 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 23, No. 3, Sept, 2005, pp. 215-221 Acceptability of and Adherence to Dispersible Zinc Tablet in the Treatment of Acute Childhood Diarrhoea Dilruba Nasrin1 , Charles P. Larson1,2 , Samina Sultana1 , and Toslim U. Khan3 1 Health Systems and Infectious Diseases Division, ICDDR,B: Centre for Health and
Population Research, GPO Box 128, Dhaka 1000, Bangladesh, 2 Department of Pediatrics,
Department of Epidemiology, Biostatistics and Occupational Health, McGill University,
Montreal, 1020 Pine Ave West, Montreal, Quebec H3A 1A2, Canada, and 3 Research Department,
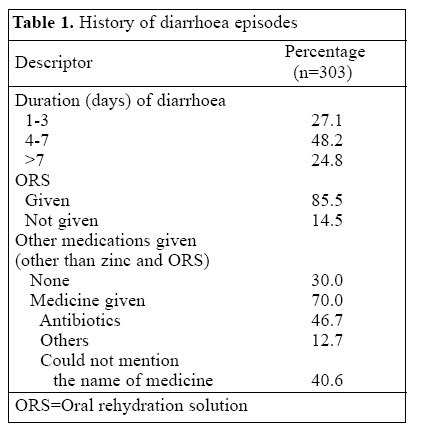
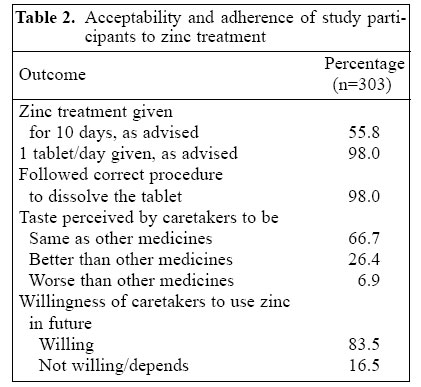
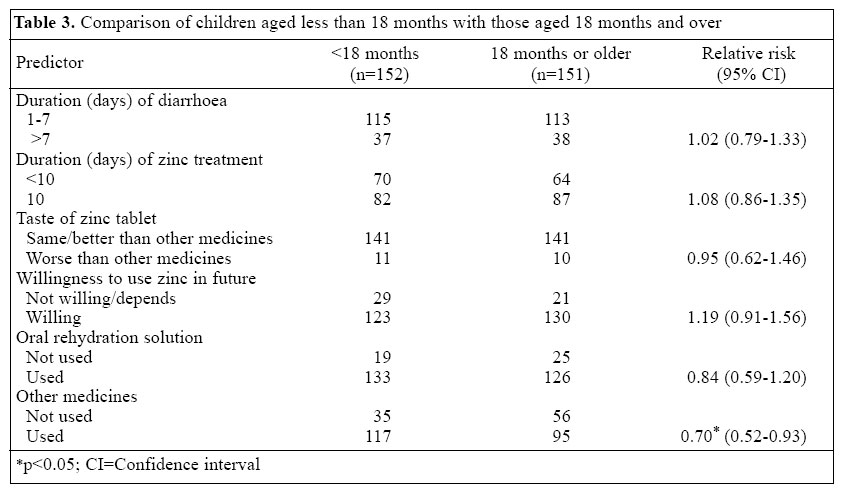
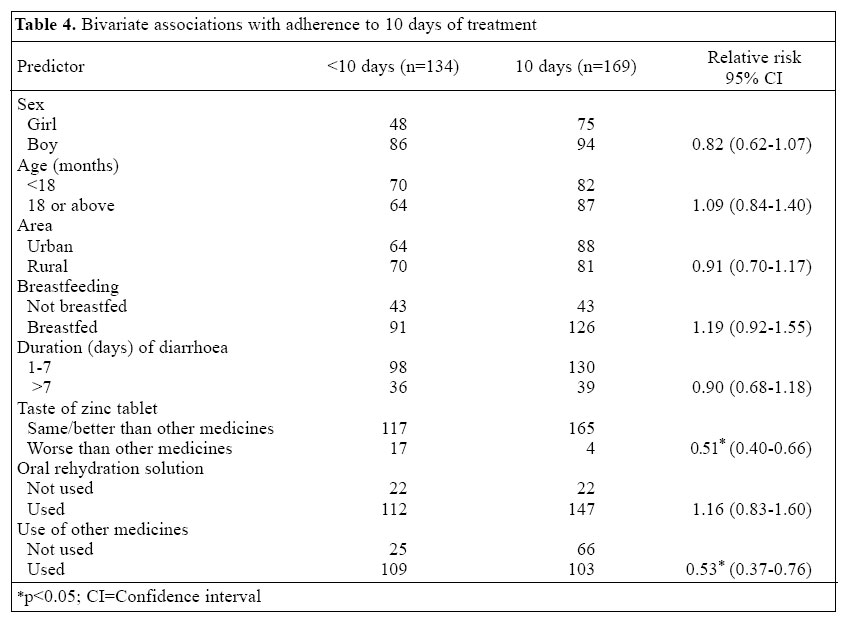
Social Marketing Company, SMC Tower, 33 Banani Commercial Area, Dhaka 1213 Code Number: hn05027 ABSTRACT Zinc treatment is now recommended by the World Health Organization as part of the routine management of acute childhood diarrhoea. A dispersible zinc tablet formulation was developed taking into account the taste, cost, and feasibility to distribute and store. Only limited information is available on the acceptability of and adherence to dispersible zinc tablet. No study has formally assessed whether the formulation is acceptable to children and if caretakers can adhere to the instructions regarding preparation, dosage, and duration of treatment. This community-based study aimed at determining the acceptability of and adherence to a dispersible zinc tablet formulation in a cohort of children (n=320) aged less than five years. Caretakers of children with acute childhood diarrhoea were prescribed zinc tablet treatment and followed up after 2-3 weeks. The formulation was acceptable to children; 90.1% of 303 caretakers perceived that the tablets were equally or even more acceptable to their children com-pared to other medicines. Ninety-eight percent of the children received the standard dose of one tablet per day, and 55.8% completed the full 10-day course of zinc treatment. Adherence rates did not vary by age or gender of the child. These findings indicate that the tablet formulation is acceptable, but further efforts are required to enhance adherence. Key words: Diarrhoea, Acute; Diarrhoea, Infantile; Zinc; Zinc deficiency; Community-based studies; Cohort studies; Bangladesh Introduction It is estimated that diarrhoeal diseases cause nearly two million deaths of children aged less than five years each year, with 98% of these deaths occurring in developing countries (1). Zinc deficiency is an important predictor of early childhood morbidity and mortality due to diarrhoea (2). This is important because, in nearly all developing countries, zinc deficiency is highly prevalent (3) and children aged less than five years will experience 4-6 episodes of acute diarrhoea each year. Over the past decade, it has been consistently demonstrated that zinc given as a treatment for acute childhood diarrhoea is effective in reducing the severity and duration of a diarrhoeal episode and, over the next 3-6 months, it decreases the risk of subsequent diarrhoeal illness and non-injury death (4-6). It is estimated that the successful scaling up of zinc as a treatment for childhood diarrhoea would lead to 400,000 fewer diarrhoea-related deaths per year (7). Given the evidence in favour of effectiveness of zinc, the World Health Organization (WHO) commissioned a private manufacturer of nutritional products for disadvantaged populations (Nutriset Ltd., France) to develop a zinc formulation that would effectively mask the taste of zinc, could be mass-produced at a low cost, and could easily be distributed and stored. With the tech-nical contribution of Rodael Laboratories (in France), a dispersible tablet formulation was developed that has now been used in several field trials on effectiveness in Africa and South Asia. The tablets contain 10-20 mg of zinc sulphate, prescribed once per day for 10-14 days. Although no problem with acceptance of the tablets has been reported, this has not been formally assessed. In addition, adherence to a 10-day treatment regimen is recognized to be an important, potential barrier to successful scaling up of zinc as a treatment that requires monitoring within normal field settings. Zinc is not entirely unknown in South Asia. Multiple zinc syrup products are currently marketed to improve growth of children, increase their appetite, facilitate digestion, and reverse weakness following a recent illness. Zinc is not generally recognized to be a treatment for childhood diarrhoea. The proposed dispersible tablet formulation has several advantages over syrups. For example, the tablets are easier to distribute and store, less costly to produce, and are easier for mother to handle and keep track of the number of days given. From a marketing point of view, tablets can be set apart from syrups and uniquely positioned as a treatment, as opposed to a micronutrient supplement. Prior to committing to the tablet formulation, the public- or private-sector investors in technology transfer, production, and marketing of the product will require assurance that the product is acceptable to young children and that treatment instructions are easily adhered to by caretakers. The taste, texture, and appearance of a medication and the schedule of administration can affect acceptability of and adherence to a treatment. The purposes of this investigation were to (a) determine whether or not Bangladeshi children aged less than five years, experiencing an episode of acute childhood diarrhoea, would find the dispersible tablet formulation acceptable and (b) document to what extent caretakers adhere to the instructions of zinc treatment as measured by its preparation and duration of treatment. Materials and Methods Study design This was a community-based study in a cohort of children with acute childhood diarrhoea, who had been prescribed dispersible zinc tablet (one 20-mg tablet per day for 10 days). Ten-tablet blister packs were distributed to selected drug-sellers by sales officers of the Social Marketing Company (SMC), a private, non-profit marketing firm that promotes, distributes, and sells low-cost, primary-care products in the health sector. A home-visit was arranged 2-3 weeks later to assess acceptability of and adherence to the instructions for zinc treatment. The study was carried out from February to April 2004. The Research Review Committee and the Ethical Review Committee of ICDDR,B: Centre for Health and Population Research approved the study as a part of the "Scaling up zinc for young children (SUZY) Project." Study site The study was conducted in four sub-districts in Dhaka division, Bangladesh. These sites were a convenient sample selected by the SMC. Within each sub-district, one SMC sales officer, purposively selected, distributed the zinc blister packs to five rural and five urban drug-sellers included in his distribution list. Each drug-seller was provided with 20 blister packs free of charge. Study population The study population included children aged 3-59 months with an acute diarrhoea episode, whose caretakers sought assistance from one of the selected drug-sellers and were provided with the zinc blister pack. Sample size To identify a ±7.5% minimal difference in acceptability between children aged over and below 18 months with an anticipated 70% acceptability (p), setting the level of confidence at 95% (z=1.95), the resulting sample size estimate is 140 children per group. To adjust for potential drop-outs, we added 10 children in each group, and the final target sample of 300 children (150 in each age-group) was sought. Measurement The definitions used for acceptability and adherence are given in the next page. Acceptability: Acceptability was measured on the basis of a caretaker's report of his/her child's behaviour when given the medication. The caretakers were asked about their perception of taste of the zinc tablet given to their children compared to other medicines. The response options were better, same, or worse than other medicines. Adherence: Adherence was defined in relation to the dose given, frequency of daily administration, duration of treatment, and preparation (dispersion) of the tablets. Methodology Four sales officers of the SMC received a one-day orientation on zinc treatment. Each sales officer was instructed to select five urban and five rural outlets from their respective allocated districts, with the exception of the Mirpur zone of Dhaka city, which is exclusively urban. The sales officers were also provided with a single-page information sheet on zinc for distribution among the drug-sellers. After the completion of orientation, the sales officers visited their allocated district and recruited drug-sellers. The drug-sellers were given a short briefing on zinc treatment in childhood diarrhoea by the sales officers and were then provided with the information hand-out on zinc treatment. Each drug-seller was advised to identify and maintain a list of up to 10 diarrhoea-affected children aged less than five years, whose parents/ caretakers sought treatment. The drug-seller recorded the name, age, address, and prominent landmark near the residence of each child on the address sheet. The questionnaire was pre-tested among four urban and two rural mothers in the presence of the research investigators and was then modified according to the feedback received. The interviewers administering the questionnaire were experienced and received two-day training and orientation. To maintain interest and motivation to participate, the drug-sellers were visited by a member of the research team one week following distribution of the blister packs to them by the sales officers of SMC. Two to three weeks after distribution, the drug-sellers were visited again to collect the list of children treated. All listed families had provided them with verbal agreement for a home-visit. A verbal consent was obtained before interviewing the study participants. Data analysis Data were entered using the dBase software, analyzed using SPSS (version 11.0) and cleaned and corrected for the outliers. Next, frequency distributions were run, and outliers were identified and corrected when appropriate. Bivariate, crude analyses of association involved chi-square and t-tests for categorical and continuous data respectively; p values of <0.05 were considered to be statistically significant. ResultsThe caretakers of 320 children who were provided with zinc tablets by the drug-sellers were interviewed. All but one of the caretakers received one blister pack containing 10 zinc tablets. At least one dose of zinc was given to 303 (94.7%) of the 320 children. Reasons mentioned by the parents of 17 children who did not give zinc tablets to their children included: illness stopped, parent was suspicious of a free treatment, and fear of complications related to a new medicine. Subsequent analyses were restricted to the 303 care-takers and children who received zinc. Of them, 151 (49.8%) were rural and 152 (50.2%) urban, 180 (59.4%) male and 123 (40.6%) female, and 151 (49.8%) aged over 18 months and 152 (50.2%) aged less than 18 months. Table 1 summarizes histories of diarrhoeal episodes. Most (75.3%) episodes lasted less than one week, with a mean duration of 6.3±5.0 days. Oral rehydration solution (ORS) was given to 259 (85.5%) children. In total, 212 (70%) children were given additional medications for their illness, but 86 (40.6%) caretakers did not know the name of the medicine. Antibiotics were the most commonly-reported medications. Fifty-three percent of those who received antibiotics were given metronidazole. Table 2 summarizes the main findings. The duration of zinc treatment for these children ranged from 1 day to 10 days with the mean of 7.78±2.94 days; 55.8% received the full course of zinc treatment for 10 days. Al-though all children were given one zinc tablet per day, the caretakers of 12 children (4.0%) divided one tablet into two or more doses. The correct procedure to dis-solve the tablet in water was followed by 297 (98%) caretakers. Caretakers of 282 (93.1%) of the treated children thought that zinc tablets were equally or even more acceptable to their children than other medicines. Most (83.5%) caretakers stated that they would use zinc treatment for their children's diarrhoea in future. Reasons mentioned by the caretakers for not completing the course included: their child was cured (15.18%), vomiting (12.21%), forgot (5.28%), and child did not improve (4.29%). The data were analyzed to see if there were any differences in acceptability or compliance among children aged less than 18 months compared to those aged 18 months or older (Table 3). There were no observed age-group differences in acceptability of and compliance with zinc treatment. ORS use was not affected by age, but a higher proportion of younger children received other medicines (77.0%vs62.9%,p<0.009). We compared the children who completed a full course of zinc treatment with those who did not (Table 4). Sixty-one percent of girls and 52% of boys completed the full course. As might be expected, children who seemed not to accept the zinc tablets were more likely to stop treatment prior to 10 days. There was no statistically significant difference in age, sex, dose of medicine, and procedure to dissolve the tablet between the children who completed the course and those who did not. A higher proportion of children who did not complete the full course was given other medicines (81% vs 61%, p<0.001). DiscussionThe objective of the study was to assess the acceptability of zinc tablets among children, aged less than five years, with an active case of diarrhoea and adherence to the treatment instructions among their caretakers. These are critically important questions for potential product manufacturers and for those involved in marketing a zinc tablet formulation. Over 90% of the caretakers thought that the zinc tablets were equally or even more acceptable to their children than other medicines. Despite minimal work with the drug-sellers and the fact that zinc tablet was an unknown product to the caretakers, more than half of the study children completed the full, 10-day course of zinc treatment, and over 90% of the caretakers complied with the instructions addressing frequency of administration, dosage, and the procedure to prepare the medicine. The study has demonstrated that, in a population with no knowledge of zinc as a treatment and little experience with dispersible tablets, the formulation was acceptable, and adherence to the instructions was quite good. In a study of compliance with anti-malarial medication, compliance was greater when information was communicated directly by provider to caregiver (8). In this study, we did not observe the content of messages regarding zinc treatment communicated to the caretakers by the drug-sellers. The drug-sellers were asked by the sales officers to provide instructions to the caretakers regarding preparation, when to give, and for how long. It is unlikely that the caretakers were fully informed, as the drug-sellers did not receive formal training on zinc treatment. Only the sales officers received formal training. They, in turn, provided the drug-sellers with a one-page hand-out containing basic information. In most cases, the child's father visited the drug-seller and received the zinc blister packs with instructions, while it was the mother who administered it in the home. This leads to additional opportunities for gaps in information. For these reasons, a multi-layered educational approach that targets varied types of drug-sellers or healthcare providers and reaches consumers through mass-media marketing will be needed to fully inform parents and support a successful scaling up of zinc as a treatment. In this study, zinc was given free to the children, which might have had an influence on higher rates of compliance. On the other hand, a few caretakers refused to give zinc to their children, as they were suspicious about free supply. Reduction in cost of treatment was reported as one of the important determinants of improved compliance to pre-packaged anti-malarial drugs (9). It is anticipated that blister pack will be sold for about 25 US cents. Whether, at this price, the poorer segments of the population are reached is yet to be determined. If zinc replaces the other medications purchased, there will be no over-all increase in cost. The field research assistants were asked to verify the number of tablets given by inspecting the blister packs. In many instances, this was not possible because the packs had been discarded. Thus, the interviewers had to rely mostly on the caretaker's report, which may have led to an over-estimation of compliance. The drug-sellers were provided with a small incentive (approximately US$ 4) to participate in this survey and dispense the blister packs. This may have had an additional influence on the behaviour of the drug-sellers in recruiting children and motivating parents to comply with zinc. Taste and appearance of medication can affect acceptability and compliance. To gain a true level of compliance, it is important to monitor all the dimensions of compliance: preparation of medicine, dose, frequency of administration, and duration of treatment. In a study comparing compliance with tablet and syrup forms of antimalarials, the study found that there was no difference between the two forms in terms of duration of administration (10). However, there was a significant variation in the frequency of administration in the syrup group despite the caregivers being instructed to give medication once a day. Among the caretakers, 15% gave medication twice a day, 14% thrice a day, and 11% varied the number of times over the 3-4-day period. In the case of tablets, non-compliance was related to either administering the drug at all or not completing the course. A number of factors affect compliance with any medication. These include sociodemographic background of patients, disease characteristics, treatment practices, and health systems. Poor compliance is associated with low socioeconomic status, illiteracy, unstable living conditions, increased distance from a treatment centre, and high medical costs (11). Several treatment-related factors affect adherence. These include the complexity of the treatment regime, duration of the regime, ease of ad-ministration, previous treatment failure, the immediacy of benefits, and the occurrence of effects (10-11). Lack of knowledge, training, and support for healthcare providers about appropriate treatments and lack of incentives for healthcare providers are also associated with poor compliance. The resulting poor understanding of treatment instructions by caretakers results in errors of treatment dosage and schedule (8). The most common explanations for poor adherence to treatment are attributed to patients or caretakers and referred to non-compliance. It is logical that a caretaker will want to observe a rapid response to any medication given. On the other hand, if the illness quickly resolves, there exists a much greater likelihood of discontinuing a medication prior to the instructed length of treatment (8). Conversely, it is more likely that a medication will be stopped if the resolution of symptoms is slow or the perception of patient/caretaker is that it is not working (12). This study assessed the acceptability of the tablets among young children with diarrhoea in urban and rural household settings and adherence of their caretakers to instructions for zinc tablet treatment. The results of the study have implications on the strategy to implement a zinc scaling-up programme in Bangladesh. This is the first published study to report on the acceptability of the recently-patented 20-mg dispersible zinc tablet developed by Rodael Pharma and distributed by Nutriset Ltd. under the brand name 'Zincfant'. It is anticipated that, in countries like Bangladesh, for scaling up zinc for the treatment of childhood diarrhoea, the technology to pro-duce the tablets will be transferred to local laboratories. In Bangladesh alone, the estimated demand is approximately 50 million blister packs per year [Social Marketing Company. Personal communication, 2004]. Thus, prior to adoption of a dispersible zinc tablet formulation, health managers and providers will want to be reassured that the product is both acceptable and feasible in terms of adherence to treatment instructions. This investigation represents a limited beginning to answering these questions. The findings suggest that the formulation is acceptable to young children. Less clear is the question of adherence to treatment. We have shown that most parents find the tablet easy to prepare and do not make mistakes in preparation or daily dosage. Not surprisingly, full compliance with the 10-day length of treatment occurred in only one-half of the cases. Much greater efforts will be required, through a broad range of promotion strategies, to attain improved rates of full compliance. AcknowledgementsThe study was funded by Bill and Melinda Gates Foundation. The authors thank the four sales officers of Social Marketing Company for recruiting the drug-sellers and distributing zinc tablets and zinc information to them. The authors also would like to thank Haribondhu Sarma, Abdur Raquib, Altaf Hossain, and Palash Mutsuddi for data collection and Ms Fariha Haseen, Ms Nafisa Lira Huq, Ms Meghla Islam, and Billal Hossain for their su-pervision in data collection. The authors acknowledge the help of Ms Sumona Liza and Dr. Rafiqul Islam for their support in undertaking the pilot study. References
© 2005 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn05027t3.jpg] [hn05027t2.jpg] [hn05027t1.jpg] [hn05027t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}