 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 23, No. 3, Sept, 2005, pp. 222-230 Feeding Practices and Factors Contributing to Wasting, Stunting, and Iron-deficiency Anaemia among 3-23-month Old Children in Kilosa District, Rural Tanzania Peter S. Mamiro1,4 , Patrick Kolsteren1,2, Dominique Roberfroid2 , Simon Tatala3 , Ann S. Opsomer1 , and John H. Van Camp1 1 Department of Food Technology and Nutrition, Faculty of Agriculture and Applied
Biological Sciences, Gent University, Coupure Links 653, B-9000 Gent, Belgium, 2 Nutrition
and Child Health Unit, Institute of Tropical Medicine, Nationalestraat 155, B-2000
Antwerp, 3 Department of Food Science, Chalmers University of Technology,
c/o SIK, Box 5401, S-402 29, Göteborg, Sweden, and 4 Department of Food Science
and Nutrition, Faculty of Agriculture, Sokoine University of Agriculture,
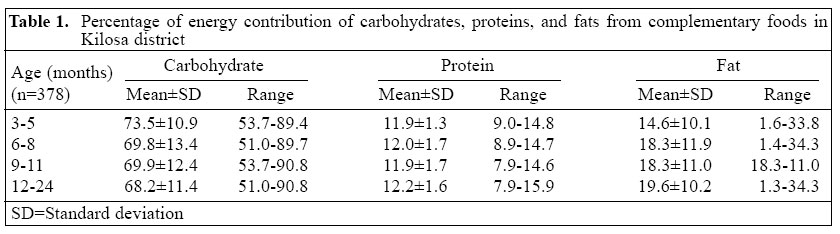
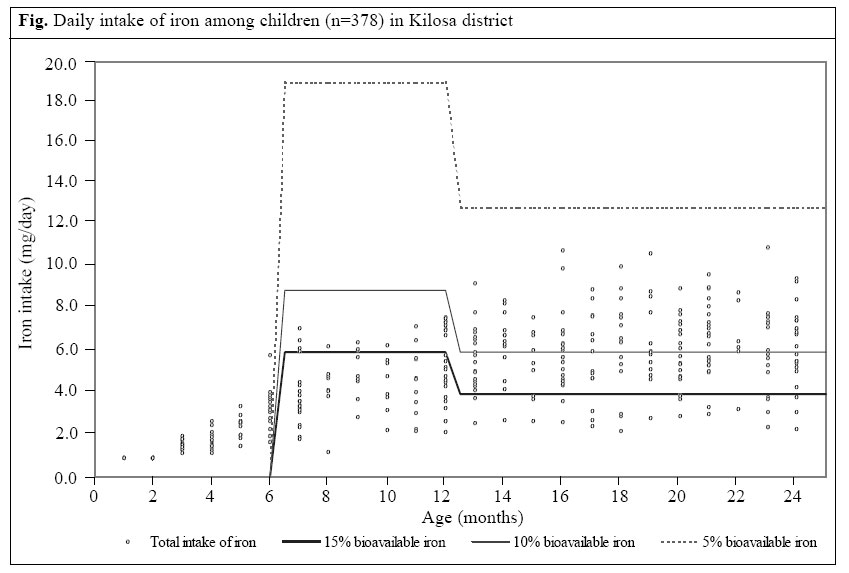
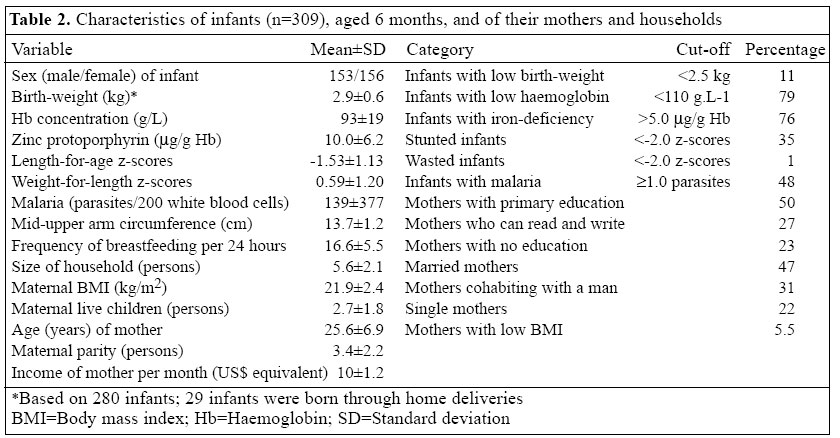
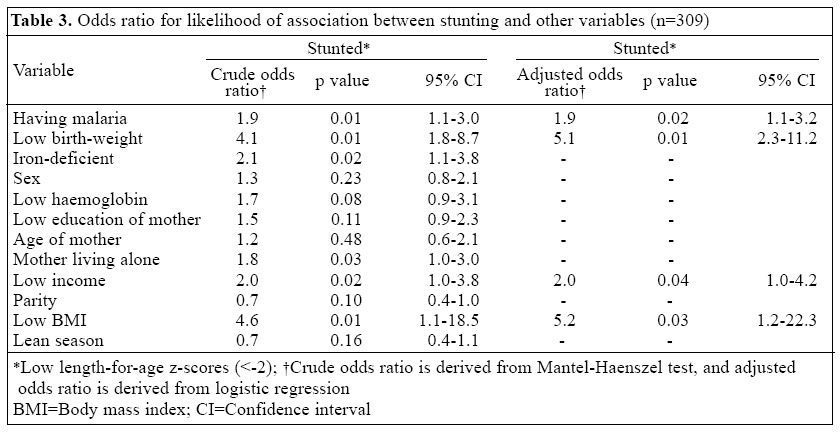
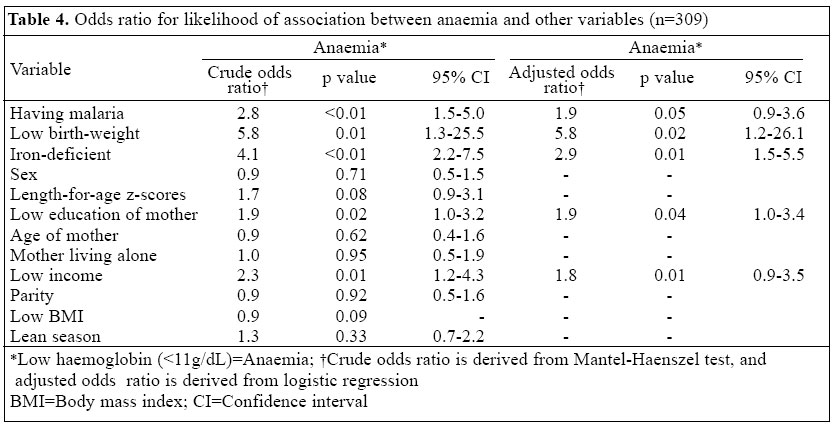
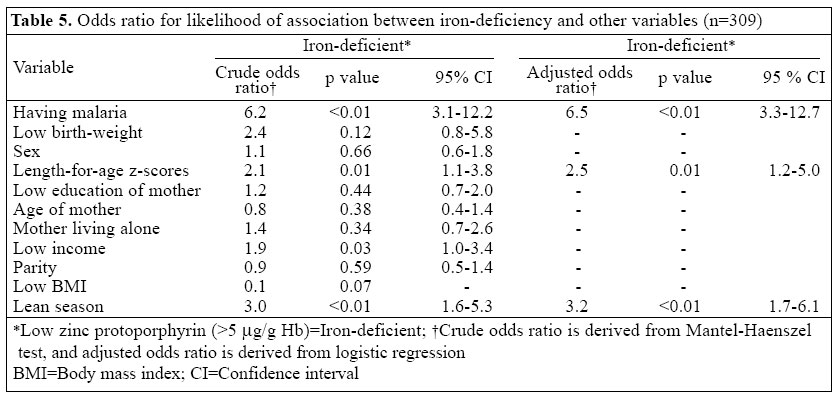
PO Box 3006, Morogoro, Tanzania Code Number: hn05028 ABSTRACT Infants in Tanzania are particularly vulnerable to under-nutrition during transition from breastmilk (as the only source of nourishment) to solid foods. A cross-sectional study was undertaken in Kilosa district in Tanzania to determine the feeding practices and the extent of wasting, stunting, and iron-deficiency anaemia. The study was done in two stages: in the first stage, a 24-hour dietary assessment was conducted to identify the type of complementary foods given and the eating habits according to age for 378 children aged 3-23 months. In the second stage, a progressive recruitment of 309 infants aged six months was made to measure weight, length, haemoglobin (Hb) concentration, zinc protoporphyrin concentration, and malaria parasitaemia. Birth-weight, the potential contributing factor to under-nutrition and iron-deficiency anaemia, was obtained from the children's clinic cards. The 24-hour dietary assessment revealed that children consumed mainly a thin porridge prepared from maize flour as complementary food. Carbohydrates contributed most energy (on average 69%), followed by fats (18.6%) and protein (on average 12.1%). The complementary food covered only 15%, 20%, and 27% of the recommended iron intake for children aged 6-8, 9-11 and 12-23 months respectively. The mean Hb concentration was 9.3±1.9 g/dL, 68% of the infants were moderately anaemic(7-<11 g/dL), and about 11% were severely anaemic with Hb below 7 g/dL, while 21% were non-anaemic Hb ( ≥11 g/dL). Equally, the mean zinc protoporphyrin concentration was 10.0±6.2 μg/g Hb, and 76% of the infants were iron-deficient(>5 μg/g Hb). The prevalence of stunting was 35%, while wasting was only 1.3%. Low birth-weight and low body mass index of mothers were the strong predictors of stunting, whereas low birth-weight and iron-deficiency were the strong predictors of anaemia. The prevalence of malaria parasitaemia was high, affecting 50% of the infants. Having malaria was the only independent predictor associated with stunting, anaemia, and iron-deficiency. There is an urgent need to improve traditional complementary foods in the studied community in terms of energy density, amount of fat in the diet, and bioavailability of macro and micronutrients. Key words: Infant-feeding practices; Anaemia, Iron-deficiency; Birth-weight; Infant nutritional status; Child nutritional status; Cross-sectional studies; Tanzania Introduction Malnutrition and infectious diseases are the most wide-spread problems, affecting young children in developing countries. Tanzania is no exception (1). Breastmilk may be a sole and sufficient source of nutrition during the first six months of life (2) but towards the middle of the first year, even breastmilk provided by the best-nourished mother is insufficient to support the growing infant (3). Rapid growth of infants during the first year of life and specifically the first six months postpartum requires an adequate supply of nutrients to cope with the rapid build-up of body muscles and other tissues (4). This critical transition period is associated with a dramatic in-crease in malnutrition among infants. The present study follows a previous pilot study conducted in Kilosa district in Tanzania to determine the magnitude of nutritional deficiencies among 338 infants aged 4-11 months (unpublished data). The z-scores of weight-for-age, weight-for-length, and length-for-age indicated that 21% of the infants were under-weight, 2.1% were wasted, and 37.6% were stunted. The mean birth-weight was 3,000±530 g with 18.0% low birth-weight (weight below 2,500 g). The mean haemoglobin (Hb) concentration was 80.4±17.3 g/L, whereby the majority (76.4%) of the infants had a Hb concentration between 70 and <110 g/L. More than 20% of the infants were se-verely anaemic (Hb concentration <70.0 g/L). Hb dropped significantly between four and seven months stabilizing beyond seven months. Infants aged 4-6 months had the highest Hb concentration (mean 96.4 g/L), while infants aged 7-9 months had the lowest Hb concentration (mean 78.0 g/L), rising a little to mean Hb concentration of 80.2 g/L in infants aged 10-12 months. The significant fall of Hb between the 4th and 7th month coincides with the introduction of complementary foods at around 4-5 months of age. The objective of the study was, therefore, two-fold: first, to investigate the feeding practices with regard to complementary foods at the age of 3-23 months and, second, to investigate the nutritional status of infants at the age of six months, with particular reference to iron-deficiency anaemia and its determinants. Materials and Methods Study area The study was conducted in Kilosa rural district in Morogoro region in Tanzania, located 300 km west of Dares-Salaam. The survey was conducted in four villages, namely Ilonga, Mvumi, Msowero, and Mambegwa, located approximately 10 km from each other. Kilosa was chosen for the study because it is among the districts in Morogoro region, which has a high prevalence of infant malnutrition and iron-deficiency anaemia (5). Study protocol and subjects The study was performed in two parts. The first part comprised a cross-sectional assessment of complementary feeding patterns among children aged 3-23 months and was conducted during August-October 2000. From the list of children, registered at the child healthcare (MCH) clinic, 400 children aged 3-23 months were randomly selected, which gave us 378 participants after refusals. Since there is a specific child health programme, all children are registered from birth. Each child is allocated a number, and using a random number table, children were selected. The total number of children was estimated on the assumption that the average intake was around 830 kcal for the 9-11-year age group with an estimated standard deviation of 100-200 kcal. With this number, we would have a precision of between 20 and 40 kcal for 350 participants. The second study enrolled children when they were aged six months. Continuous enrollment was necessary to have a large sample of a homogeneous population in terms of age. On this group of children, Hb, erythrocyte protoporphyrin, presence of malaria, birth-weight, and body mass index (BMI) of mother and socioeconomic determinants were studied. In total, 309 infants were en-rolled from March 2001 to March 2002. Dietary assessment For dietary assessment, home-visits were made, and a 24-hour quantitative dietary recall was used. For some mothers, who were not at home at the time of the first visit, a new appointment was fixed, leaving a message to request the mother to be at home. This is because mothers in Tanzania, especially in rural areas, prepare and give complementary foods to their children. During the dietary recall interviews, the mother was requested to show the type and amounts of foods, which the infant had consumed in the last 24 hours. The amount of food consumed by the infant was weighed using a digital weighing scale (Tefal scales UK or measured by a measuring cylinder, Pyrex - UK). No attempts were made to estimate the amount of spilled food. Macro and micro-nutrient contents of food items were calculated using the food-composition tables of the Food and Agriculture Organization (6) and computed with Microsoft Excel 2000 software. Anthropometric indicators Most infants were born in hospitals or maternity centres, where healthcare personnel measured birth-weight soon after birth. Birth-weight of the infant was obtained from his or her clinic card. Recumbent length of infants was measured to the nearest mm using an infant-measuring board (Perspective Enterprises, Portage, MI). Weight of infants was measured to the nearest 100 g, with a Salter scale (Model 235 6S - England) with a capacity of measuring up to 25 kg. Measurement of haemoglobin concentration, zinc protoporphyrin, and malaria parasitaemia Hb concentration was measured on finger-prick blood by the Hemocue B-Haemoglobin System (Hemocue AB Ängelholm, Sweden). Zinc protoporphyrin (ZP) was mea-sured with a portable haematofluorometer (Aviv Bio-medical Inc, Lakewood, NJ). Values of >5 µg ZP/g Hb indicated iron-deficiency erythropoiesis. A finger-prick blood sample was used for preparing blood smears. Malaria parasite counts were made per 200 white blood cells after Giemsa-staining. Ethical considerations Verbal consent to participate in the study was obtained from mothers. Infants found infected with malaria and having other diseases, such as severe anaemia and diarrhoea, were referred to the respective health centres and treated free of charge. The ethics committee of the Tanzania Food and Nutrition Centre and Gent University reviewed the protocol and gave approval for the study. Statistical analysis Data were entered using Epi Info (version 6.04d; Centers for Disease Control and Prevention), and analyses were done with Stata 5.0 package (Stata version 5.0; Stata Corporation, College Station, Texas). Z-scores of weight-for-length and length-for-age were computed using EPINUT according to the National Center for Health Statistics standards, reference of 1978. Logistic regression analysis was performed with three main outcomes (dependent variables), i.e. anaemia (Hb <110.0 g/L), iron-deficiency (zinc protoporphyrin >5 µg ZP/g Hb), and stunting, i.e. length-for-age <-2 stan-dard deviation of the population reference median (7). Wasting was not considered in the analysis because it was virtually non-existent in our sample. We were interested in determining the biological or environmental factors associated with the outcomes. The considered factors (independent variables) were the following: Child's parameters: zinc protoporphyrin >5 µg ZP/g Hb (0=no, 1=yes), Hb <110.0 g/L (0=no, 1=yes), blood smear positive for malaria (0=no, 1=yes), birth-weight <2,500 g (0=no, 1=yes), length-for-age <-2 z-score (0=no, 1=yes), sex (0=girl, 1=boy), and season at entry in the study (0= harvest season, 1=other season). Mother's parameters: education of mother lower than primary school (0=no, 1=yes), mother living alone (0=no, 1=yes), age of mother <20 years (0=no, 1=yes), parity ≥ 3 (0=no, 1=yes), BMI (0=between 18.5 and over 25, 1=under 18.5), and income lower than 10,000 shillings (0=no, 1=yes). The strategy of data analysis was set in two steps. First, the association was studied between each of the main outcomes and the potential determinants analyzed by the Mantel-Haenszel test; and second, a multivariable analysis was performed by applying logistic regression. Three sets of models were defined - one for each of the main dependent outcome variables coded 0/1. For all sets, the variablessignificantly(p<0.05) associated with the dependent variable in univariate analysis were included in the regression model. To determine which variable was to be kept in the final model, a stepwise back-ward procedure was used. Removal of variables was at a level of significance of >5% for the likelihood ratio test. The presence of multicolinearity and other numerical problems in regression analysis was appraised by verifying the presence of a high-estimated standard error (8). Results Twenty-four-hour dietary recall Food-consumption data from the 24-hour dietary recall in the area showed that the complementary foods alone covered 21%, 55%, 61%, and 60% of the total daily energy requirements for children aged 3-5, 6-8, 9-11 and 12-23 months respectively. Comparing these values with what the minimal contribution of complementary foods should be in terms of energy showed that, in the 3-5-, 6-8-, 9-11- and 12-23-month age-group, complementary foods only covered 48%, 81%, 75%, and 66% respectively of what is recommended by the World Health Organization (9), assuming low intake of milk to use a conservative approach. Carbohydrates were the main energy contributors (on average 69%) (confidence interval [CI] 68.0-70.5) and protein contributed, on aver-age, 12% (CI 11.9-12.3) to total energy intake and fats 18.6% (CI 17.5-19.7) (Table 1). The composition of complementary foods was continuously changing over time, depending on the age of children. Very thin maize porridge was prepared for children aged 3-5 months with increasing viscosity of maize or composite flour porridge prepared for children aged 6-11 months. Older children received a much thicker maize or composite flour porridge and family foods. Results of analysis of food intake showed that most complementary foods were cereal-based porridges with a global average iron content of 4.5 mg per day. Not a single infant's total iron intake could cover the iron needs with a 5% bioavailability level taking into consideration that most complementary foods were cereal-based and high in phytates (Fig.). The main foods given to these children included plain maize porridge, finger millet, rice and peanut composite flour porridge, beans and sardines. However, very few families fed their children beans and sardines. Even with a 15% bioavailability, equivalent to a diversified diet with milk and meat products, the majority of the children would not be able to cover their daily needs from complementary foods as per the recommendations of WHO (9). The complementary food covered only 15%, 20%, and 27% of the recommended iron intake for children aged 6-8, 9-11 and 12-23 months respectively. Six-month old children Average birth-weight was 2,900 g, and the prevalence of low birth-weight was 11%. Characteristics of infants showed a high degree of malaria and anaemia at six months with a low prevalence of wasting in mothers and children (Table 2). The mean Hb concentration was 9.3±1.9 g/dL, 68% of the infants were moderately anaemic(7-<11 g/dL), and about 11% were severely anaemic with Hb below 7 g/dL, while 21% were non-anaemic Hb (≥ 11 g/dL). Equally, the mean zinc protoporphyrin concentration was 10.0±6.2 μg/g Hb, and 76% of the infants were iron-deficient(>5 μg/g Hb). The prevalence of stunting was 35%, while wasting was only 1.3%. Stunting and associated factors Among the factors significantly associated with stun-ting in crude analysis, only malaria, low birth-weight, low income, and low BMI of the mother significantly contributed to stunting in the final logistic model (Table 3). Low birth-weight (adjusted odds ratio 5.1, 95% CI 2.3-11.2) and low BMI of the mother (adjusted odds ratio 5.2, 95% CI 1.2-22.3) were the two strongest in-dependent predictors of stunting in our sample. Five factors were significantly associated with anaemia in crude analysis, i.e. having malaria, being born with a low birth-weight, being iron-deficient, having a mother with low education, and being from a low-income family (Table 4). All the five factors were kept in the final logistic model. The two strongest independent predictors of anaemia in our study sample were low birth-weight (adjusted odds ratio 5.8, 95% CI 1.2-26.1) and iron-deficiency (adjusted odds ratio 2.9, 95% CI 1.5-5.5). Equally, four factors were significantly associated with iron-deficiency in crude analysis, i.e. having malaria, being stunted, being from a low-income family, and being in a lean season. Only malaria, stunting, and lean season could be kept in the final logistic model. Malaria (adjusted odds ratio 6.5, 95% CI 3.3-12.7), stunting (adjusted odds ratio 2.5, 95% CI 1.2-5.0), and lean sea-son (adjusted odds ratio 3.2, 95% CI 1.7-6.1) were the three strongest predictors of iron-deficiency in our study sample (Table 5). It was observed that the odds for developing anaemia and iron-deficiency were two and six times higher when having malaria parasitaemia than infants with normal Hb and iron status respectively (Tables 4 and 5). In this study, the prevalence of malaria was 48% with the same distribution in both the sexes. The average number of parasites per infant was 139±377 per 200 white blood cells ranging from 0 parasite to 2,760 parasites per 200 white blood cells. Discussion The total energy intake from complementary foods with-out breastmilk was covering about 69% of the total daily energy requirements for children aged 3-23 months. This shows that the contribution of complementary foods alone did not cover daily requirements from complementary foods adequately. The high contribution of carbohydrates in the complementary foods of children as depicted in Table 1 was a characteristic of complementary food given to children in most of Tanzania (10). This is mainly the result of complementing breastmilk with gruels made up of locally-produced staple foods, such as maize, cassava, sorghum, finger millet, and sweet potato (11). These starch-based complementary foods are characterized by a high water content and low energy and nutrient density. To achieve an intake that is sufficient to meet energy and nutrient requirements, a child is supposed to ingest relatively large volumes of such foods (9). The dietary bulk characteristics of complementary food could be among important factors contributing to the aetiology of protein-energy malnutrition in children. Supply of dietary fat from complementary foods remained low, covering 18.6% of energy requirements, on average, with a slight increase from 14.6% and 19.6% from four months to 23 months. Peanuts in the habitual complementary food-mix contributed most to fat intake from complementary foods. Similar findings were reported by Prentice and Paul in Gambia where they found that the percentage of total energy from fat was initially >50%, but declined to 30% by 17 months of age (12). Peanuts were the main providers of dietary fat. Current guide-lines suggest that dietary fat should range from 30% to 45% of the total dietary energy for children aged less than two years (13). By removing the amount supplied by breastmilk, complementary foods that were currently consumed by children in the study area did not provide adequate dietary fat. Infants were already iron-deficient at six months of age, as revealed by the zinc protoporphyrin values. This study revealed that the majority of the mothers started to complement their infants with solid foods by three months of age on average. The low dietary iron correlated well with the zinc protoporphyrin values obtained, in which 76% were iron-deficient. According to WHO, meeting micronutrient needs from complementary foods appears to be the greatest challenge (9). It has been re-ported that it is practically impossible to supply enough iron from unmodified complementary foods to meet the calculated needs of infants aged 6-11 months without high intakes of animal products, such as liver, fish, beef, and eggs (14). However, affordability of animal products in rural Tanzania by the majority of households is questionable. One possibility could be to modify currently-consumed grains by germination to reduce the anti-nutritional factors, such as phytates and tannins, that interfere with the bioavailability of micronutrients (15,16). The high prevalence of stunted infants (35%) observed in these rural Tanzanian infants at six months of age suggests that linear growth retardation has an early onset. Indeed, it takes time to cross the -2 z-score limit, and to observe such a high-prevalence stunting must start early. This would be in a period before the effects of complementary feeding on growth can be expressed. Similar observations were made in East Java where the high pre-valence of stunting was related to an onset from birth and could be related to intrauterine growth retardation (17-19). In our study population, stunting at six months was related to low birth-weight. Stunting has frequently been associated with maternal factors and in particular the mother's poor nutritional status before conception, short stature, and poor nutrition during pregnancy (17,20). Inadequate weight gain during pregnancy is particularly important since it accounts for a large proportion of foetal growth retardation. In our results, BMI of mothers was the strongest predictor of stunting in children. Malaria was observed to be a predictor of all three main outcomes in our study, i.e. stunting, anaemia, and iron-deficiency. The study area is a malaria-endemic area where reinfection is very common. According to Menendez, continuous reinfection causes disturbance in physiological growth processes, which end up in growth faltering among infants (21). Our study further observed a positive association of anaemia at six months of age with low birth-weight. Similar results were observed in the Honduran children where-by low birth-weight was strongly related to low Hb, haematocrit, and ferritin values (22). Because of the well-known relationship between birth-weight and iron reserves, it is commonly recommended that infants with birth-weight less than 2,500 g receive iron supplements beginning at 2-3 months of age. It was rather surprising that low birth-weight was not associated with iron-deficiency. Dietary deficiency in iron might be among the major reasons for iron-deficiency at this age period because, for the majority of infants and young children in rural Tanzania, complementary foods are cereal-based, low in iron content and its bioavailability. The condition of iron-deficiency is aggravated when calorie intake is low. This was reflected in our results in that the lean season was a strong independent predictor of iron-deficiency in infants at six months of age. Tanner and Lukmanji reported that, during the post-harvest period, infants were given superior foods, and they became healthier than in the lean season where porridge made of cassava was the main dish (23). In summary, this study has identified several potential factors responsible for malnutrition and iron-deficiency anaemia among infants in rural Tanzanian communities. Poor nutrition and diseases have been seen as the main factors responsible for health deterioration in infants at complementary stage. If nutrition could be improved at this age, there might be beneficial effects on growth and health of infants in the short run. Therefore, there is an urgent need to improve traditional complementary foods in terms of energy density and bioavailability of macro and micronutrients. Acknowledgements The authors wish to acknowledge financial assistance from Nutritional Tiers Monde, Steve Biko and Flemish Interuniversity Council (VLIR) for the study. The authors appreciate all mothers in Ilonga, Mvumi, Msowero, and Mambegwa villages for the patience they showed in responding to the questionnaire and accepting their infants to be tested for various parameters. References
© 2005 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn05028t5.jpg] [hn05028t3.jpg] [hn05028f1.jpg] [hn05028t1.jpg] [hn05028t4.jpg] [hn05028t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}