 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 23, No. 3, Sept, 2005, pp. 207-214 Perceptions of Growth Monitoring and Promotion among an International Panel of District Medical Officers Dominique Roberfroid; Pierre Lefèvre; Tom Hoerée; Patrick Kolsteren; Department of Public Health, Nutrition
Unit,Institute
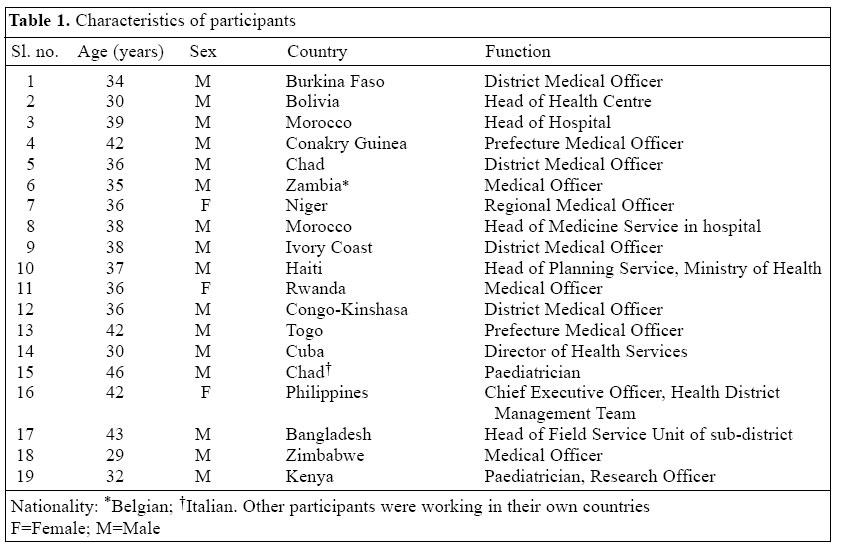
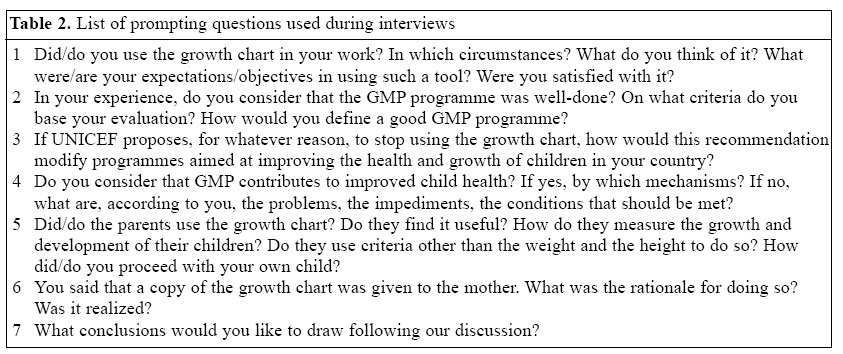
of Tropical Medicine, 2000 Antwerp, Belgium Code Number: hn05026 ABSTRACT The growth chart has been proposed as an educational tool to make the child's growth visible to both health workers and caregivers and to enhance communication between them. In the case of growth faltering, this would trigger timely corrective measures. Although the relevance of growth monitoring and promotion (GMP) has often been questioned in the literature, opinions of District Medical Officers responsible for local implementation of GMP are unknown. The aim of this qualitative research was to explore the perceptions and difficulties of an international panel of District Medical Officers regarding GMP. As an exploratory study, in-depth interviews of an international panel of District Medical Officers (n=19) were conducted. Data were coded using the QSR Nudist 5.0 software. A discrepancy between intended purposes and practice of GMP was detected at two levels. First, lack of participation of care-givers was reported. Second, the District Medical Officers expressed a restrictive interpretation of the concept of growth monitoring. The communication with parents was never reported as a means or a result of GMP, neither as an evaluation criterion of programme efficiency. The growth chart was mainly considered a tool intended to be used by health services for the purpose of diagnosis. This two-fold discrepancy between the intention of international policy-planners and practice of local programme implementers could be a crucial factor affecting the performance of GMP. More emphasis should be put on social communication and involvement of caregivers. Key words: Child growth; Growth charts; Child nutritional status;Perceptions; Developing countries Introduction The World Health Organization (WHO) defines growth monitoring and promotion (GMP) as a nutrition intervention that measures and charts the weight of children and uses this information to counsel parents so that they take actions to improve child growth (1). The growth chart is, thus, an educational tool that helps both health workers and mothers to visualize child growth (2). When growth is adequate, parents should be encouraged and advised on how to preserve that pattern. In the reverse situation, growth faltering can be detected long before any easily-observable sign or symptom of malnutrition becomes evident. This should then trigger a reaction from health workers and caregivers to take corrective measures so that the child recovers. This recovery is visualized by an upward growth trajectory (3-5). Central to all this is that parents are expected to appropriate the chart as a tool to evaluate and understand the growth and development of their children. Malnutrition is, in part, responsible for high rates of mortality of children, aged less than five years, as observed in developing countries (6,7). GMP programmes have, therefore, the potential to contribute to achieving the goals of the child survival and development revolution (2,8). Several authors have pointed out that, despite important international efforts, there is little evidence that these goals are being achieved (3,9-11). Explanations put forward relate to the poor performance of the growth chart as a measurement tool, the insufficient or inadequate training and supervision of basic health workers (12), and the poor understanding of the chart by parents, particularly those with low school achievement (13-16). In the whole debate on growth monitoring, the way mothers understand and use the growth chart has received much attention. However, how health managers, such as District Medical Officers who organize and supervise the health-system activities, view and appreciate growth monitoring has, to our knowledge, never been addressed. The aim of this qualitative exploratory study was, therefore, to document the perceptions of these professionals on GMP, their expectations of the programme, and the difficulties they face in its implementation. Materials and Methods During October-December 2000, an anthropologist with a medical background interviewed 19 District Medical Officers from South America, Europe, Africa, and Asia (Table 1). They were randomly selected from a class beginning a masters programme in public health in Antwerp, Belgium. All the interviewees had several years of experience as District Medical Officers. In-depth interviews were held in French and English and lasted 45-75 minutes. A series of structured prompting questions was used (Table 2). All interviews were tape-recorded with permission of respondents and fully transcribed. A secretary made transcripts, and the interviewer checked against the recordings to ensure ac-curacy. Data were coded using the QSR Nudist 5.0 software (QSR International Pty. Ltd., Melbourne, Australia. 2000) to facilitate cross-indexing. Codes were derived from the research themes (or research questions) and from themes emerging from data. The interviewer analyzed the data and a sociologist cross-checked to ensure their reliability (17,18). The data provided by the interviewees were treated as social constructs, i.e. as displays of perceptions, belief systems, or assumptions, not as presentation of versions of 'reality'. The transcripts were analyzed for the constructs the participants referred to, to articulate their understanding and experience of GMP. ResultsThe mean age of the 19 interviewees was 37 years. Males (16 of 19) and sub-Saharan Africans (10 of 19) were over-represented, but those proportions corresponded with the student population of that year. A large variety of experiences and opinions, reflecting the international pattern of the panel, were collected. The interviewees originated from settings where nutritional issues, malnutrition rates, literacy rates, health policy, organization, and resources of health services differed considerably (Table 1). They also had very different personal and professional histories, although all had been serving, or had served, as District Medical Officers for several years. Despite this variety of backgrounds, the interviewees were quite homogeneous in appreciating the poor effectiveness of growth monitoring. The majority expressed the opinion that, in their experience, GMP did not work the way it ought to. The interviewees emphasized a gap between intended purposes and practice. An interviewee argued, "In theory, it is a good tool, it is very interesting, but, in practice, it is different. It is, maybe, more a tool for me than for the mother… to do evaluations, statistics." (15:168-70* [*indicate transcript no. and lines respectively]). Another one added: "Of course, we did it [GMP]. There are many things done only by routine. It was there, so we kept it on, maybe, due to the lack of time to find a new strategy." (6:140-1). One even said, "That is nearly utopian!" (5:293). This discrepancy between purpose and practice of GMP was identified at two levels in the narrative of the participants: first, in their personal experiences and, second, in the expression of their understandings and perceptions of GMP. Personal experiences The interviewees evoked operational difficulties in the implementation of GMP. The most consistently-reported reason was irregular attendance of mothers at weighing sessions after completion of the vaccination schedule. The participants explained this by a lack of interest of mothers in programmes which do not display technical acts and visible effects. Mothers were said to use their own criteria to evaluate the growth and health of their children and to visit health services only for obvious ill-ness of their children.
The weak capacity of awareness campaigns for motivating parents to adhere to the programme was also underlined. The District Medical Officers attributed this failure partly to the low motivation of health workers for performing GMP activities. Low competence and heavy workload of field staff were presented as obstacles to GMP [This was particularly mentioned in sub-Saharan countries where the responsibility of GMP is most of the time taken by basic health workers], although it was not clear why these two limitations should have affected GMP more particularly than other health activities. Other limitations of the highlighted growth monitoring related to the capacity of response of parents to the information provided. The District Medical Officers frequently stated that parents failed to understand the growth chart, mainly because they are illiterate or not educated. One interviewee explained: "Because, in our country, they are illiterate. They do not understand too much what is written on it [the growth chart], it is not too much their concern." (1:341). Other interviewees were more subtle in their explanations: "They [health agents] also think that it is not that important that mothers understand, because the understanding point is quite low, you see." (16:58-61). "But I am wondering if she [the mother] really understands. Because it is simple, but sometimes nurses also have difficulties to fill in the growth chart." (15:209-10). The District Medical Officers also related the lack of response to the messages to low food accessibility and, thus, limited applicability of nutrition advice in some contexts, as reported in the following quote: "But they know it, they know that the child does not eat very well because it is the same meal every day. What are you going to propose? You are not going to propose anything because she won't have the capacity to apply it. This is a problem. Thus, I think that they are right not to come to be repeated the same thing again and again." (7:515-19). Understanding and perceptions of GMP The above results show that the explanations provided for the perceived malfunction of GMP relate much to operational problems and to the demand of the population for curative and technical, but not promotional, ser-vices. The same opposition between technical (visible, curative) and intuitive (invisible, preventive, or promotional) aspects of care can be found in the narrative of the interviewees. Actually, the District Medical Officers endorsed consciously or implicitly the primacy of technical aspects over promotion of health and growth. One interviewee gave this revealing pun: "A malnourished one is not going to contaminate somebody else. He does not carry much weight in the society." (9:389). Another interviewee added: "Yes, I always said that the mother has not come to learn that her child gained weight or not. She has come for you to do something else. You do the vaccinations." (18:201-3). About criteria used by mothers to evaluate the growth of their children, the District Medical Officers consistently considered them subjective, approximate, and intuitive. However, most District Medical Officers were unable to describe what these criteria consisted of. One interviewee, for instance, said, "Their criteria give an idea but this is not something that is very acute…. We are giving GMP criteria in a scientific way, they [the parents] are not up to that point, they have a very general idea." (17:356-7). The ambiguity is obvious in this interviewee: "Thus, I think that mother's perception is a criterion that cannot be really defined, but I believe it is important even if it is intuitive." (5:176-77). Thus, mothers are said to come mainly for vaccinations because this is part of the technical sphere under the responsibility of health services. For the majority of District Medical Officers, communication was not a primary objective. Some interviewees even tended to consider communication as a 'no-act', while weighing was considered as the technical justification of their presence in GMP. As summarized by one interviewee: "Finally, to weigh, as I said previously, demonstrates to the mother that an act is done…. Second, it is also an act, not a medical one, but an act made by the health agents that can encourage the mother to come back the next time." (5:132-5). The same interviewee went on talking about village volunteers: "Their task is much more to gather mothers and to be willing to listen to them but they do not act." (5:344-5). From this perspective, communication with parents using the growth curve is secondary. It was never either reported as an objective of GMP, or as a criterion to evaluate the programme efficiency. The growth chart was considered to have mainly diagnostic purposes and used for the health information system. For most interviewees, the growth chart was given to caregivers for preservation and transfer of information on vaccinations and diseases, not for motivating parents to monitor the child's growth: "I find it useful to not lose information. But if there were another means, better to get the information, I think we can let it [the health card] down." (12:225-7). The following quote is even more direct: "The objective is not to discuss with parents, to educate them but to determine if the child is malnourished or not. I think that, with that objective, we do not have to discuss with the mother to know if the child gained weight or not." (9:295-7). When growth faltering is detected, the focus is on unilateral transmission of information and recommendations rather than on genuine communication with care-givers. The interviewees rarely described balanced and specific exchange of information between caregivers and health workers. One of them did mention a satisfactory ability of his staff to interact with caregivers but perceived an imbalance in the communication process: "This is my feeling, my understanding: health agents, nurses, and doctors can speak well but often cannot listen. Maybe, those messages and advice will work much better if one can develop the capacity to listen." (2:207-10). Some interviewees acknowledged the dichotomy. They justified it as the result of their professional training and its focus on curative care, but also because health professionals tended to give more value to technical acts: "Yes, you are health agents. Yes, you are here to fight against diseases, to heal people. It is how it is said during your training or even on several occasions…." (1: 644-5). "The health workers are more concerned by immunization because each single case is checked by us, and this is transmitted at the district level. Much emphasis is given nationally on immunization." (17:260-2). Finally, the gap between what should be done and what is actually implemented gave the feeling to some medical officers that GMP was a frustrating but compulsory routine prescribed by national and international agencies: "This is an activity of the Ministry of Health, thus we cannot forget it because of the risk of being reprimanded…. It is the WHO, the UNICEF which advised to do so", commented this interviewee. (13:363-71). Another interviewee confirmed it: "I would say that most of the time we do it because we were told to do so." "The WHO told us that it was useful, important, it was interesting, but I think that, in every-day practice, with some experience, you can manage without the growth chart." (15:66-9). Others dealt with the contradiction by considering that the programme had still a role to play because there was no relevant alternative or the growth chart was useful to health services: "But even so, it is a tool for the management of activities that we can maintain." (19: 154-7). "And before abolishing, you need something to replace it, a valid alternative, and we do not have it." (16:143-4). Discussion This study was exposed to two potential biases. First, the interviewed District Medical Officers constitute a particular group, which might limit external validity. They were all starting a masters programme in public health in a European country. Their representativeness is, therefore, limited. The relatively high degree of coherence among the interviewees, despite the variety in backgrounds, could be explained by an affiliation to a common professional sub-culture, the field of international health. Second, the content of the interviews could have been influenced by the fact that the interviews took place in the institutions where the interviewees were studying. Each interview was led by an anthropologist employed by the same institution (19). Since the course programme puts emphasis on participatory processes and the provision of healthcare in a process of communication with the population, some answers, considered more acceptable, could have been forwarded. However, if these elements would have played a role, we would have expected more answers mentioning health service activities committed to communication and empowerment of caregivers. Although all the interviewed health professionals agreed on the sub-optimal functioning of GMP, they have a rather limited understanding of the determinants for this failure. The quoted operational difficulties are very consistent with previous studies. The drop-in compliance after the immunization schedule is completed has often been mentioned and raised questions about the real acceptability of GMP by caregivers (20). Although studies re-port mitigating results on the understanding of the chart by caregivers, overall scores are low (13,21-25), and the association with literacy is quite consistently reported (13). Determinants relating to the understanding of the growth chart and of GMP by health workers themselves were never mentioned, although it has been cited as a potential crucial element (26-29). For instance, it was shown that when health workers had a correct know-ledge of GMP, a substantially higher proportion of growth charts was maintained (24). One potential explanation for low rates of comprehension reported in mothers, as mentioned by some interviewees, could be due to low comprehension of the objectives of GMP by health workers, resulting in a limited communication (20,21,25,26). A study in India reported that there was a gap between knowledge and skill for interpretation of growth-chart data among the assessed Child Development Project Officers (30). Twenty-four District Medical Officers working in the same setting had a sub-optimal know-ledge about GMP (31). Some authors have proposed that nutrition education could be more effective by making it more specific, action-oriented, individualized, and relevant (10,32,33). This can only be achieved if clear algorithms for decision-making are available, and if health workers are trained in social communication (32). Unfortunately, these conditions appear to be rarely fulfilled under field conditions (14,15,20,26-28,34,35). Our study also revealed that most interviewed medical officers, by lack of understanding or conviction, did not attach great importance to the communication process theoretically underlying GMP. This is a striking finding as communication is central in the concept of GMP and as District Medical Officers bear the responsibility of implementing GMP programmes at the local level. We propose two main hypotheses to explain the poor results of GMP worldwide: irrelevancy of the concept or poor programme implementation (36). Our study widens this second hypothesis. If caregivers poorly understand the growth chart, this might be the final con-sequence of a misunderstanding between international policy-makers and local implementers. Indeed, in the interviews, GMP appeared quite secondary in primary healthcare and communication quite secondary in GMP. It might be as well that the two hypotheses are strongly interrelated: to translate one concept (GMP) into universal practice with one same tool (graphical representation of the growth) in various cultural contexts and nutritional situations/settings could be considered a priori irrelevant. The question can be raised: is this conceptual and technical dominance compatible with the idea of communication imbedded in GMP? What constitutes adequate growth does not necessarily overlap among lay people and health professionals (37,38). This point has too often been overlooked. In Ghana, for instance, weight variation is only one indicator among many others traditionally used by caregivers to assess the nutritional status of their children (39). In promotion as in evaluation of GMP, the significance of lay perceptions and behaviours concerning child development has seldom been recognized within the context of more 'modern' approaches based on western concepts of health and disease. The important international promotion of the growth chart might not have taken various cultural definitions of adequate growth enough into account so far (40-43). The attribution of growth faltering to a lack of information leading to inappropriate behaviours is a linear and simplistic paradigm still too often met in GMP practice. This approach does not recognize the complex interplay of the factors behind child growth and development. To have a future, GMP practice needs to re-focus on the child as a whole taking into account his/her health, growth, and development, and his/her family and socio-economic environment. Caregivers should, therefore, be involved in the process to bring together the observations and measurements made by both mothers and health workers (21,33,41,44,45). Developing and implementing such an approach is challenging. It requires new ways of working in health services, reviewed training curricula of health personnels to help them centre on the child and improve their attitudes and communication skills (46). In that process, it will be particularly crucial to convince medical officers that communication with families represents a major skill for health workers. Acknowledgements The authors would like to thank the students of the Inter-national Course in Health Development 2000 for their participation in the study. References
© 2005 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn05026t1.jpg] [hn05026t2.jpg] |
| |||||||||

{kind=link}
{kind=link}