 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
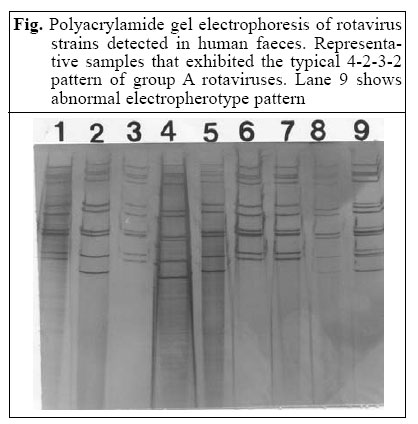
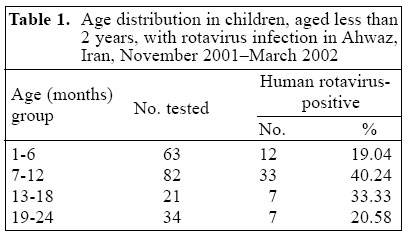
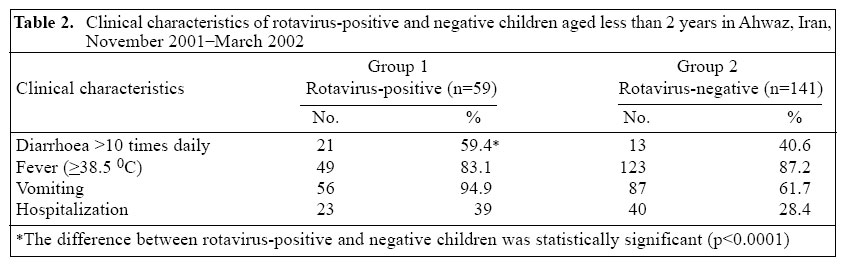
Journal of Health, Population and Nutrition, Vol. 23, No. 3, Sept, 2005, pp. 245-249 Epidemiological Aspects of Rotavirus Infection in Ahwaz, Iran Alireza Samarbafzadeh1 , Elham Mazaheri Tehrani2 , Manouchehr Makvandi1 , and Mahnaz Taremi3 1 Department of Virology, Ahwaz University of Medical Sciences, Ahwaz, Iran, 2 Department of Virology, Pasteur Institute of Iran, 69 Pasteur Ave. 13164, Tehran, Iran, and 3 National Research Department of Foodborne Diseases, Research Center for Gastroenterology and Liver Diseases, Shaheed Beheshti University of Medical Sciences, Evin, Tehran Correspondence and reprint requests should be addressed to: Dr. Mahnaz Taremi, National Research Department of Foodborne Diseases, Research Center for Gastroenterology and Liver Diseases , Shaheed Beheshti University of Medical Sciences, Taleghani Hospital, Tabnak St., Evin, Tehran, Iran, Email: mmtaremi@yahoo.com and taremi@rcgld.org Fax: +98 21 2402639 Code Number: hn05031 ABSTRACT Rotavirus is the major cause of diarrhoea in children worldwide. In this study, conducted in the city of Ahwaz, Iran, during November 2001 - March 2002, stool samples from 200 inpatient (n=63) and outpatient (n= 137) children aged 1-24 month(s) were analyzed. Polyacrylamide gel electrophoresis was used for isolating rotavirus. Rotavirus was isolated from 36 (26.3%) of the 137 stool samples of outpatients and from 23 (36.5%) of the 63 stool samples of inpatients. The overall frequency of rotavirus in this population was 29.5%. The highest detection of rotavirus was made in children aged 7-12 months, which demonstrated that the relationship between age and rate of rotaviral infection was statistically significant (p<0.05). The predominant electrophoretic pattern detected was the long (L) electrophoretype (46 of 59; 78%), followed by the short (S) electrophoretype (12 of 59; 20.3%). One strain had a mixed pattern. Such analysis throughout Iran would assist in developing sound guidelines for the prevention of rotavirus infections. Key words: Rotavirus; Rotavirus infections; Diarrhoea, Infantile; Polyacrylamide gel electrophoresis; Diagnosis, Laboratory; Epidemiology; Iran Introduction Rotaviruses, members of the Reoviridae family, are the single most important aetiological agents of severe diarrhoea in infants and young children worldwide (1-3). The genome consists of 11 segments of double-stranded RNA (dsRNA), which can be separated by polyacrylamide gel electrophoresis. Using this method of separating the viral RNA in conjugation with the sensitive silver-staining technique, it is possible to analyze the viral genome extracted directly from stool specimens (4). Such electrophoresis allows comparisons between different strains; two major types of strain (short and long electrophoretypes) can be differentiated according to differences in the relative migration patterns of segment 10 and 11 (5). Based on distinctive antigenic and dsRNA electropherotype, rotaviruses are classified into at least seven groups (A-G). Group A rotaviruses are classified into G and P types, respectively, based on the VP7 and VP4 proteins presented on the outer shell of the virus (6). Diarrhoea, one of the most common diseases in children, causes more than five million deaths annually. The greatest morbidity and mortality were seen among children aged less than two years (7,8). Human rotavirus is responsible for a large proportion of these deaths and 20-50% of the episodes of acute diarrhoea (8,9). Because the immune response to the infection reduces the occurrence and severity of subsequent infections, diarrhoea due to rotavirus may be controlled through vaccination (10). Results of earlier studies in Iran showed that rotavirus was a major aetiological agent of acute diarrhoea in infants and young children (11). This study, for the first time, assessed the proportion of rotavirus infection by polyacrylamide gel electrophoresis among children aged less than two years with gastroenteritis admitted to the Abuzar Paediatric Hospital, Ahwaz, in the southern part of Iran. Materials and Methods Study site and sample The research was carried out in the city of Ahwaz with a population of 1.5 million. Stool specimens were collected from 200 children, aged less than two years, from the urban zone, who had acute gastroenteritis and attended the Abuzar hospital in the city of Ahwaz from November 2001 to March 2002. This is the only paediatric university hospital in Ahwaz with an admission rate of approximately 320-350 children with acute diarrhoea each year. According to the severity of illness, 63 of these patients were hospitalized, and 137 were treated as out-patients. Diarrhoea was defined as the passage of three or more loose or watery stools in the preceeding 24 hours. Diarrhoea of over seven-day duration, other gastroenteric diseases, and immunodeficiency were considered exclusion criteria for the study. Basic demographic data and clinical information, such as symptoms and severity of diarrhoea, were extracted either from the files or by asking their parents, and only one stool sample was collected per episode of diarrhoea. The labelled stool samples were transported on ice to the virology department at the Medical University of Ahwaz, where these were stored at -20 °C until processed. RNA extraction The crude faecal samples (0.5 g) were diluted with 150 µL of phosphate-buffered saline before they were treated with 1 µL RNase T1 (Roche) at 56 °C for 15 minutes to lyse the single strand of RNAs. Specimens were centri-fuged at 12,000 g for 10 minutes after being mixed with an equal volume of Trizol (Roche) and chloroform to disrupt the viral particles. The clarified stool suspensions were examined. Viral dsRNA was released using the agarose gel DNA extraction kit (Roche) following the instructions of the manufacturer. Polyacrylamide gel electrophoresis The 12-µL samples were loaded onto 10% polyacryla-mide slab gels (acrylamide-to-bisacrylamide ratio of 30:0.8) which were polymerized with 0.01% (vol/vol) of N,N,N',N'-tetramethylethylenediamine and 0.05% (wt/vol) ammonium persulphate. The discontinuous buffer system contained 0.35% of Tris, 1.44% of glycine, and 0.1% of sodium dodecyl sulphate (SDS). Electrophoresis was performed at room temperature for 8-10 hours at 100 V. Silver staining The gels were stained using a modified method described by Herring et al. (12). The gels were washed with 10% ethanol containing 0.2% of acetic acid for three minutes two times and then soaked in 0.3% silver nitrate solution for 10-15 minutes. The gels were then rinsed briefly in distilled water, and the reduction step was performed with 3.5% sodium carbonate solution containing 0.3% of for-maldehyde. The reaction was stopped with 5% acetic acid. Statistics Statistical analyses were performed using the chi-square test and Fisher's exact test. The level of significance was set at a p value of <0.05. The responsible ethics committee of the Research Center for Gastroenterology and Liver Diseases, Shaheed Beheshti University of Medical Sciences, endorsed the study. Results In total, 200 stool samples - 109 from males and 91 from females - were collected from children aged less than two years for the study. Of these samples tested by poly-acrylamide gel electrophoresis, 59 (29.5%) yielded a typical rotavirus electrophoretic pattern. As expected, all samples that could be analyzed by electrophoresis showed the characteristic 4-2-3-2 pattern of group A rotavirus. The figure shows the electropherotypes detected during the study period. The large majority (78%) of the isolated strains were of the long RNA electrophoretype, and 20.3% of the strains exhibited the short migration pattern. One strain had more than 11 RNA segments, a typical feature of mixed infections. The frequencyof isolation was 23 (36.5%) of the 63 stool samples from hospitalized children and 36 (26.3%) of the 137 stool samples from outpatients. There was a significant difference between age and rotavirus infection(p<0.03). The highest incidence of rotavirus infection was observed in children aged 7-12 months (40.24%). The age distribution of the infected children is shown in Table 1. Rotavirus was detected more frequently in males (31%) than in females (28%), although this wasnotsignificant(p>0.05). Breastfed children (n=128) had an infection rate of 19%, and bottlefed children (n= 72) had an infection rate of 48%; the difference was statistically significant (Fisher'sexacttestp<0.0001). The clinical manifestations in rotavirus-positive (Group 1) and negative (Group 2) children are shown in Table 2. Vomiting (94.9%) and diarrhoea with more than 10 stools per day occurred at higher rates in rotavirus-positive children (p<0.001), for which more children in this group needed hospitalization (39%) compared to their rotavirus-negative counterparts. Discussion Diarrhoeal diseases continue to be a major public-health problem worldwide, especially in developing countries (13). This is the first study in Iran investigating rotavirus isolated from children with gastroenteritis by polyacrylamide gel electrophoresis. The greatest advantages of the polyacrylamide gel electrophoresis and silver-staining method are the lack of ambiguity and the fact that it provides information about viral electropherotype. Since the test detects the viral genome, which has a unique number and pattern of dsRNA segments, the results are unequivocal. During the study period, we identified two prominent rotavirus electrophoretypes - the long and short strains, and only one strain had more than 11 RNA segments, a typical feature of mixed infections. In agreement with the results of other studies, isolates with a long RNA electropherotype occurred more often than strains with a short pattern (14-17). One patient in the present study was simultaneously infected by rotaviruses of two different electropherotypes, which were prevalent at the time. This evidence suggests that opportunity for different electrophoretypes to interact with one another in nature is not insignificant. Analysis of data showed a rotavirus rate of 29.5% (59/200) in our study population. However, the rate of 36.5% (23/63) was higher in hospitalized children than in out-patients. This reinforces the association between more severe cases of gastroenteritis and rotavirus infection, as demonstrated in other studies (11,18,19). As documented by other surveys, most cases of diarrhoea due to rotavirus occur in children aged less than two years (20,21). The highest incidence of rotavirus-associated diarrhoea in this study occurred in children aged 7-12 months. This is similar to the incidence in other developing countries where rotavirus is a significant pathogen among infants aged less than 12 months (22), emphasizing that a rotavirus vaccine should be administered in the first months of life to prevent the most severe cases of gastroenteritis. In our study, there was a statistically significant association between breastfed and bottlefed infants with frequency of rotavirus infection (p<0.0001).This result may indicate that breastfed infants, besides acquiring a passive immunity from mothers, may also acquire resistance to infection with rotavirus as is implied here by the low number of breastfed infants among patients. The protective effect of breastfeeding on gastroenteritis caused by rotaviruses has been variable. Breastfeeding does not provide total protection against infection, and serious episodes of rotavirus infection have been noted in breast-fed infants (23-25). However, in many populations, breast-feeding lessens the severity of diarrhoea and vomiting associated with rotavirus infection in hospitalized children (25-27). In our study, there is no statistically significant difference between rotavirus-positive inpatients and outpatients with type of nutrition (p>0.05). During this study, associated signs and symptoms of vomiting, fever, and frequency of diarrhoea among rotavirus-positive cases were broadly comparable with findings reported in other studies (11,28,29). This report confirms that rotavirus is an important cause of paediatric diarrhoea in the south of Iran. Our results are in agreement with reports worldwide and a previous study from Iran (11,30), which reported that rotavirus was the most important cause of severe diarrhoea in children. Such analysis throughout Iran will assist in developing sound guidelines for the prevention of rotavirus infections. AcknowledgementsThe authors thank Dr. K. Eizadpanah for his technical assistance and Dr. P. Ghaempanah for critical reading of the manuscript. References
© 2005 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn05031t1.jpg] [hn05031t2.jpg] [hn05031f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}