 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 23, No. 2, June 2005 , pp. 105-120 Potential Impact of Adjustment Policies on Vulnerability of Women and Children to HIV/AIDS in Sub-Saharan Africa Roberto De Vogli; Gretchen L. Birbeck; Department of Epidemiology and
Public Health, University College of London,
1-19 Torrington Place, London WC1E
6BT and African Studies Center and
Departments of Neurology and
Epidemiology, Michigan State University,
138 Service Road,
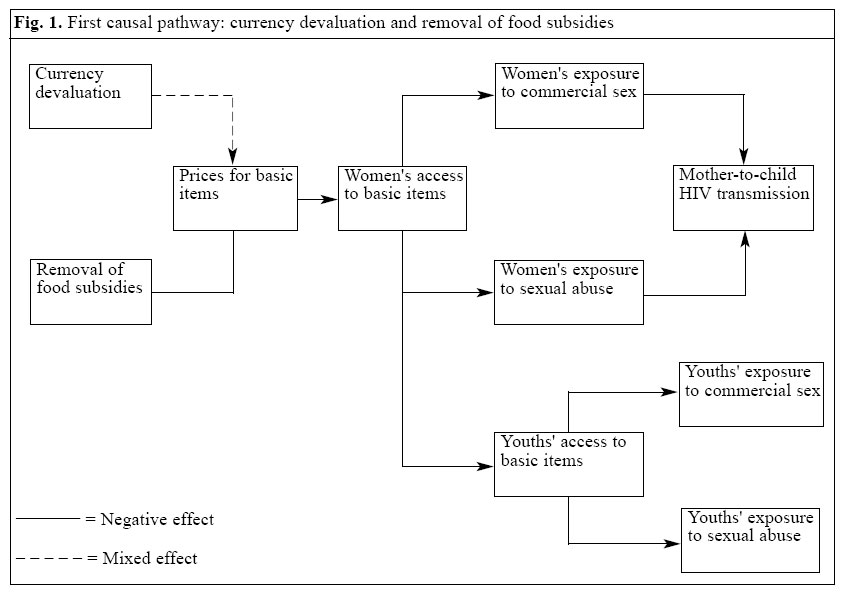
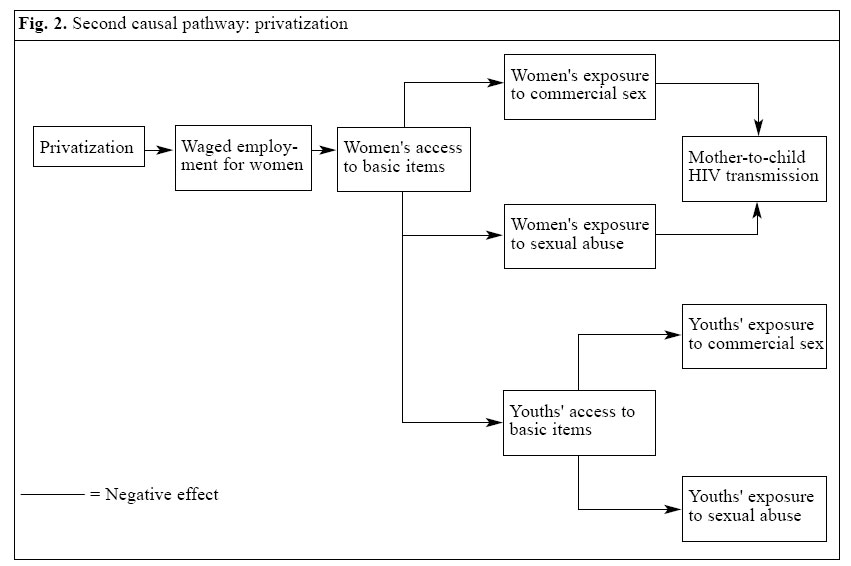
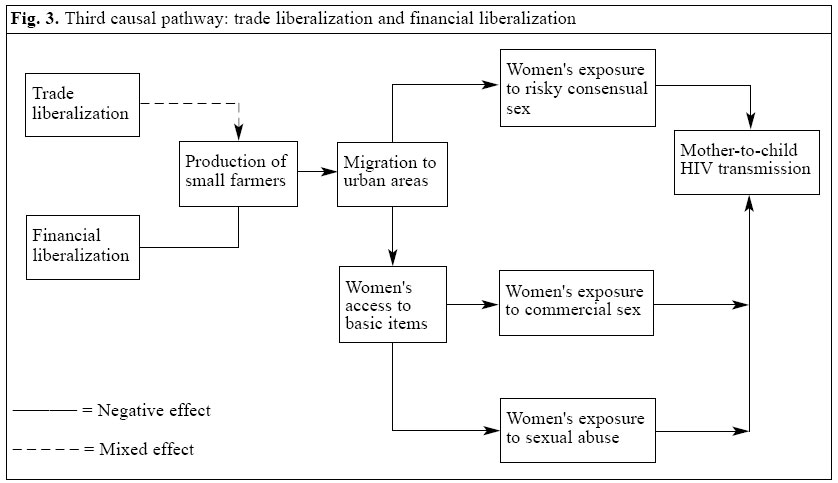
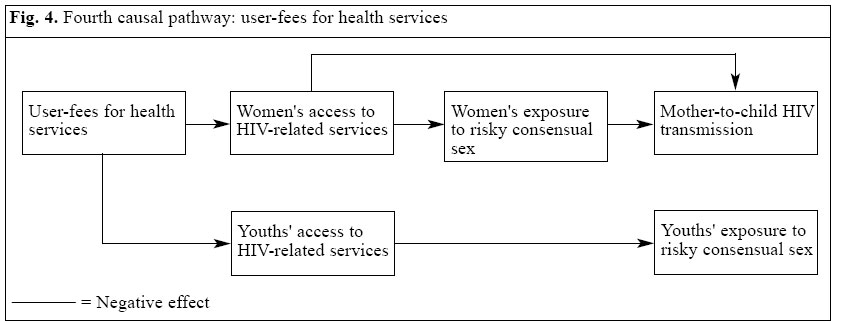
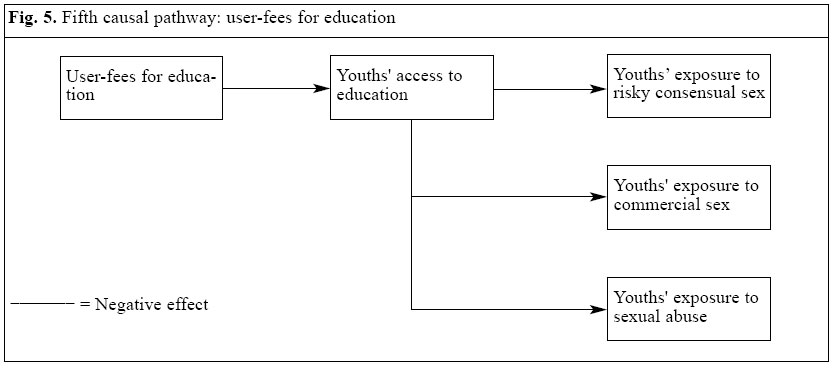
A217, East Lansing, MI 48824-1313, USA Code Number: hn05013 ABSTRACT This paper evaluates the potential impact of adjustment policies of the International Monetary Fund and the World Bank on the vulnerability of women and children to HIV/AIDS in sub-Saharan Africa. A conceptual framework, composed of five different pathways of causation, is used for the evaluation. These five pathways connect changes at the macro level (e.g. removal of food subsidies) with effects at the meso (e.g. higher food prices) and micro levels (e.g. exposure of women and children to commercial sex) that influence the vulnerability of women and children to HIV/AIDS. Published literature on adjustment policies and socioeconomic determinants of HIV/AIDS among women and children in sub-Saharan Africa was reviewed to explore the cause-effect relationships included in the theoretical framework. Evidence suggests that adjustment policies may inadvertently produce conditions facilitating the exposure of women and children to HIV/AIDS. Complex research designs are needed to further investigate this relationship. A shift in emphasis from an individual approach to a socioeconomic approach in the study of HIV infection among women and children in the developing world is suggested. Given the potential for adjustment policies to exacerbate the AIDS pandemic among women and children, a careful examination of the effects of these policies on maternal and child welfare is urgently needed. Key words: Structural adjustment policies; HIV; Acquired immunodeficiency syndrome;Socioeconomic factors; Impact studies; Women; Child; Sub-Saharan Africa Introduction The social and economic impact of the adjustment programmes of the International Monetary Fund (IMF) and the World Bank in developing countries has been a source of heated debate over the last two decades. Research on the effects of these policies has led to contradictory conclusions. [In this review, adjustment policies or programmes refer to stabilization policies implemented by the International Monetary Fund and structural adjustment policies implemented by the World Bank. Both are designed to reduce basic imbalances in the economy. Stabilization policies reduce imbalances in the external accounts, while structural adjustment policies are designed to reduce imbalances in domestic resources use.] A number of World Bank evaluations indicate that 'adjuster countries' generally succeed in improving health, education, and social welfare programmes compared to 'non-adjusters' (1-3). Based on such studies, the World Bank concludes that adjustment programmes do not necessarily adversely affect vulnerable populations. Further-more, the World Bank believes that reforms that include these reforms are necessary for poverty eradication in developing countries. On the other hand, publications from UNICEF and from representatives of academic institutions and non-governmental organizations (NGOs) indicate that adjustment policies may be particularly harmful for the most vulnerable populations. In "Adjustment with a human face", UNICEF reports studies from several developing countries which indicate that adjustment policies have negatively affected the health status of women and children (4). Evidence suggests that the adjustment programmes may also create conditions favouring societal vulnerability to HIV/AIDS (5). Unfortunately, no study, to date, has systematically evaluated the relationship between IMF/World Bank economic reforms and the vulnerability of women and children to HIV/ AIDS. This paper reviews what is known regarding the social and economic consequences of adjustment policies on maternal and child welfare and explores the potential impact such consequences may have on the vulnerability of women and children to HIV/AIDS. We approach the impact of macroeconomic adjustment policies from a conceptual perspective. Our theoretical framework illustrates how adjustment policies may influence the predisposing factors for impoverishment of women and exposure of children to HIV/AIDS in sub-Saharan Africa. A set of causal pathways that relate the implementation of these macroeconomic measures to increased vulnerability to well-established HIV-related risk factors among mothers, infants, and young adolescents is proposed. The underlying assumption is not that adjustment is the only cause of vulnerability of women and children to HIV/AIDS. Antecedent predisposing factors, such as poverty and inequality, are responsible for the vulnerability of women and children to HIV/ AIDS in the first place. However, adjustment policies may further contribute to a socioeconomic environment that facilitates the exposure of women and children to HIV/AIDS, especially when their implementation is not accompanied by specific measures protecting the most vulnerable populations. A substantial proportion of studies addressing the social and economic changes accompanying adjustment programmes are reviewed here to assess the plausibility of the hypotheses of the theoretical framework. Methodological Obstacles to Evaluating Adjustment Policies The validity of studies analyzing the effects of adjustment policies on vulnerable populations is often limited by a number of methodological obstacles. In general, the different approaches used in such evaluations are judged in terms of their ability to provide estimates of the counterfactual. Two types of designs--pre- and post-adjustment assessment and cross-country analyses--have been widely used. Both designs have limitations. The pre- and post-adjustment assessment design cannot separate the effect of the adjustment programmes from exogenous factors, such as wars, natural disasters, and social tensions. Another problem in examining indicators before and after the implementation of adjustment programmes is the scarcity of reliable time-trend data, including the difficulty of operationalizing variables, such as privatization or liberalization. Moreover, the high number and complexity of interrelationships among variables of interest, including confounding factors, make it extremely difficult to establish causal links between macro changes and modifications at the meso and micro levels. Control conditions for sorting out these interrelationships are often difficult to identify. Some countries adopt the entire set of recommended economic reforms, while others implement only select reforms, but not all of those recommended. Furthermore, countries adopt adjustment policies for varying amounts of time: some of them for a decade or more, others only for a few years. Cross-country analyses also present limitations. The main problem of these types of studies is the underestimation of country-specific characteristics, such as political and social structures, and natural resources. Also, the depth with which an adjustment programme is implemented is critical in determining the programme's effect on vulnerable populations. Studies relying on cross-country analyses usually measure an adjustment programme by using the loan as a proxy variable without giving any indication of the degree of implementation of the programme. The World Bank's somewhat arbitrary distinction among "Early Intensive Adjustment Lending", "Other Adjustment Lending", and "Non-Adjusting Lending" probably fails to truly reflect the implementation methods (6). Finally, there are methodological problems common to both pre- and post-adjustment assessments and cross-country designs. For example, it is crucial to distinguish between the effects of macroeconomic policies and the effects of finance that accompanies the programmes, including those of the international financial institutions, co-financing from bilateral donors, and possible debt relief. Both pre- and post-adjustment assessments and cross-country comparisons fail to account for the foreign aid and investment benefits available to 'adjusters' versus 'non-adjusters'. Most of these studies use secondary datasets that, in developing regions, are often insufficient and unreliable. Also, many studies rely heavily on aggregated data that provide limited information on sub-populations. Poor women and children in such analyses may be affected by the ecological fallacy. Finally, there are no analyses of the impact of adjustment policies on vulnerable populations that have used the incidence of HIV infection as an outcome, probably because of the difficulties relating to accessing such data across different social strata of the population. Despite these limitations, studies evaluating the health effects of adjustment policies are of extreme value in advancing our understanding of the complex interrelations connecting different sectors of society. Lack of rigorous research designs and reliable population-based data are problematic issues, but this should neither stop the development of future research on the impact of adjustment programmes nor prevent countries and/or lenders from taking action against their unintended effects. Socioeconomic Forces Driving the HIV Epidemic Among Women and Children Vulnerability of women and children to HIV/AIDS AIDS in sub-Saharan Africa directly and indirectly devastates the lives of millions of women and children. According to the joint United Nations Programme on HIV/AIDS (UNAIDS) and the World Health Organization, 19.2 million women and 3.2 million children aged less than 15 years are living with HIV/AIDS in the world. Almost two-thirds of them reside in sub-Saharan Africa. In 2003, over one million women and approximately 610,000 children died from AIDS. World-wide annually, two million women and 700,000 children are newly infected with HIV. This occurs primarily in sub-Saharan Africa where infant mortality rates are soaring because of AIDS (7). The U.S. Bureau of the Census estimated that "by the year 2010, if the spread of HIV is not contained, AIDS may increase infant mortality by as much as 75% and mortality in children under five by more than 100% in those regions most affected by the disease" (8). According to the UNAIDS, the majority of children with HIV/AIDS have been born to infected mothers. Most of these mothers contracted the virus through risky consensual sex, sexual abuse, and commercial sex and then infected their children through vertical transmission. Few of these women have access to information and services for the prevention of mother-to-child HIV transmission, such as antiretroviral medications, during pregnancy (9). Older HIV-positive children are infected through other routes of transmission, such as sexual abuse, commercial sex, and consensual sex with peers. This group includes disenfranchised populations who have been particularly affected by the epidemic, such as young sex workers, injecting drug users, street youths, child labourers, and imprisoned youths (10). Given the factors contributing to childhood HIV, UNICEF has concluded: "women and children's exposure to HIV/AIDS is principally caused by a lack of protection from human rights abuses". Human rights abuses include sexual abuse, commercial sex, and sexual exploitation in addition to lack of access to basic human needs, such as food, shelter, healthcare, and education (11). Children living in, what UNICEF terms, "especially difficult circumstances" are at an increasing risk of HIV infection mainly because of the miserable socioeconomic conditions in which they live. These circumstances are associated with impoverishment of women and social, economic and political factors at the local, domestic and international levels. Socioeconomic conditions of women and children are determined by a series of hierarchical factors that interact with one another at different levels of their eco-system. These factors correspond to the household level (i.e. income of the family), the meso level (i.e. food prices, real wages, employment opportunities), and the macro level (i.e. economic policies, health policies, social welfare systems). The latter level is particularly important: macroeconomic changes modify the meso-economic conditions that, in turn, are transmitted down to the household level. Macroeconomic measures, such as adjustment policies, may have an impact not only on macro-economic indicators, such as gross domestic product (GDP) growth and the external debt rate, but also on social indicators, such as access of women and children to shelter, food, healthcare, and education. Since poor access to basic human needs may facilitate the exposure of children to HIV/AIDS, economic policies at the macro level may ultimately be related to the socioeconomic conditions that reduce or facilitate the spread of HIV/ AIDS among infants and youths. Economic reforms that decrease access to basic needs for poor households will eventually result in increased exposure of women and children to HIV/AIDS. Conversely, economic growth that leads to increased access to basic goods and ser-vices for the most vulnerable families may significantly reduce their exposure to the infection. Adjustment policies From an economic standpoint, macroeconomic measures that deal with the balance of payments of developing countries are clearly needed to undertake stabilization and maintain economic growth. A developing country hit by economic recession must implement a series of reforms to reach these goals. According to the IMF and World Bank, placing constraints on demand by monetary policies and expanding supply by changes in the market environment is the solution to unsustainable deficits. These reforms, generally called adjustment policies, are intended to promote economic development and relieve debt crisis by stimulating growth of the private sectors and by promoting free trade to make economies of developing countries more competitive in the international market. The IMF and the World Bank claim that, if correctly and consistently implemented, these policies promote economic growth with the sustained reduction of poverty (2,12,13). Adjustment policies mainly consist of: a. currency devaluation and financial liberalization; Since 1980, most sub-Saharan African countries entered into one or more adjustment programme(s) of the IMF/ World Bank. Many of these programmes have not been implemented as prescribed by the World Bank and IMF, but as implemented, these policies have not produced the expected results in terms of economic growth and reduction of unsustainable debt. A World Bank study of 26 African countries that implemented adjustment policies concluded that six countries had a large improvement in macroeconomic indicators, nine had a small improvement, and 11 had a deterioration (3). Moreover, Africa’s external debt increased from US$ 120 billion in 1980 to US$ 340 billion in 1995 (14). Several economists have criticized adjustment policies and their main assumptions. Adjustment policies assume that the macroeconomic imbalances of sub-Saharan African countries are mainly due to internal problems, such as mismanagement and inefficiency. Despite the relevance of these problems, factors beyond the control of national policy-makers (e.g. rise in oil prices, falling commodity prices, increasing international interest rates, protectionism of the developed world) have played a major role in deteriorating the economy of the region. The problem of macroeconomic destabilization derived from exogenous shocks emanating from the world market is not addressed in the adjustment packages prescribed by the IMF and World Bank (15). These institutions have been inactive in reducing growing volatility of GDP of developing countries mainly caused by banking, financial and currency crises following financial deregulation at the global level. Instead of applying their regulatory capacity to prevent financial problems and abnormal fluctuations in real exchange rates and imports, they have forced developing countries to implement orthodox domestic policies abruptly, regardless of what their initial conditions. However, policies, such as domestic deregulation and external liberalization, function primarily in settings where domestic markets are competitive and non-exclusionary, regulatory institutions are strong, asset concentration is moderate, access to public-health services is widespread, social safety nets are in place, and rules of access to global markets are non-exclusionary (16). Another major criticism is that adjustment policies fail to facilitate a progressive redistribution of income and resources to the poor, a basic prerequisite for poverty reduction. There is evidence that, in countries that have implemented adjustment policies, disparities between rich and poor and disparities between males and females have actually increased (4). Income polarization following excessive liberal economic policy regimes not only limits poverty reduction, but it also depresses the rate of economic growth. This finding has been documented by recent research efforts showing that the relationship between inequality and growth is concave: both very low and very high inequality depress growth (17-19). Theoretical Framework To study the potential impact of adjustment policies on the vulnerability of women and children to HIV/AIDS, we propose a theoretical framework used as a reference for conducting a review of the existing evidence on the topic. The target populations of the present framework include mothers and infants living in poverty and vulnerable young people. Both these groups have been identified as being at high risk for HIV infection (20). Infants whose mothers live in adverse socioeconomic conditions are particularly at risk of mother-to-child transmission of HIV infection since their mothers are frequently exposed to sexual abuse, commercial sex, and risky consensual sex. Vulnerable young people refer to children living on the street or in urban slums, imprisoned youths, young girls in the sex trade, illiterate girls, and any child exposed to labour exploitation and sexual abuse. The theoretical framework specifies the processes by which adjustment policies (causal factors) may in-crease the vulnerability to HIV/AIDS (final outcome) through reduction in access of women and children to food, shelter, basic commodities, healthcare, and education (intermediate outcomes). The causal connection among adjustment policies, access of women to basic needs, and vulnerability of women and children to HIV/ AIDS is mediated by a series of intervening variables at the meso and micro levels. The most immediate effect of adjustment policies is to modify certain existing conditions at the meso level of women and children's socio-economic system (e.g. food prices). The main effect of these economic variations is to decrease access of women to basic needs. The link between the reduction of access of women to basic needs and the vulnerability of children to HIV/AIDS is, however, mediated by another series of intervening factors at the micro level: economic deprivation increases the exposure of women and youths to sexual abuse, commercial sex, and risky consensual sex. Both meso- and micro-level factors are potentially capable of increasing the vulnerability of infants and youths to HIV/AIDS. The framework is primarily unidirectional flowing from adjustment policies to vulnerability of women and children to HIV/AIDS and does not necessarily include all possible pathways linking these concepts. The framework is composed of the following five different patterns of causation: First pathway: The first pathway argues that currency devaluation and removal of food subsidies increase prices for basic items, thereby reducing access of women and youths to food, shelter, and basic commodities. This deprivation then increases the exposure of women to commercial sex and sex abuse that, in turn, increases the exposure of infants to mother-to-child HIV trans-mission. It also increases the exposure of youths to sexual abuse and commercial sex. Second pathway: The second pathway states that privatization causes a reduction of real wages and employment opportunities for women, decreasing access of women and youths to food, shelter, and basic commodities. As for the first pathway, there is an increase in the exposure of women to commercial sex and sexual abuse that, in turn, increase the exposure of infants to mother-to-child HIV transmission. Also, there is a concomitant increase in the exposure of youths to sexual abuse and commercial sex. Third pathway: In the third pathway, it is assumed that financial liberalization and trade liberalization re-duce production of small farmers increasing migration towards urban areas. This increases the exposure of women to risky consensual sex with male partners who commute to urban regions. It also increases the exposure of women to commercial sex and sexual abuse through reduction of access to food, shelter, and basic commodities. As a result, the exposure of infants to mother-to-child HIV transmission increases. Fourth pathway: In the fourth pathway, user-charges for health services reduce access of women and youths to HIV-related prevention and identification services, such as AIDS education, condoms, HIV testing, and treatment of sexually transmitted infections (STIs). Reduced access to such services among women increases their likelihood to engage in risky sexual behaviours that, in turn, increases the exposure of infants to mother-to-child HIV transmission. Fifth pathway: The fifth pathway states that user- charges for education reduce access of youths to education (especially for girls) that, in turn, increases their exposure to risky consensual sex because of their reduced capability to recognize AIDS as a threat. Also, reduced access to education increases the exposure of youths to sexual abuse and commercial sex in later life. Evidence for the Five Causal Pathways This theoretical framework was developed as part of an evidence-based review of literature (studies, articles, and published works) investigating the association between adjustment policies and the factors relating to increased vulnerability of women and children to HIV/AIDS. To combine both economic and public-health perspectives, we divided the literature review into three phases. First, we reviewed publications of the MEDNET database investigating the major social, economic and political determinants of HIV/AIDS, with particular reference to women and children in Africa. Then, we assessed major economic studies on the social and health impact of structural adjustment policies in Africa by reviewing the literature of the Joint IMF-World Bank Library. Finally, we combined information gathered to draw a comprehensive view of the issue and to shed some light on the associations proposed in the theoretical framework. First pathway: currency devaluation and removal of food subsidies Analyses of the effects of currency devaluation on prices for basic items, such as food, housing, and transportation, lead to controversial conclusions (Fig. 1). Prices for basic commodities rise after the adoption of the adjustment policies because currency devaluation increases the cost of imports. In Zambia, devaluation increased the cost of bread from 12 kwacha a loaf in 1990 to 350 kwacha in 1993 (21). In Senegal, after currency devaluation, inflation rates dramatically increased especially for daily food and health products (22). In Kenya, the real price for maize rose by 29% between 1982 and 1983 (23). In Tanzania, commodity prices skyrocketed as a result of devaluation (24). Despite these results, there is also evidence that currency devaluation may be an appropriate solution to pre-vent a further collapse of a failing economy (13). A study conducted in cocoa-growing areas of Ghana concluded that even the poorest smallholders benefited from the improved producer prices resulting from devaluation (25). If currency devaluation produces mixed effects, removal of food subsidies has a more direct impact on access to food and basic commodities, especially among low-income groups. In Zambia, after the removal of subsidies in 1985, the price of maize meal rose by 50% (26). In Zimbabwe, after eliminating food subsidies, the cost of living for lower-income urban families rose by 45% between mid-1991 and mid-1992. The increased cost of food items results in a sharp reduction of low-income household expenditure on other basic commodities. Re-search conducted in a low-income settlement in Harare (Zimbabwe) showed that an increase in food prices following food subsidies reform decreased per-capita food expenditure among the poorest households by 15.4% (27). Women, who are responsible for ensuring that meals and basic commodities are available in the house-hold, bear the heaviest burden of price reforms and removal of food subsidies (26). Only a very small proportion of poor women are food producers (beyond their own needs) who may benefit from increases in food prices. Reductions in household expenditure are disproportionately higher in female-headed households compared to male-headed households, and both urban and rural women are adversely affected by policies that lead to increases in prices for basic items. Urban women are disproportionately affected by these policies because a large share of their food is purchased from the market (27). Rural women barely cover their subsistence with the food they produce, and with the increasing cost of food they can no longer afford to purchase other foods. In Nigeria, 85% of rural farm women re-ported reducing the number of meals per day in the household from three to two after the implementation of adjustment policies. Thirty percent reported that the family intake decreased to only one meal per day (28). Many impoverished women are forced to adopt survival strategies, such as providing unprotected sexual intercourse in return for money, lodging, and food (29,30). To earn a living, many women engage in unprotected sex with several partners, exposing themselves to HIV infection. Furthermore, women with reduced economic power have limited ability to negotiate safe sex and cope with sexual harassment, regardless of their level of knowledge and attitudes towards AIDS prevention (30). Impoverished women are more dependent on their male partners, and this increases their vulnerability to non-consensual sex and domestic violence. In fact, many HIV-positive women have contracted HIV infection through sexual abuse (29) from partners, relatives, other members of the community, and strangers. Sexual abuse, commercial sex, and domestic violence increase the number of unwanted pregnancies and HIV-infected mothers that are very likely to transmit the virus to their foetuses. There are no data demonstrating a causal link between sexual abuse or commercial sex and HIV infections among the newborns. However, a proportion of HIV-positive mothers has been infected through these routes of transmission. In Swaziland, the proportion of HIV-positive pregnant women attending antenatal clinics in 2000 ranged from 32.2% in urban areas to 34.5% in rural areas; the corresponding figures were 43.9% and 35.5% in Botswana (5). In Zimbabwe, 30% of pregnant women, aged 15-19 years, attending antenatal clinics, were HIV-positive (11). Sharp increases in the cost of living and impoverishment of women not only increase the vulnerability of infants to HIV/AIDS, but also have a negative impact on vulnerable young people. Children of poor mothers are more likely to be exposed to predisposing factors for HIV (10). Socioeconomic constraints force these children to leave school and search work to support their families. Children may also be abandoned. Youths and children living in impoverished families are more likely to live and work on the street, where they may be forced into prostitution to exchange sex for money, goods, food, or shelter (31). In Tanzania, economic and matrimonial hardships at home have been shown to increase the number of unsupervised children in urban areas. Home-lessness caused by economic problems increase the number of girls who engage in commercial sex exposing themselves to the risks of unwanted pregnancies and HIV/AIDS (24). Female children are particularly vulnerable to exploitation and abuse. Seventy-eight percent of young girls interviewed at truck stops along the Trans-Africa Highway in Kenya report exchanging sex for gifts or money (32). Girls may also be forced into the sex industry by their relatives (33), and the rate of HIV infection among such sexually-exploited children is very high. A survey conducted in Kenya showed that 30% of street girls were HIV-positive (20). Second pathway: privatization Privatization can be an appropriate reform to contribute to fiscal stability by either reducing governmental expenditure (in the form of subsidies) to state-owned enterprises or increasing government revenues through sale receipts and future tax contributions of the privatized firms (Fig. 2). This may decrease budget deficits and improve countries' credibility in the international community resulting in more access to international investment, including import-export relations with positive effects on economic growth and poverty reduction. How-ever, privatization results in significant job losses in the public sector without necessarily increasing employment in the private sector (34-36). To improve efficiency and keep production costs low, public enterprises reduce costs of labour by freezing wages and reducing employment. This results in a decline of real wages or an increase in unemployment, especially among low-income workers. During the 1980s, average real wages declined in 26 of 28 African countries (34). In Ghana, between 1984 and 1991, after privatization of the 42 largest state enterprises, more than 150,000 workers lost their jobs (31). These cutbacks in public-sector employment disproportionately affect women (4,37,38) who traditionally hold positions, such as clerical workers, cleaners, nurses, or teachers. In Ghana, the least skilled women working in the public sector lost job protection, security, and benefits as a consequence of policies aimed at increasing efficiency, while others lost employment altogether (39). Privatization not only affects women in urban areas, but also impacts those in rural areas since informal land privatization is linked to a reduction in access of women to subsistence food production (40). Unemployment, low wages, and job insecurity caused by privatization not only increase women's adoption of survival strategies, including prostitution, but also modify existing gender-related relationships. Employed women tend to be more empowered by having more opportunities for education, more experience in public life, more self-confidence and self-esteem, all basic prerequisites for negotiating safe sex with male partners (41). Conversely, unemployment, job insecurity, and reduced purchasing power increase the exposure of women to sexual harassment and sexual abuse, especially among those working in low-earning jobs (42). In Cote d'Ivoire, the economic changes accompanying adjustment policies were associated with increased marital conflict (39). In fact, gender conflict is likely to increase in households where women do not have a regular source of income or have low purchasing power (27). These studies strongly support that income for women provides an important negotiating tool in gender relations and buffers women somewhat from domestic violence, sexual abuse and, ultimately, HIV infection. Reduced employment opportunities resulting from privatization may also increase the proportion of African children forced to live on the street or work to support their families (43). In Zambia, due to privatization and retrenchment of government employees, 72,000 people lost their jobs and child labour increased nine folds among females aged 12-14-years (44). Third pathway: financial liberalization and trade liberalization Financial liberalization is one of the most criticized adjustment reforms (Fig. 3). International financial deregulation has led to economic crises in a number of countries with devastating effects on the poor. At the domestic level, liberalization of the financial system may result in an increase in real interest rates benefiting lenders at the expense of borrowers (16). These reforms coupled with removal of agricultural subsidies severely affect agricultural micro-enterprises: higher interest rates dramatically decrease access to credit for small farmers, while subsidy reform further weakens their economic activity. According to a recent report of the Structural Adjustment Participatory Review International Network (SAPRIN) for Ghana, limited access to credit was the single most important problem faced by food producers. Fertilizer reform that involved the removal of subsidies increased the price of insecticides, fungicides, and spraying machines making these inputs unaffordable for most small farmers (45). The positive effects of trade liberalization have also been reported. Import liberalization and export promotion may reduce imbalances in the import-export ratio, resulting in economic growth and reduced poverty. Developing nations, including African countries, that implemented aggressive export-promotion policies have grown faster than 'non-globalizers' (46). Presumably, this rising income for the poor is associated with improved health status. Results of a recent survey conducted in Uganda showed that poverty levels dropped significantly after trade reforms, especially among smallholders producing export crops (47). After trade liberalization, many small farmers, however, went out of business. Promotion of exports and incentives for tradable goods may lead to the replacement of food production for local consumption with the production of commodities for export, such as coffee, cotton, bananas, and tobacco. More competitive, large-scale agricultural producers often displace small farmers, who have no access to modern equipment. As rural subsistence production declines, small farmers are often forced to leave their families to migrate to urban areas for long time in search of employment, and such migration is a major contributor to the HIV epidemic in Africa (5,48-51). Effect of migration on the vulnerability of children to HIV/ AIDS has not been formally studied, but in Zimbabwe, males who leave their families for extended periods of time in search of work are more likely to engage in sexual activity with multiple casual partners in the city and are also more likely to engage in unsafe sex with prostitutes (52). Several studies indicate that migrant workers in the mining industry of South Africa significantly contributed to the spread of HIV through sexual contact with prostitutes (53-55). Women who are financially dependent upon their male partners working in the cities are often unaware of the HIV-related risks involved in consensual unsafe sex when their partners re-turn home. Moreover, these women may have little power to negotiate safe sex due to their increasing financial dependency, and this dependency may worsen their exposure to sexual abuse and domestic violence (56). Finally, women who are abandoned by their male partners often adopt survival strategies, such as prostitution (57). Fourth pathway: user-fees for health services User-fees can be an important tool to ensure the sustainability of health services, to improve the quality of care, and to require African households with adequate resources to pay for their healthcare services (2,58). However, in regions where a significant proportion of population live in miserable conditions, indiscriminate cost-recovery measures disproportionately affect those who cannot afford to pay user-charges (Fig. 4). The World Bank and other organizations which support the implementation of user-fees for health services insist that even poor households are willing to pay for higher-quality, more reliable health services. In a household survey conducted in Rwanda, most respondents, regard-less of income, indicated a preference for higher fees to assure the availability of medications (59). However, populations living on less than a dollar per day can rarely afford to pay user-fees and their inability to pay may negate their 'willingness' to pay (60). The literature repeatedly shows that introducing user-charges at STI clinics result in a dramatic drop in women's use of ser-vices (61-64). Access to free STI treatment and condoms increase their use (65-66), and the introduction of user-charges creates an obstacle to HIV-preventive behavioural practices among women. Women and youth without access to AIDS education, HIV screening, STI treatment, and reproductive health services have little control over their AIDS-related risk factors. Untreated STIs increase the risks of HIV transmission (67) as shown in Uganda where over 90% of new HIV infections were attributable to other STIs (68). The introduction of user-fees for health clinics is likely to increase the number of untreated STIs consequently producing high HIV susceptibility in women (66). These HIV-infected women infect their children through vertical transmission of the virus. Fifth pathway: user-fees for education Following the prescriptions for structural adjustment and stabilization policies, many sub-Saharan African countries reduced public expenditure on education and introduced school fees limiting access to education, especially among those children who cannot afford to pay such charges (4,36). The introduction of school fees causes a dramatic fall in primary school enrollment rates and increases the number of children who drop out of school (Fig. 5). Sub-Saharan Africa has the lowest primary school enrollment ratio in the world. This ratio fell from 77.1% in 1980 to an estimated 66.7% in 1990 (69). In a cross-country analysis, the impact of user-charges on primary school enrollment revealed that 'early adjuster countries' experienced a significantly higher decline in school enrollment rates compared to 'other adjusters' and 'non-adjusters' (70). School enrollment for girls coming from poor households fell dramatically as a result of adjustment (71). The World Bank recognized the falling primary school enrollment rates as evidence for the in-compatibility between imposition of user-chargers for socially-sensitive items and the protection of the poor (72). When user-fees are imposed, girls living in poverty are particularly affected by inability of their families to pay for education. Girls from poor families are often withdrawn from primary school to work in the household (73,74). Reduced access to education among youths and children has negative consequences for the prevention of HIV. According to the International Labour Office (ILO), children out of school are at higher risk of HIV infection (75). Lack of education undermines the capabilities of youths to perceive AIDS as a threat and to negotiate safe sex both during their early sexual experience and in their future sexual life. This decreases their use of HIV-prevention activities, such as condom use and HIV testing. The introduction of school fees is especially concerning in sub-Saharan Africa where young women are dangerously ignorant about HIV/AIDS. For instance, in Somalia, over 70% of adolescent girls have never heard of AIDS. This corresponding figure is approximately 40% in Guinea Bissau and Sierra Leone. In Kenya and Tanzania, more than 40% of adolescent girls have serious misconceptions about how the virus is transmitted (7). Moreover, young boys and girls who drop out of school and work in the household or on the street are more likely to be victims of sexual abuse and exploitation through commercial sex. This is especially serious in Africa, where sexual abuse of girls is a common practice. More than half of young Malawian women reported that their first sexual experience was coerced. In Nigeria, over 20% of young women reported being forced to have sex (76). Illiteracy and poor education are often associated with child labour. Many poor children drop out of school to enter into the workforce. The introduction of user-charges for education further encourages them to do so. Children at work are often in dangerous situations, receive minimal monetary compensation, and suffer frequent physical, mental and sexual abuse (8). Studies indicate that working girls appear to be disproportionately affected by sexual abuse by males in the employer's family (29). This is another potential source of vulnerability to HIV. Conclusion Results of this analysis are complex to interpret. Certain components of adjustment reforms, such as currency de-valuation and trade liberalization, may produce mixed effects on the vulnerability of women and children to HIV/AIDS. Other reforms, such as financial liberalization, removal of food subsidies, and introduction of user-fees for healthcare and education have a negative impact on the spread of the epidemic among poor women and children. In most cases, adjustment policies create synergies making it extremely difficult to identify their net social effects. Clearly, there is, currently, no single study capable of demonstrating a causal link between adjustment policies and the exposure of women and children to HIV/AIDS. However, this analysis provides some evidence that adjustment policies may inadvertently facilitate societal conditions that increase the vulnerability of women and children to HIV/AIDS in sub-Saharan Africa. Furthermore, our study underestimates the impact of adjustment policies since it excludes men from the analysis and does not discuss the effect of these policies on access to antiretroviral therapy among vulnerable and poor populations. Findings of this review have been limited to sub-Saharan Africa for two reasons. First, the African continent has been more impacted by adjustment policies than other regions of the world. Second, in sub-Saharan Africa, women account for 58% of adults living with HIV/ AIDS, and such percentage is much lower in other regions of the world (e.g. 24% in East Asia and the Pacific) (7). However, these results may be applicable to other developing regions provided that they have similar proportions of women and children living in economic marginalization. Well-designed studies, combining public-health data and economic indicators at the macro, meso and micro levels, are needed to further test these hypotheses. HIV researchers should be encouraged to adopt a broader approach in their evaluation of the spread of the epidemic in the developing world, including the role of socio-economic factors. Evaluation of biomedical and behavioural indicators focusing on the individual is largely insufficient to measure the determinants of HIV infection. An integrated and collective approach (which considers the macro-indicators reflecting social, economic and political factors) must be developed for monitoring the HIV epidemic. Development economists should broaden their analyses of adjustment policies to take into account not only macroeconomic aggregates, but also micro-indicators at the household levels. Appropriate social and health indicators must be developed to examine the success and failure of the structural adjustment reforms (77). Rigorous study designs are needed to overcome the methodological obstacles relating to measuring the health impact of adjustment policies. Such studies must take into account the antecedent factors and the need to specify the strata-specific effects that these reforms have on different socioeconomic groups. Combined approaches and methodologies that make use of both cross-sectional and longitudinal designs, aggregated and disaggregated indicators, qualitative and quantitative data gathering techniques are needed. Such analyses must include inter-sectoral research activities involving different disciplines and including the participation of civic society. To date, the IMF has been resistant to supporting any type of evaluation or public scrutiny regarding the social effect of its policies (78). How-ever, the World Bank has facilitated the active involvement of other societal sectors and the public in the assessment of the social impact of adjustment policies. The launch of the SAPRI, in conjunction with a network of NGOs, is a concrete example of such intention (79). It must also be acknowledged that the World Bank is, at present, the largest single investor in health in sub-Saharan Africa. Such investment may reduce the HIV epidemic through some mechanisms. However, the un-intended consequences of adjustment policies may have greater negative effects on the same health outcome. Given the potential for adjustment policies to exacerbate the AIDS pandemic among women and children, there is an urgent need to either demonstrate that such measures are not harmful to maternal and child welfare or to modify policies. The present buffering mechanisms designed to protect the most vulnerable segments of the population during macroeconomic stabilization and structural adjustment are not sufficient. The IMF and the World Bank need to provide adequate scientific evidence demonstrating the effectiveness of their policies. Failure to do so may undermine their international credibility and further exacerbate the already tragic social conditions of marginalized women and children at risk of HIV/AIDS in the developing world. Acknowledgements We are very grateful to Ella Kelly for her useful comments on an earlier draft of this manuscript. Portions of the present article were presented at the XIV International AIDS Conference, Barcelona (Spain), 7-12 July 2002. References
© 2005 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn05013f4.jpg] [hn05013f5.jpg] [hn05013f3.jpg] [hn05013f1.jpg] [hn05013f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}