch over to exclusive breast-feeding. During the study period, infants who developed some dehydration due to frequent vomiting and purging where hydration with ORS was not possible were rehydrated with intravenous polyelectrolyte solution (mmol/L: Na+ 67, K+ 7.5, Cl- 48, acetate 24, with 5% dextrose) and then again switched over to the as-signed ORS for subsequent replacement of ongoing loss of stool. A nurse monitored vital signs, such as pulse, respiration, and temperature, 8 hourly. The study physicians supervised the patients round the clock. Laboratory investigations On admission, white blood cell count, haematocrit, and serum electrolytes were determined. Serum electrolyte determination was repeated after 24 hours. Stool cultures for Vibrio cholerae, Shigella, and Salmonella spp. were done on admission. Outcome measurements Stool was collected in a pre-weighed diaper and weighed. Urine was collected separately using a paediatric urine-collection bag to prevent contamination with stool. The amount of ORS offered each time was recorded, and the leftover was measured to calculate the actual amount consumed by the study subjects. Intake of supplemented infant formula was also measured. Nude body weight was measured on admission, at randomization to treatment, and every day thereafter until the end of the study. For all measurements, an electronic scale (Sartorius, Germany) with a precision of 1 g was used. Scales were calibrated daily with standard weights. Mothers were provided with small pieces of round metal chips to place in a box for each episode of stool and vomiting to count frequency separately. All infants were followed for a maximum of five days. Cessation of diarrhoea was defined as the last watery stool or loose stool before passage of two consecutive soft or formed stools, or after 12 hours without passing any stool. Duration of diarrhoea was the time in hours from randomization until cessation of diarrhoea. Serum sodium concentrations of more than 150 mmol/L and less than 130 mmol/L were judged as hypernatraemia and hyponatraemia respectively. Stool output was defined as weight of stool in g per kg of body weight and was expressed per 24 hours or for the entire period of the study after randomization. Withdrawal from the study Those patients who continued diarrhoea beyond five days were considered as treatment failure and were withdrawn from the study. Those who developed complications, e.g. fever or respiratory infection, during the study were also withdrawn. Subjects leaving the hospital against medical advice were also considered to be withdrawn from the study. Data from all such patients up to the point of withdrawal were taken for analyses. Data analyses Statistical analyses were performed using SPSS for Window software (SPSS Inc., Chicago, IL, version 6.1). Ad-mission characteristics, such as age, body weight, duration of diarrhoea before admission, etc., were analyzed to make a baseline comparison between the two groups using Student's t-test for continuous variables with uniform distribution. Non-parametric Mann-Whitney-U test was applied to continuous variables with skewed distribution to compare outcome data, and the chi-square test was employed for discrete variables wherever it was necessary. Initial analysis of data was blinded; the treatment groups were labelled as 1 and 2 without the knowledge of which ORS each group had received. ResultsIn total, 144 neonates and young infants were enrolled in the study. Seventy-three infants received ORS-75, and 71 received standard ORS-90. In the ORS-75 group, 20 patients and, in the ORS-90 group, 17 infants continued to have diarrhoea beyond five days (p=0.6). They were withdrawn from the study and were given the usual standard treatment in another ward. Seven infants in the ORS-75 group and five in the ORS-90 group were also withdrawn from the study when they developed fever and respiratory tract infections during the study period. They were given standard treatment in a special care unit. All of them eventually recovered from their illness. Seven infants in the ORS-75 group and two in the ORS -90 group left the hospital against medical advice. Eighty-six infants completed the study and had resolution of diarrhoea within five days. Of these, 39 received ORS-75 and 47 received ORS-90. Data from all infants enrolled in the study were analyzed on the basis of intention-to-treat. Baseline demographic, clinical and laboratory characteristics were comparable between the two groups (Table 1). Clinical outcomes of the two groups showed that stool output, stool frequency, and intake of ORS during the first 24 hours and for the entire study period were similar (Table 2). None developed hypernatraemia, irrespective of group. Three infants receiving ORS-75 and two receiving ORS-90 developed very mild hyponatraemia (p= NS), and the lowest level of serum sodium in those cases was 127 mmol/L in each group. Other components of serum electrolytes and acid base status in both the groups were similar at 24 hours (data not presented). More infants on ORS-75 vomited during the first 24 hours than those treated with standard ORS-90, butthe difference was not significant. Proportions of infants who required unscheduled therapy with intravenous fluid were comparable (Table 2). Body weights at the end of study (mean±SD) (3.7±0.6 vs 3.8±0.6 kg, p=0.9), total frequency of breast-milk intake (median 58 vs 53, p=0.7), and total urine output (median 102 vs 115 mL/kg, p=0.4) were similar in both the groups. The total intake of supplemented infant formula (median 55 vs 51 mL/kg, p=0.6) was also comparable in both the groups. Discussion To our knowledge, no clinical trial has been conducted with low osmolar ORS of this formulation in neonates and very young infants with acute watery diarrhoea. It is an important clinical issue in treating diarrhoea in very young infants in developing countries. The results of the study demonstrated no statistically significant difference in stool output, stool frequency, and ORS in-take between the two groups. No infants developed hypernatraemia in either group, though mild asymptomatic hyponatraemia developed in some infants in both the groups. Thus, this study does not show any superiority of either solution but it does demonstrate the efficacy and safety of both when used in neonates and very young infants with acute watery diarrhoea presenting with some or no dehydration. The findings of our study are consistent with those of two other multicentre studies which demonstrated almost equivalent efficacy of standard ORS-90 and low osmolar ORS with this formulation in adults and children suffering from cholera and non-cholera diarrhoea respectively (16,17). Simultaneously, we admit a limitation of our study in that it does not indicate how the two ORS formulations would work in very young infants with more severe illness. The findings of this study differ from those of other studies in children with non-cholera diarrhoea where low osmolar ORS with sodium 60 mmol/L and osmolarity 250 mmol/L showed some benefit (11-13). Low osmolar ORS, in our study, contained a relatively higher concentration of sodium (75 mmol/L) compared to those used in other trials that demonstrated beneficial effects. The differences in the findings in our study may also be attributed to the very young age of the study subjects. For a long time, WHO has encouraged the use of a single ORS for all ages and for all types of diarrhoea, irrespective of aetiology. This simplified approach is highly encouraging. The consensus of the last meeting of the ORS Expert Committee in New York, USA, in July 2001 advocated the use of ORS with sodium of 75 mmol/L, glucose of 75 mmol/L, and osmolarity of 245 mmol/L instead of standard ORS-90 in developing countries (18). The results of our study provide support for this advocacy specially for very young infants. AcknowledgementsThis study was conducted at the ICDDR,B: Centre for Health and Population Research with the financial support of USAID, Washington, DC, vide the Cooperative Agreement no. HRN-A-00-96-90005-00. ICDDR,B acknowledges with gratitude the commitment of USAID to the Centre's research effort. We would like to thank the concerned nursing staff and physicians of CRSC for their valuable cooperation in the management of patients and Mr. M.A. Rahman Patwary for secretarial assistance. References
© 2005 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn05007t2.jpg] [hn05007t1.jpg] |
| |||||||||

{kind=link}
{kind=link}