 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 23, No. 3, Sept, 2005, pp. 236-244 Routine Use of Antimicrobials by Pregnant Indian Women Does not Improve Birth Outcome: A Randomized Controlled Trial Amitava Sen1 , Dilip Mahalanabis1 , Sanjib Mukhopadhyay2 , Kamalendu Chakrabarty2, Arun K. Singh3 , Samiran Bisai1 , Monilal Chakrabarty4 , Debasis Halder2 , and Mohammad Aminul Islam5 1 Society for Applied Studies, 2 M.R. Bangur Hospital, 3 Institute of Postgraduate Medical
Education & Research, 4 Kothari Medical Research Centre, Kolkata, India, and
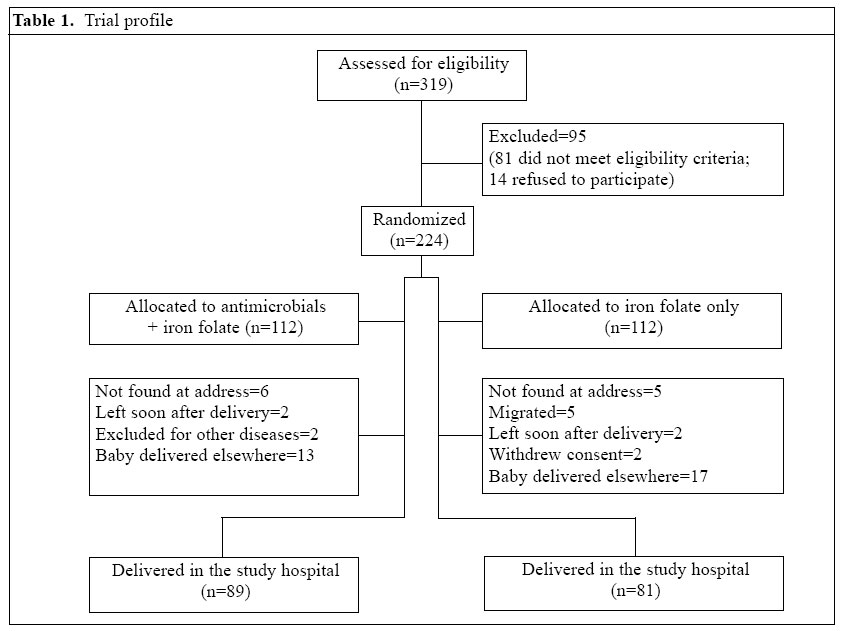
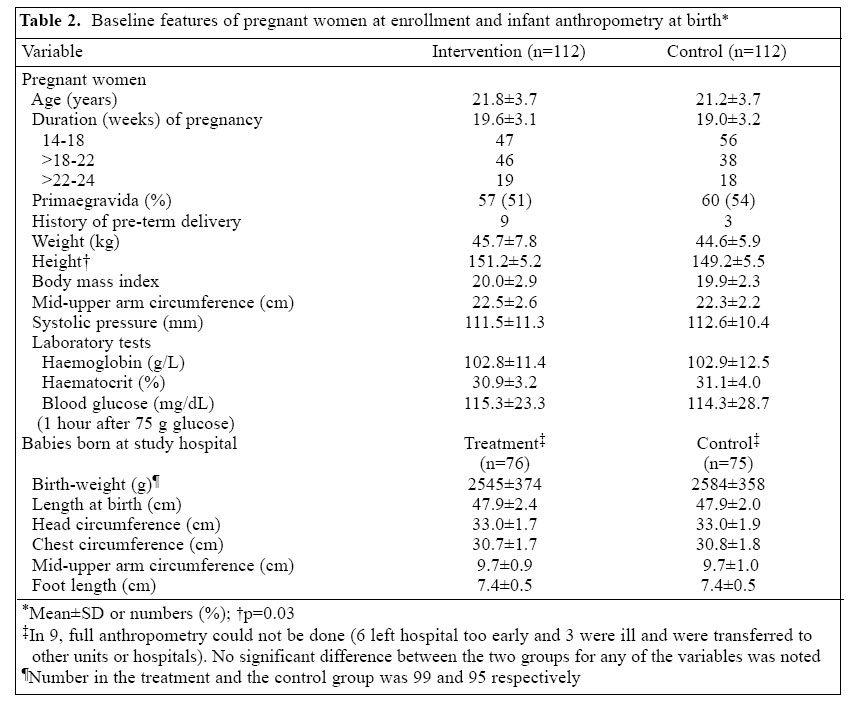
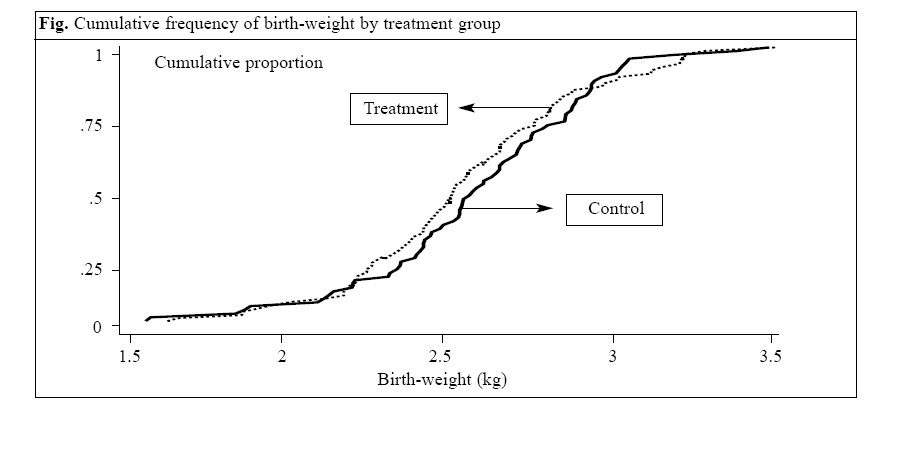
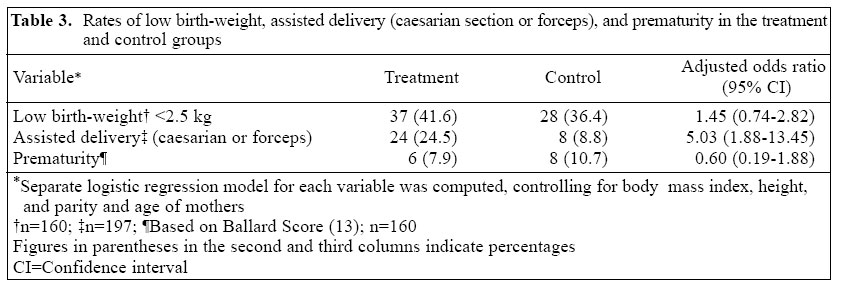
5 University of Alabama at Birmingham, USA Code Number: hn05030 ABSTRACT Low birth-weight is a leading health problem in developing countries. In a randomized controlled trial, the effect of antimicrobials in pregnant women on improving birth-weight and duration of gestation was evaluated. Two hundred twenty-four pregnant women in their second trimester were randomized to receive metronidazole (200 mg 3 times daily for 7 days) and cephalexin (500 mg twice daily for 5 days) orally by one group. The mean (±SD) birth-weights were 2,545 g (±374) and 2,584 g (±358, p= 0.51), the low birth-weight rates(<2.5 kg) were 40% and 36% (p=0.28), and the prematurity rates were 8% and 11% (p=0.6) in the treated group and the control group respectively. Due to small sample size, it is cautiously concluded that routine antimicrobials for genital and urinary tract infections of pregnant women do not improve birth-weight or duration of gestation. Rather an unexpected observation was the proportion requiring caesarian section or forceps, which was five-fold higher in the treated group (p= 0.001), and given no plausible explanations, this finding needs confirmation. Stunted mothers(<25th centile or 146.4 cm) had two-fold higher risk for low birth-weight (p=0.04) and assisted delivery (p= 0.1). Low maternal body mass index(<25th centile or 18) had six-fold higher risk for stillbirth or abortion (p= 0.007), and high body mass index(>75th centile or 21.2) had three-fold higher risk for assisted delivery (p=0.003). Key words: Birth-weight; Drug therapy; Infant, Low birth-weight; Intrauterine growth retardation; Pregnancy trimester, Second; Pregnancy outcome; Reproductive tract infections; Urinary tract infections; Pregnancy outcomes; Randomized controlled trials; India Introduction Seventy percent of the annual 32 million low-birth-weight (weight <2.5 kg at birth) neonates globally are born in developing countries (1). In South Asia (which includes India), an estimated 30% of babies are born with low birth-weight (1). Low birth-weight is often used as a proxy indicator for intrauterine growth retardation in developing countries because a valid assessment of gestational age is often not available. In India, one-third of babies born are of low birth-weight (2). Low birth-weight is associated with increased morbidity and mortality, impaired immune function, and poor cognitive development (3) for neonates, infants, and young children. The risk of neonatal deaths among babies weighing 2-2.5 kg at birth was estimated to be four times the rate in neonates with birth-weight of 2.5-3 kg and 10 times higher than in neonates weighing 3-3.5 kg (3). Of all the neonatal deaths in India, an estimated 81% occur among low birth-weight neonates, and a high proportion occurs among pre-term babies (2). Bacterial vaginosis has been consistently associated with a risk of spontaneous pre-term birth in the West (4-7). In two randomized trials involving women at high risk of pre-term birth, treatment of bacterial vaginosis with metronidazole either alone or in combination with erythromycin resulted in substantial reduction in rates of spontaneous pre-term births (8,9). Furthermore, un-diagnosed and untreated bacteriuria in pregnant women may also increase the risk of low birth-weight and perinatal deaths (10). The prevalence of reproductive tract infections (RTIs) is high among Indian women of reproductive age (11,12), particularly among the lower socio-economic groups. In developing countries, large maternity hospitals serving the urban poor work beyond capacity and under extreme resource constraints. Given these factors and reported benefit (8,9), the health practitioners in India commonly give antimicrobials to pregnant women to treat putative bacterial vaginosis for improving pregnancy outcome, particularly birth-weight. However, such an approach to treatment has not been evaluated. We hypothesize that treating poor urban pregnant women with antimicrobials for putative RTIs and UTIs routinely will reduce the rate of low birth-weight by prolonging the duration of pregnancy and by improving intrauterine nutrition of the foetus. In a randomized controlled trial, we evaluated the role of routine antimicrobial therapy during the second trimester of pregnancy on birth-weight and gestation in urban poor pregnant women in the metropolitan city of Kolkata, India. The rate of low birth-weight is known to be high in this patient population. Materials and Methods Study population and intervention The study was conducted among pregnant women in their second trimester as ascertained by the history of last menstrual period (between 14 and 24 weeks), not suffering from any significant medical, surgical, obstetric or gynaecological disorders and attending the antenatal clinic of a government hospital in Kolkata, India, that serves the urban poor. Women likely to deliver at this hospital were enrolled in the study after obtaining in-formed written consents from the pregnant women. Recruitment took place during February-July 2001. The subjects who stayed at a distance where home-visits, if necessary, would be difficult were excluded. Detailed history, anthropometric measurements, and clinical examinations of the subjects were recorded in a pre-tested data form, and the following investigations were done at recruitment. Urine was tested by the dipstick method for protein, nitrites, and leucocytes, which are indicators of infection. The test results were not used for inclusion of subjects in the study. Blood was tested for haemoglobin and haematocrit, Venereal Disease Research Laboratory test for syphilis, C-reactive protein, blood group, and one-hour post-prandial blood glucose after taking 75 g of glucose. The subjects were randomized into intervention group and control group. Women in the intervention group were treated with a course of antimicrobials and were provided with iron-folic acid tablets, and the control-group women received iron-folic acid tablets only. A combination of metronidazole and cephalexin was chosen for antimicrobial therapy, as this combination was likely to be effective against both RTIs and UTIs and safe for use during the second trimester of pregnancy. Metronidazole and erythromycin have been used in earlier studies. Metronidazole is known to be effective against Gram-negative bacteria and Trichomonas vaginalis . Cephalexin and cephalesporin are effective against both Gram-positive and Gram-negative organisms and have a marginally-better safety profile for use in pregnant women. The subjects in the treatment group received the antimicrobial combination orally in the following dosage and duration: (a) metronidazole 200 mg tablet eight hourly after food for seven days and (b) cephalexin 500 mg capsules 12 hourly for five days. Both the groups received iron-folic acid tablets for 100 days. The subjects were followed up at the clinic first after 7-10 days and then at monthly intervals until delivery. Any observed or reported adverse-effect was recorded. At follow-up visits, they were encouraged to come for delivery in the same hospital. All perinatal events were recorded. Home-visits in situations of failure to turn up for a scheduled follow-up visit were conducted. Evaluation of the newborn Detailed clinical examinations, including assessment of gestation and anthropometry, were performed on neonates born to mothers in the treatment and control groups in the delivery areas (Maternity wards) of the same hospital and were recorded. Birth-weight was measured with a triple beam balance with a precision of 1 g. Length was measured with a rigid measuring board with a moving footboard to 0.1 cm. Circumferences were measured with a non-stretchable tape to 0.1 cm. Foot length was measured with a set square triangle. Ballard score done within 12-24 hours of birth was used for determining the gestational age of neonates born at the study hospital. This score is based on neuromuscular and physical maturity. It is most accurate when performed between 12 and 20 hours of age. Combined score from five neuromuscular maturity signs and five physical maturity signs are used for estimating the gestation in weeks (13). The Ethical Review Board of the Society for Applied Studies approved the protocol. Randomization A person not associated with the study prepared a master randomization schedule using permuted blocks of random numbers using variable block lengths chosen at random. The allocation to treatment or control according to this randomization was sealed in serially-numbered envelopes so that the serial numbers correspond to the subject serial numbers and held by a person not involved in the study. After irrevocably assigning a pregnant woman in the study, the envelope with the serial number of the subject was opened to ascertain treatment allocation. Study design A non-placebo randomized controlled trial design was used for testing the hypothesis that antimicrobial therapy aimed at treating putative RTIs and UTIs during the second trimester of pregnancy will improve birth-weight and gestation. The physician examining the neonates and the trained health worker doing the measurements at birth were kept unaware of the treatment allocation. The outpatients department where the pregnant women were recruited and followed up was housed in a different building, at a distance from the maternity ward, and a separate team of workers was responsible for this part of the programme. Outcome measure The primary outcomes of interest were birth-weight and rates of low birth-weight. Secondary outcome measures were adverse events likely to be associated with the use of antimicrobials, such as nausea, vomiting, and allergic response. Sample size It may be noted that such an intervention has not been reported for the unique problem of low birth-weight in South Asia, and the anticipated improvement can only be surmised. Calculation of sample size was based on the expected change in birth-weight. To detect an increase in mean birth-weight by 150 g (taking mean birth-weight= 2.6 kg and standard deviation [SD]=350 g, based on our unpublished data in this population) at 95% confidence and 80% power, the required number in each group is 86. We aimed at recruiting 95 pregnant women in each group to detect an increase in mean birth-weight by 150 g that includes 10% deviated course (a total of 190 pregnant women). No interim analysis was planned. The sample size was calculated to detect a relatively large difference in birth-weight, and a smaller increase in birth-weight would still be of public-health interest. Data analysis Data were recorded in pre-tested standard forms, entered into a desktop computer and edited using Epi Info version 6.03 software (CDC, Atlanta and WHO, Geneva). Data were analyzed using Epi Info and Stata version 7.0 (Stata Corporation, Texas, USA). Quantitative variables were compared using t-test, and proportions were compared using the chi-square test or Fisher's Exact test. Rate ratios and 95% confidence intervals (CIs) were calculated for appropriate variables. Adjusted analysis was done using multiple linear regression and logistic regression models. Results Of 319 pregnant women assessed for eligibility, 224 were randomized into the study and control groups (Table 1). Eighty-one women did not meet the eligibility criteria, and 14 refused to participate. The baseline characteristics of the pregnant women in the two groups were similar (Table 2), except mean height which was significantly higher in the treatment group (p=0.025). More than 50% of the women were primaegravida. At enrollment, the period of gestation was similar in the two groups, and over 80% had gestation between 14 and 22 weeks (Table 2). The body mass index estimated at the time of admission, i.e. 14-24 weeks of gestation, was low, and 69% of the subjects had body mass index less than 18.5. Urine was positive for nitrite in two each, for leucocytes in seven and six women, and for protein in one and three women in the treatment group and the control group respectively. However, urine culture and/or vaginal swab culture were not done in this study. Thirteen mothers in the treatment group and 17 in the control group delivered either at home or in other health facilities (Table 1). For these 30 women, information on deliveries was sought during home visits. We compared the baseline features of these mothers, which were similar in the two groups. Compliance with antimicrobials in the study group was ascertained by in-depth interview after 7-10 days of starting therapy, and none reported stopping medicine or skipping doses. The antimicrobials were well-tolerated, and no untoward effects, such as nausea, vomiting, allergic reactions, were reported. One mother in the control group discontinued iron folate tab-lets for nausea and vomiting. Accurate weighing and anthropometric measurements at birth were taken on the babies born at the study hospital (Table 2). Birth-weight, length, head, chest and midarm circumferences, and foot length were similar in the two groups. The cumulative frequency of birth-weight by treatment group is compared in the Figure, and no significant difference was observed between the two groups. Rates of low birth-weight, assisted delivery (i.e. caesarian section or forceps), and prematuredelivery(<37 weeks of gestation) were compared after adjusting for age of mothers, body mass index, height, and parity (Table 3). Type of delivery (Table 3) could be ascertained in 189 cases, and the proportion requiring caesarian section or forceps delivery was five times higher in the treatment group (adjusted odds ratio [OR]=5.03; 95% CI, 1.88-13.45, p=0.001). Furthermore, proportion having elective caesarian section due to previous history of caesarian section or due to post-dated primipara was similar in the two groups (i.e. 5 in each group). Thirteen mothers in the treatment group had caesarian section for indications, like prolonged or non-progress of labour, foetal distress, ruptured membrane, diminished foetal movement, obstructed labour, and transverse lie, and only one mother in the control group had caesarian section due to such an indication, i.e. foetal distress (RR=12.6, CI 1.7-93.8, p=0.001). In several subjects, gestation age based on last menstrual period appeared implausible. We, therefore, used Ballard score for comparing gestation period, and this was feasible for babies born at the study hospital (n= 171). Based on Ballard score, proportion of neonates with pretermdelivery(<37 weeks gestation) was 40% lower (Table 3) in the treated group (adjusted OR=0.60, CI 0.19-1.88, p=0.38) but the difference was not significant. There were 17 (20%) small-for-gestation age neonates in the treatment group and 13 (17.3%) in the control group, and this difference was not also significant. The low birth-weight rate was 45% higher in the treated group compared to the control group after adjusting for confounders (Table 3), but this difference was not significant (adjusted OR=1.45, 95% CI 0.74-2.82, p=0.28). Four neonates in the treatment group had recognizable defects at birth (3 talepes equinovarus and one cleft lip with cleft palate) compared to none in the control group, and this difference was not again significant (p=0.12, Fisher's Exact test, two-tailed). We also carried out analysis to explore independent risk factors for low birth-weight, assisted delivery (i.e. caesarian or forceps), and stillbirth or abortion after adjusting for treatment effect and confounding variables. Stunted mothers (<25 percentile, i.e. <146.4 cm; adjusted for antimicrobial treatment, maternal age, parity, and body mass index) were an independent risk factor for low birth-weight (adjusted OR=2.21, 95% CI 1.05-4.67, p=0.04) and for assisted delivery (adjusted OR=2.18, 95% CI 0.84-5.68, p= 0.1). The latter, however, did not achieve conventional level of statistical significance. Low maternal body mass index (<25th percentile, i.e. <18) was an independent risk factor for stillbirth or abortion (adjusted OR=6.58, 95% CI 1.66-26.13, p= 0.007). High body mass index (>75th percentile, i.e. >21.2) was associated with an increased rate of assisted delivery (adjusted OR=3.60, 95% CI 1.54-8.42, p=0.003). Discussion In South Asia, the magnitude of the problem of low birth-weight is massive, and in India alone, an estimated seven million babies are born annually with low birth-weight (1). As stated earlier, low birth-weight is associated with increased mortality and morbidity, impaired immune function, and poor cognitive development (3). Furthermore, recent studies have shown that low birth-weight is associated with long-term adverse health con-sequences, the so-called foetal origin of adult disease hypothesis proposed by David J.P. Barker and colleagues (14). In an overview of 126 randomized controlled trials, Gulmezoglu and colleagues evaluated 36 prenatal interventions to prevent or treat impaired foetal growth and found that most prenatal interventions did not show any significant benefit on pregnancy outcomes (15). Some likely benefit was only shown for cessation of smoking and protein-energy supplementation during pregnancy. A systematic review concluded that the evidence was insufficient to infer that supplementation of iron during pregnancy increased birth-weight (16); this was largely because available studies suffered from design problems. In a recent large community-based study in Nepal, supplementation of antenatal folic acid-iron moderately reduced the risk of low birth-weight (17). In a study among low-income pregnant women in the USA, supplementation of prenatal iron was associated with a mean in-crease of birth-weight by 206 g (18). Results of intervention trials with multiple micronutrients for improving birth outcome were either equivocal or non-contributory (17,19-21). In this population, a small improvement in the rate of low birth-weight should have a large impact in absolute terms on morbidity and mortality in infants and children. In the present study, treatment of pregnant women from a population known to have a high rate of low birth-weight with a course of metronidazole and cephalexin during the second trimester of pregnancy (14-24 weeks of gestation) did not show a marked beneficial effect on birth-weight and rate of low birth-weight. One unexpected finding was that significantly more mothers who received such treatment had problems at delivery and had to undergo operative and/or assisted delivery com-pared to mothers who did not receive such treatment. The strength of the association (OR >5, p=0.001) sug-gests that the effect may be real. We, however, need to consider whether any prior knowledge of the treatment would have influenced the obstetricians in their decision to do caesarian or apply forceps. We think that it is unlikely given that the mothers received the course of antimicrobials nearly five months back and was administered by a different team at the antenatal clinic. Furthermore, the rate of elective caesarian section was nearly the same in the two groups. It was only the emergency obstetric interventions which were substantially higher in the treated group (OR >12, p=0.001). We, how-ever, take a guarded view of these unexpected findings and think that it needs to be confirmed in a randomized double-masked placebo-controlled trial. The findings caution against the routine use of antimicrobials for putative RTIs and UTIs in pregnant women. A trend was noted for more neonates in the treatment group to have recognizable birth defect at first examination compared to the control group, which did not achieve statistical significance (p=0.12). The sample size was too small for any meaningful interpretation of the apparent increased incidence of congenital malformation in the treated group and can only be confirmed in a trial of adequate sample size. The subjects of this study were asymptomatic pregnant women from among a population with a very high rate of low birth-weight. Earlier reports in developed countries showed benefit of treating pregnant women with metronidazole with or without erythromycin in preventing pre-term delivery (8,9). We, therefore, hypothesized that such a treatment approach may beneficially influence the low birth-weight rate, an important health problem in developing countries, particularly in South Asia. Soon after we completed recruitment of subjects for this study, a report by Klebanoff and colleagues showed that metronidazole not only failed to prevent pre-term delivery, such treatment actually increased its rate among pregnant women with asymptomatic infection due to Trichomonas vaginalis (22). The risk of pre-term delivery, how-ever, did not increase in other trials of metronidazole for treatment of bacterial vaginosis during pregnancy (23). In the absence of elaborate microbiologic data, we can only speculate on the reason for an apparent adverse effect of treating pregnant women with metronidazole and cephalexin. It is possible that such treatment may have suppressed competing flora and allowed some pathogens to flourish. In developed countries, trials for treatment of bacterial vaginosis were usually conducted in women with a history of prior spontaneous preterm delivery. The subjects of the present study were pregnant women from a population known to have a very high rate of low birth-weight. However, the vast majority of these low-birth-weight babies are small-for-gestation due to inadequate intrauterine growth. Some findings from the exploratory analysis are relevant. As expected, height of mother was correlated with birth-weight. One centimetre increase in height of mother was associated with 9% reduced rate of low birth-weight (p=0.005). Furthermore, height of mother also tended to correlate with a reduced need for assisted delivery, i.e. caesarian or forceps. Each centimetre in-crease in height of mother was associated with 8% re-duced rate of assisted delivery (p= 0.074). On the other hand, stunted mothers (height <25th centile or 146.4 cm) had two-fold higher risk of having a low-birth-weight baby. Better body mass index correlated with an increased rate of assisted delivery; body mass index >75thcentile(>21.2) was associated with a three-fold increase in the rate of assisted delivery. Higher height-adjusted weight (i.e. body mass index) may, therefore, be a risk factor for adverse pregnancy outcome. We can only speculate on the reason for it. The 75th percentile of body mass index in this population was only 21.2. However, these mothers come from a population (being from South Asia) where type II diabetes is hyper-endemic. It is plausible that some mothers with better weight were pre-diabetic which may partly explain the adverse pregnancy outcome. The study was randomized but not masked. However, the health workers who assessed mothers and infants at birth were kept unaware of treatment allocation. It is feasible for them to ascertain from the mothers about the treatment they received nearly five months back. However, all the measurements on the babies and the mother are objective in nature. Events, such as caesarian or forceps delivery, are not liable to subjective interpretation. Furthermore, the number of elective caesarian operations that are subject to judgment by the obstetricians was very similar in the two groups. A large difference was found only for emergency obstetric interventions. One limitation of the study is that we have not done laboratory tests to ascertain RTIs. Non-compliance of the pregnant women to deliver at the study hospital also prevented full evaluation of some infants at birth. We compared the baseline features of the mothers of those babies who could not be measured at the hospital between the two groups, and they were similar. Furthermore, the baseline features of those who delivered elsewhere were also similar in the two groups. We have, however, analyzed data on the basis of intention to treat, and all information available for a given variable was used in the analysis. We conclude that, for a population with a high rate of low birth-weight, a marked improvement in birth-weight could not be demonstrated following routine use of antimicrobial therapy to treat putative genital and urinary tract infections of pregnant women during the second trimester of pregnancy. The study does not preclude the plausibility of a more modest weight gain following such intervention. The duration of gestation also did not improve but the sample size was inadequate for a meaningful conclusion. Secondary analysis revealed some expected and relevant information which confirms a large body of evidence in literature. The stunted mothers had a higher risk of low birth-weight. The wasted mothers, as indicated by low body mass index, were at a higher risk of stillbirth or abortion. The mothers with higher body mass index from this population had a higher risk of assisted delivery. Acknowledgements The study was supported by the Society for Applied Studies Trust. The authors thank the staff members of the Antenatal Clinic and the Maternity Ward for their support and assistance, Mr. Jakir Hossain for assisting in computer data management and analysis, and Mr. Subodh Karmakar for typing and editing the manuscript. References
© 2005 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn05030t3.jpg] [hn05030f1.jpg] [hn05030t1.jpg] [hn05030t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}