 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 23, No. 1, March, 2005, pp. 74-81 Perceptions of Tuberculosis: Attributions of Cause, Suggested Means of Risk Reduction, and Preferred Treatment in the Limpopo Province, South Africa Supa Promtussananon1; Karl Peltzer2; 1Department of Public Health and
2Human Sciences Research Council and Department of Psychology, School of
Health Sciences, University of Venda for Science and Technology, Private
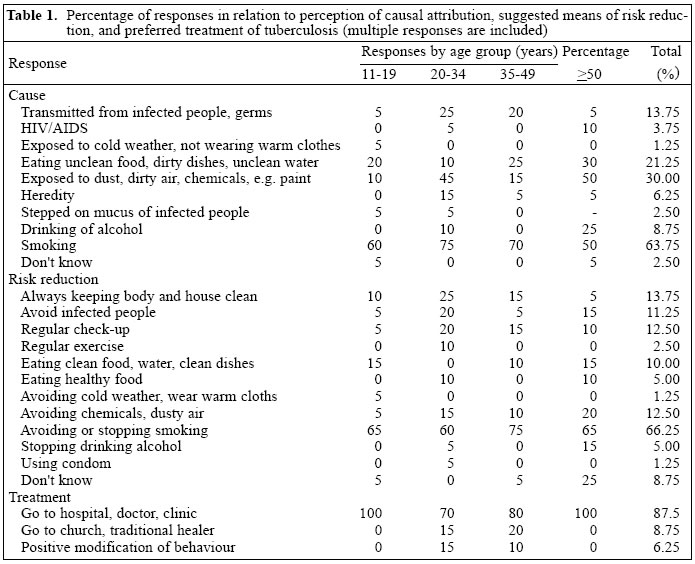
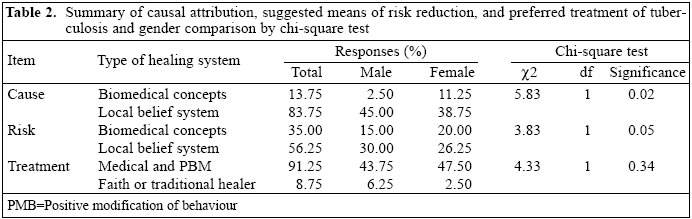
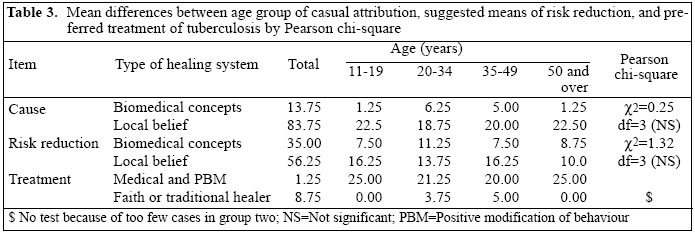
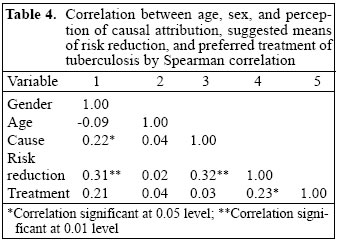
Bag X5050, Thohoyandou 0950, South Africa Code Number: hn05009 ABSTRACT Despite the availability of effective treatment regimens, exceptionally high rates of tuberculosis persist in South Africa. A better understanding of public perceptions of tuberculosis is important for the improvement of the existing tuberculosis-control programmes. This study was aimed at investigating public perceptions about causes, suggested means of risk reduction, and preferred treatment of tuberculosis. The cross-sectional study included a sample of 80 community members from four different age groups chosen by quota sampling in a semi-urban community. Results indicated that 13.75% of the community members reported biomedical causes of tuberculosis, 35% suggested biomedical methods as a means for risk reduction, and 91.25% preferred medical treatment. Significant gender but not age difference was found. Women reported more often than men a biomedical cause of tuberculosis. A number of misconceptions about the cause and risk reduction of tuberculosis were also mentioned. The results suggest that people in a semi-urban area of the Limpopo province have limited knowledge and understanding of tuberculosis. It is suggested that healthcare workers provide services for increasing basic knowledge about causes and risk reduction of tuberculosis of the population in every age group. Key words: Tuberculosis; Perceptions; Risk factors; Cross-sectional studies; South Africa Introduction South Africa is burdened by one of the worst tuberculosis epidemics in the world, with disease rates more than double those observed in other developing countries and up to 60 times higher than those currently observed in the USA or Western Europe. The Medical Research Council (MRC) estimated that the country had about 180,507 cases (55% reported) in 1997, or 419 per 100,000 of the total population. Of these, 32.8% (73,679 cases) were probably infected with HIV (1). The tuberculosis problem in South Africa is largely a result of historical neglect and poor management systems, compounded by the legacy of fragmented health services. Prior to the introduction of the Tuberculosis Register in 1995, cure rates were unknown, and consequently control efforts could not challenge the poor performance. The implication of this failure is evident from the fact that, in 1997, a cure rate of only 54% could be recorded, with the consequence of continued high rates of transmission in the country (1). Data on self-reported tuberculosis among men and women related more frequently to older people (e.g. age less than 35 years was 1.5% and age more than 35 was 4.6%) and people living in non-urban areas (e.g. men: urban 2.6%, non-urban 3.3%, women: urban 1.6%, non-urban 2.6%) (2). The Department of Health in November 1996 declared tuberculosis a top health priority, and National Health Minister Zuma committed her Department to implementing a new control programme based on the directly-observed therapy (DOT) strategy of the World Health Organization that includes: (a) Government commitment to a national tuberculosis programme as a specific health-system activity, integrated into comprehensive primary care, and supported technically at a national level; (b) Standardized, directly observed, short-course treatment, prioritizing sputum smear-positive patients; (c) Case detection by means of a patient-friendly and clinically-efficient service based primarily on smear microscopy (passive case-finding); (d) An ensured supply of essential anti-tuberculosis drugs; and (e) Effective monitoring (3). The pace and extent of implementation of the programme is, however, slow in most provinces. Since 1996, a system of case registration based on strict criteria for case definition was implemented in South Africa. These registrations, based on standardized criteria, are now beginning to present a clearer picture of disease rates in the country than what was available before (4). Some progress has been made in DOTS population coverage in South Africa (70% in 2001), but the implementation of the DOT strategy in the Limpopo province has been slow (1). Early case identification and adherence to treatment regimens are the remaining barriers to successful control of tuberculosis. Two twin problems of delay in seeking treatment and abandonment of prescribed regimens derive from complex factors. One reason for the patient's delay in seeking treatment may be poor understanding of tuberculosis among people as a disease and its risk factors (5). Westaway reported from a study in South Africa that tuberculosis was perceived as a threat, and sufferers of the disease were thought to be dirty and to eat bad food (6). In South Africa, the conventional strategies to combat tuberculosis focused on the treatment of individual patients within the framework of the control programme (7). This approach emphasizes the role of education and behaviour adjustment on the part of patients, particularly with regard to compliance with medical regimens (8). Causation and treatment of the disease, including problematic area, must be understood by taking into account the social environment of patients, including living arrangements, belief systems, and nature of community health services (9). Insights into social and cultural factors could possibly help reduce delays in diagnosis, improve treatment compliance, and provide suggestions for improvement of health education. Local explanatory models may differ from biomedical ones and may define the care patients seek. The current programme of tuberculosis control in less-developed countries is not focused on infected people. Preventive therapy is indeed a highly-effective method for controlling the breakdown risk in infected people (10). Knowledge and perceptions of health have become a critical tool for successful tuberculosis-control programmes (11). Also, a better understanding of local beliefs about tuberculosis is important for the improvement of the existing tuberculosis-control programmes and will achieve early and more complete case-finding (12). Ob-served age and gender differences in perceptions of attribution of cause, suggested means of risk reduction, and preferred treatment can be summarized for designing effective methods for controlling tuberculosis in South Africa. This study illustrates a method for investigating and quantifying public perceptions of tuberculosis. It then analyzes perceptions of the disease, tuberculosis, due to attribution of cause, suggested means of risk reduction, and preferred treatment among different age groups of the population sample. Materials and MethodsSample The study was conducted in Mankweng, a semi-urban area, with a population of 11,139 (latest available statistics) (13) in Limpopo province, South Africa. This area is part of a historically-disadvantaged community situated in one of the former Apartheid homelands of South Africa. The sample of 80 participants was selected on the basis of quota sampling by age and sex. Ten males and 10 females were selected from each of the following age bands: 11-19 (teen-ager), 20-34 (young adult), 35-49 (adult), and 50 (elderly) years and over. This sample is not typical of the age strata among the African population in South Africa, which is significantly weighted towards children and younger adults. However, this sample facilitated the valid consideration of disease perception, knowledge, and beliefs of older residents. After randomly assigning the first house to be visited, participants were identified by approaching every fourth house from the previously-approached one. Any available member of a particular age group was interviewed, but only one individual from each household. All the 80 participants were African/Black South Africans, namely Northern Sotho (87.5%), followed by Tsonga (7.5%) and others (5%). In the study area, according to the population census data from 1996 (latest statistics available), the majority had a house on a separate stand (57%), followed by informal dwelling/shack (20%), house/flat /room in backyard (20%), and other (3%) (13). The majority had piped water in the dwelling (56%), followed by piped water on site (36%), public tap (3%), and others (5%). Twenty-one had a per-month income of R 2,501-3,500, 20% R 1,501-2,500, 38% less than R 1,501, and 21% more than R 3,500 (1$=R 8.7, July 2002). In the study area, 5% had no formal education, 21% had primary education, 46% secondary education, and 52% more than secondary education (13). One public hospital, three public clinics, and some private practitioners are available in the study area at a distance of 1 to 10 km. Results of a community survey in the study area showed that most participants indicated that they were not to be a member of a medical aid scheme or health insurance, and their perceptions of biomedical healthcare were as follows: low acceptability of biomedical healthcare; 78% felt that medical services are poor. There was a significant relationship among not being a member of a medical scheme, subjectively poorer health status, and availability of health services. The subjectively poorer health status was also significantly related to acceptability of health services (14). Methods of data collection Information was gathered from a community population using the individual structured interview method. One trained research assistant conducted interviews in Northern Sotho, the first language in the Mankweng area. The three questions structured for the interview were adopted from Ager, Carr, MacLachlan, and Kaneka-Chilongo (15). Participants were asked the following questions: (a) What do you think causes tuberculosis?; (b) What do you do to reduce the chance of getting tuberculosis?; and (c) What do you do to treat tuberculosis if you (or someone in the family) get it? The semi-structured interview questions were translated into Northern Sotho and back-translated by a bilingual expert according to scientific standard procedures. The word tuberculosis was communicated through the Northern Sotho term "Bolwetsi Bja Mafahla", commonly used in this population. As a qualitative study, content validity was developed not through pilot study but by refinement and sharpening of the questions and continuous analysis and interpretation of data as the study progressed. Being of open-ended categories, some items were either ignored as participants volunteered data or elaborated with further probing. The researcher prompted the participant as required, and a pre-prepared interview sheet was used for recording such prompts and responses of participants. Written responses were considered by two independent raters and grouped by the nature of response. In a few instances where two or more distinct responses were given to a single question (e.g. alternative 'treatments' for a problem), responses were grouped in accordance with the initial response. Causes and means for risk reduction of tuberculosis were grouped into three main categories: (a) biomedical cause (concepts derived from Western medicine), (b) local belief systems (concepts derived from local cultural orientations), and (c) don't know (the respondents mentioned "I don't know"). Preferred treatments for tuberculosis were further grouped into three groups: (a) medical treatments (hospital, clinics, and private practitioners), (b) traditional healers and others, and (c) positive modification of behaviour (e.g. quit smoking and stop drinking). For each question, categories were collapsed until in excess of 0.80 reliability was achieved between raters. The Ethics Committee of the University of the North approved the study protocol. Participants were asked for verbal consent and in the case of a child from the parent as well, and permission was obtained from the local authorities. Results After content analysis, the responses were grouped under three categories: (a) Cause, (b) Risk reduction, and (c) Treatment (Table 1). The table shows that, in summary, 10 responses yielded for cause, 12 for risk reduction, and 3 for preferred treatment. Only 13.8% of the total sample perceived cause of tuberculosis as transmitted from infected people, and the perceived cause 'germs' varied between 5% in the teen-ager and over 50-year age group compared to 25% in the young adult group. The majority (63.8%) of the respondents (more than 50% within each age group) perceived the cause of tuberculosis as smoking. The second most important cause of tuberculosis was seen, especially by adults, as exposed to dust, dirty air, and chemicals (30%). Eating unclean food, using dirty dishes, and drinking unclean water were seen as a cause of tuberculosis by 30% of the participants aged 50 years and above and by 10% of young adults. Apart from smoking, other lifestyle factors, such as drinking alcohol, were seen as a cause of tuberculosis by 9% of the participants. The majority (66.3%; more than 50% in each age group) of the sample suggested as a means of tuberculosis risk reduction to stop or avoid smoking, followed by always keep body and house clean (13.8%), to avoid chemicals, dust, and dirt (12.5 %), regular check-up (12.5 %), to avoid infected people (11.3%), eating clean food, drinking clean water, using clean dishes (10%), etc. Most (87.5%) participants preferred medical treatment for tuberculosis, 8.8% preferred tuberculosis treatment by going to church or a traditional healer, and 6.3% mentioned positive modification of behaviour, e.g. quit smoking and stop drinking. From Table 1 the responses relating to 'cause of tuberculosis' were summarized and grouped into biomedical concepts of disease transmission (13.8%), local belief systems (83.85%), and don't know (2.5%). Further, the suggested means for risk reduction of tuberculosis were summarized and grouped into biomedical concepts of means of risk reduction (35.0%), local belief systems (56.3%), and don't know (8.8%) (Table 2). Gender comparisons of cause, suggested means of risk reduction of tuberculosis, and preferred treatment between men and women were analyzed using chi-square tests (two-tailed levels of probability). Women (11.3) perceived biomedical causes of tuberculosis more often than men (2.5), while there were no significant gender differences regarding perceived risk reduction of and preferred treatment for tuberculosis. Data from Table 2 were separated by age group as shown in Table 3. The data were recoded into '1' (for biomedical causes of disease transmission, biomedical means of risk reduction, medical treatment, and positive modification of behaviour) and '0' (for non-biomedical causes of tuberculosis, other means of risk reduction, traditional healer, and don't know). Comparisons of age-group differences of each of the response categories, analyzed using Pearson's chi-square, did not show any significant differences regarding the perception of tuberculosis causes, suggested means of risk reduction, and preferred treatment of tuberculosis between the age groups. Correlations among age, sex, and perception of causal attribution, suggested means of risk reduction, and preferred treatment of tuberculosis were analyzed by Spear-man correlation. Results indicated significantly low relationships among gender, perceived cause, and suggested means of risk reduction of tuberculosis. Perceived causes of tuberculosis had a low relationship with suggested means of risk reduction of tuberculosis and not with preferred treatment (Table 4). Discussion The respondents had limited knowledge about the causes of tuberculosis. Only 13.8% reported biomedical causes of tuberculosis, such as germs and transmission from infected people. This study found lower knowledge among participants than that found among urban black South Africans, for example, 29% thought that germs caused tuberculosis (6). Further, the perception of biomedical causes of tuberculosis was significantly higher among women compared to men, while more men than women held local cultural beliefs about tuberculosis. This may be explained by the non-biomedical risk factors, often mentioned by men, of increased exposure of men to both work (exposure to dust or dirty air) and lifestyle (smoking or drinking alcohol). In this study, misconceptions about causes of tuberculosis included smoking, exposure to cold and dirty air, eating unclean food and water, and using dirty dishes. Similarly, in a study in Cape Town, South Africa, respondents indicated cold weather (38%), smoking (31%), and poor eating habits (29%) as causes of tuberculosis (16). The perceived cause of cigarette smoking may be associated with tuberculosis because many other lung diseases are caused by smoking, such as emphysema and lung cancer. Moreover, smoking reduces appetite among some, but not all, that can cause them to become thin; similarly, people infected with tuberculosis may become thin (17). The belief that cold may be a cause of tuberculosis may be originated from the fact that other respiratory infections are more common in winter (16). In the present study, 5% of the participants perceived heredity as a cause of tuberculosis. This finding is similar to the finding of a study in Viet Nam where older people in rural areas also believed that the cause of tuberculosis was heredity (5). This study also found that 2.5% of the respondents believed that stepping on mucus of infected people causes tuberculosis, which concurs with the findings of a previous study in South Africa (16). Having scientifically unfounded beliefs about the causes of tuberculosis increases the prejudice towards people with tuberculosis (18). In the present study, one-third of the participants reported biomedical means of risk reduction of tuberculosis, which was higher than the perceived biomedical causes of tuberculosis (14%). There was a low association between causes and risk reduction of tuberculosis. This means that not all of those who suggested biomedical means of risk reduction had biomedical concepts about the causes of tuberculosis. The suggested biomedical means of risk reduction were: always keep body and house clean, avoid infected people, eat clean food, drink clean water, and use clean dishes. Although the respondents did not indicate food as a risk, water or dishes might be contaminated with tuberculosis bacilli from infected people, suggesting that this practice could possibly reduce the risk of getting tuberculosis. Contrary to this study, it was found among Mexican migrant farm workers in the United States that the majority thought that the best method of prevention was to avoid getting to close to others with tuberculosis, followed by eating, keeping clean, and avoiding unclean air and pollution. Fifty-seven percent believed that they could contract tuberculosis by using the utensils of someone afflicted with tuberculosis (17). It is suggested that further studies should be conducted focusing on questions to clarify the knowledge and understanding of communities in South Africa on these issues. An unexpected result of this study was that no respondents suggested immunization, which is very effective in preventing tuberculosis, as a means of risk reduction, while many respondents of a study on the Philippines indicated that tuberculosis might be prevented by immunization (17). The relatively-poor understanding of the causes of tuberculosis and stigma could also be a contributing factor to low adherence to DOT in this South African context (18-20). In this study, most other suggested means of risk reduction included health behaviours, such as quitting smoking, taking regular exercise, and eating healthful food. These responses show a positive attitude towards health behaviour to prevent illness. Regular check-ups, also indicated as a means of risk reduction, could reduce the severity of tuberculosis due to early investigation and subsequent early treatment beneficial to health. Strong evidence suggests that early diagnosis is very important for tuberculosis control (4). The preferred treatment among participants in this study focused on medical treatment (87.5%). In a survey of women in Cape Town, Metcalf et al. found that all women would seek medical treatment if they had tuberculosis (16). They more frequently gave biomedical causes of tuberculosis than men, which may be considered when tailoring tuberculosis programmes. This study has several limitations. The source of information on tuberculosis was not included in this study, and the sample was based on quota sampling. Further, the validity of data collected from the young age group (teen-agers) may have limitations. Thus, one cannot generalize from the data. This study has a number of implications for healthcare workers providing care for people in Limpopo province. First, it indicates that basic knowledge on causes of tuberculosis needs to be increased for every age group in the population. Second, the subjects in this study had misconceptions about causes and risk reduction of tuberculosis. Although most subjects in this study preferred medical treatment for tuberculosis, healthcare workers should be aware of misconceptions about tuberculosis and implement a programme to increase know-ledge in the community and in schools. Conventional strategies to combat tuberculosis focus on the treatment of individual patients within the framework of a control programme and emphasize the role of education and behaviour adjustment on the part of patients, particularly with regard to compliance with a medical regimen. The application of an exclusively-biomedical model to the problem of tuberculosis appears to be ineffective and needs to include local beliefs in general, age, and gender differences about the perceived causes and treatment of tuberculosis. Less knowledge and more misconceptions on tuberculosis existed among teen-agers and older people and men who should be targeted for community tuberculosis education. Tuberculosis education in this group needs to build on existing knowledge and awareness and should focus on changing attitudes, such as misconceptions about transmission and stigmatization of the disease. Every seventh participant saw tuberculosis as hereditary, which may lead to unnecessary isolation of a whole family or clan. If people's misconceptions of tuberculosis and society's behaviour towards tuberculosis sufferers can be modified, early passive case-finding as an important part of tuberculosis-control programmes will be improved. Cause and treatment of disease, including problematic area of non-compliance, need to be understood taking into account the social environment of patients, including living arrangements, belief systems, economic conditions, and the nature of community health services. AcknowledgementsThe authors are grateful to the University of the North, South Africa, for funding the study. References
© 2005 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn05009t3.jpg] [hn05009t4.jpg] [hn05009t2.jpg] [hn05009t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}