 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 23, No. 3, Sept, 2005, pp. 259-265 Risk Factors for Mortality Due to Shigellosis: A Case-Control Study among Severely-malnourished Children in Bangladesh J.M. van den Broek1 , S.K. Roy2, W.A. Khan2, G. Ara2, B. Chakraborty 2 , S. Islam2, and B. Banu2 1 Academical Medical Centre, University of Amsterdam, The Netherlands, and
2 ICDDR,B: Centre for Health and Population Research, GPO Box 128,
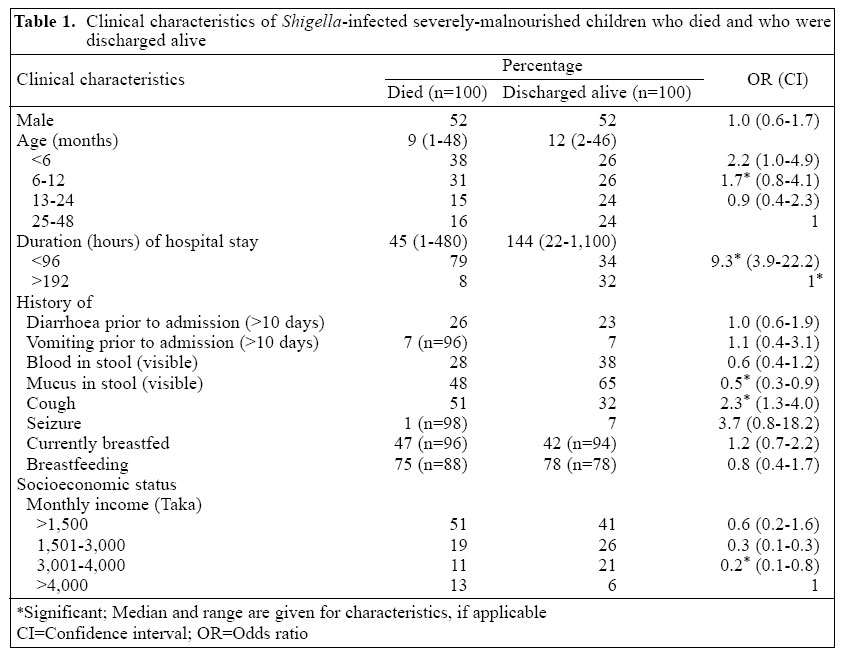
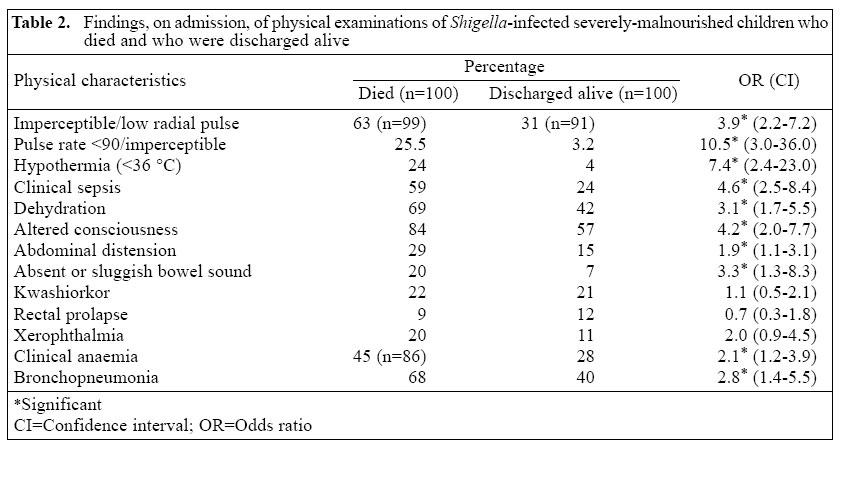
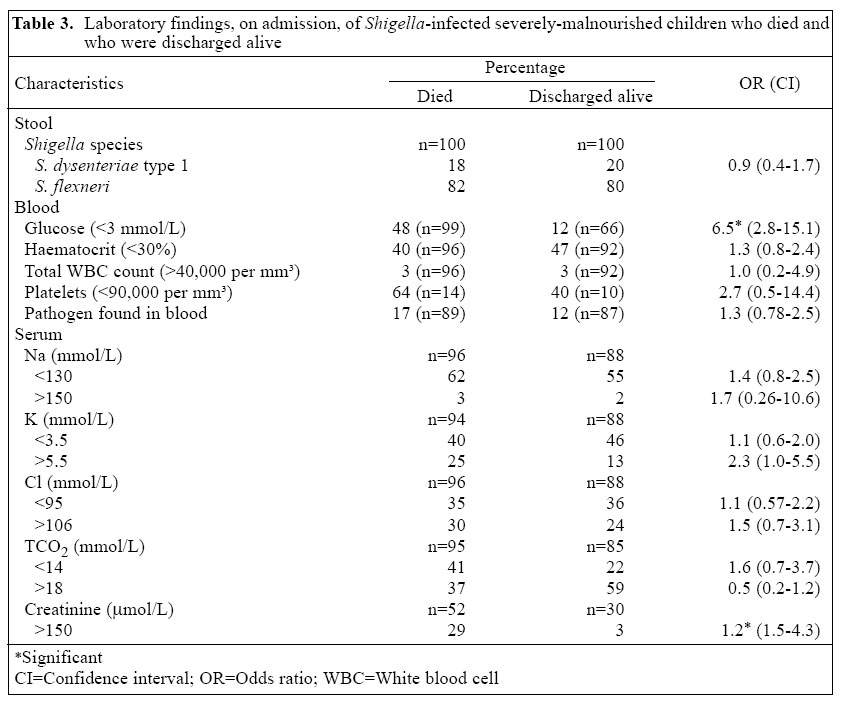
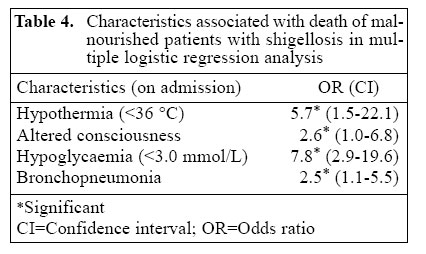
Dhaka 1000, Bangladesh Code Number: hn05033 ABSTRACT To determine the risk factors for death of severely-malnourished Bangladeshi children with shigellosis, a case-control study was conducted at the Clinical Research and Service Centre of ICDDR,B: Centre for Health and Population Research in Dhaka, Bangladesh. One hundred severely-malnourished children (weight-for-age <60% of median of the National Center for Health Statistics), with a positive stool culture for Shigella dysenteriae type 1 or S. flexneri, who died during hospitalization, were compared with another 100 similar children (weight-for-age <60% and with S. dysenteriae type 1 or S. flexneri-associated infection) discharged alive. Children aged less than four years were admitted during December 1993 - January 1999. The median age of the cases who died or recovered was 9 months and 12 months respectively. Bronchopneumonia, abdominal distension, absent or sluggish bowel sound, clinical anaemia, altered consciousness, hypothermia, clinical sepsis, low or imperceptible pulse, dehydration, hypoglycaemia, high creatinine, and hyperkalaemia were all significantly more frequent in cases than in controls. In multivariate regression analysis, altered consciousness (odds ratio [OR]=2.6, 95% confidence interval [CI] 1.0-6.8), hypoglycaemia (blood glucose <3 mmol/L (OR= 7.8, 95% CI 2.9-19.6), hypothermia (temperature <36 °C) (OR = 5.7, 95% CI 1.5-22.1), and bronchopneumonia (OR = 2.5, 95% CI 1.1-5.5) were identified as significant risk factors for mortality. Severely-malnourished children with shigellosis having hypoglycaemia, hypothermia, altered consciousness and/or bronchopneumonia were at high risk of death. Based on the findings, the study recommends that early diagnosis of shigellosis in severely-malnourished children and assertive therapy for proper management to prevent development of hypothermia, hypoglycaemia,bronchopneumonia, or altered consciousness and its immediate treatment are likely to reduce Shigella-related mortality in severely-malnourished children. Key words: Shigella; Dysentery, Bacillary; Infant nutrition disorders; Child nutrition disorders; Infant mortality; Child mortality; Risk factors; Case-control studies; Bangladesh Introduction Shigellosis, prevalent worldwide, is still a major cause of childhood mortality in developing countries. An estimated 667,000 children, aged less than five years, die due to shigellosis each year in developing countries (1). In Bangladesh, Shigella dysenteriae causes epidemic dysentery and is associated with more complications than other Shigella species, and S. flexneri is responsible for endemic infection. Malnutrition is another major public-health problem in developing countries (2), and interaction of malnutrition with shigellosis leads to an even higher mortality (3). Shigellosis causes malnutrition, which is enhanced through reduced food intake (4), in-creased energy expenditure as a consequence of systemic effects of inflammation and fever, malabsorption, and enteric loss of protein (5). Hypothermia, severe malnutrition, severe dehydration, altered consciousness, abdominal distension, thrombocytopaenia, hypoproteinaemia, hyponatraemia, hypoglycaemia, renal failure, and bacteraemia are significantly more common in patients with Shigella-associated infection (6). Complications due to shigellosis, such as mal-nutrition, pneumonia, and septicaemia, predispose children to a higher risk of mortality (7). Frequent resistance to antibiotics (8) and absence of effective vaccines impede the treatment of shigellosis. Although risk factors for the death of children with shigellosis have been described before (6,9), it was not specific for severely-malnourished children. As severe malnutrition is significantly associated with deaths due to dysentery (9), it is necessary to identify the risk factors for mortality of severely-malnourished children to reduce preventable deaths. We hypothesized that severely-malnourished children, who die of shigellosis, present with some particular characteristics compared to those who are discharged alive. Therefore, to determine the factors responsible for in-creased mortality, we undertook a case-control study using the hospital records of 200 patients with lethal S. dysenteriae type 1 or S. flexneri-associated infection admitted to the Clinical Research and Service Centre of ICDDR,B: Centre for Health and Population Research during December 1993 - January 1999. Of these patients, 100 died in the hospital, and the remaining 100 matched patients were discharged alive. Materials and Methods Although all Shigella species are endemic in Bangladesh, S. flexneri and S. dysenteriae are the most commonly-isolated species from culture of stools of patients who attended the treatment centre of ICDDR,B during 1983-1987 (6). These two also cause a more severe form of dysentery with more gastrointestinal and extraintestinal manifestations than S. boydii and S. sonnei (10,11). The hospital records of patients admitted to the Clinical Research and Service Centre of ICDDR,B during December 1993 - January 1999 were reviewed. The Centre treated more than 150,000 diarrhoeal patients in 1998. Approximately, 10,000 of them had a positive culture for Shigella. Death cases were selected from those cases who died due to shigellosis in the hospital. The probability for the controls to have a risk factor was estimated to be 10%. We planned to identify a risk factor with an odds ratio of size 2.5 or more. This sample size is adequate for 95% level of significance and 80% power of the test. One hundred cases were selected by calculating the sample size. Death cases and controls were selected after matching with the major criteria. Every case was compared with a control, leading to a total sample size of 200 (12). Patients who attended the Centre were mainly of low socioeconomic status and came either from Dhaka city or from its surrounding areas. Patients with severe diarrhoea or dysentery with complications, such as pneumonia, suspected sepsis, severe malnutrition, or patients of extreme age, such as infants, and those aged over 65 years, were hospitalized. Approximately, 5% of patients who visit the ICDDR,B hospital are admitted to the inpatient ward. It was possible to get clinical findings of patients who died within a short period after admission. Rectal swabs or stool culture and microscopic examinations were routinely done for all admitted patients. Blood culture, white cell count, and serum electrolytes were analyzed in most cases. On suspicion of a severe respiratory disease or any gastrointestinal complications, an X-ray was taken. Surgery or peritoneal dialysis facilities were not available, and patients who required such treatment were transferred to other hospitals. All cases were severely malnourished defined by Gomez classification weight-for-age <60% of median of the National Center for Health Statistics. For each case, a matched control was identified who was admitted during the same period (within 3 days) and was of the same sex but recovered from their illness. Patients suffering from any chronic illness or those who were refer-red to other hospitals or left the hospital against advice of the physicians were not included. To avoid confounding effects, individuals isolated with enteropathogens other than S. dysenteriae type 1 or S. flexneri were excluded. Clinical information on age, sex, socioeconomic status, duration of hospitalization, duration of vomiting and diarrhoea prior to admission, history of seizures, and current and past breastfeeding status, when available, was obtained from the records of patients. Clinical findings on admission included signs of kwashiorkor, abdominal distension, absent or sluggish bowel sound, rectal prolapse, xerophthalmia, altered consciousness, lethargy, coma, anaemia, bronchopneumonia, hypothermia, sepsis, pulse rate, and dehydration. Laboratory investigations included stool microscopy, white blood cell and plate-let count, haematocrit, blood glucose level, isolation of bacteria, serum creatinine, and serum electrolytes, such as Na, K, Cl, and TCO2. Statistical analysis Data were entered into the microcomputer and checked using a software (SPSS version 7.5). Comparison of continuous variables between cases and controls was done with the Student's t-test for normally-distributed data or with the Mann-Whitney U-test for non-normal distribution. Categorical variables were analyzed with the chi-square test. Fisher's exact t-test was used where the expected count was less than five. Two-sided significant test was used. To identify the factors independently associated with an increased risk of death, multiple logistic regression analysis was carried out. In a backward step-wise regression, all non-significant variables were eliminated until a final model with significant p values and odds ratios was accessed. ResultsThe clinical characteristics of 52 boys and 48 girls were almost similar (Table 1). The median age of cases and controls was 9 months and 12 months respectively. This difference in age was significant. The proportion of subjects in each age category was comparable between the groups. The average duration of hospital stay was almost two days for the fatal cases and sixdays(p<0.001) for the controls. Recent medical history showed that complaints of coughing were more common in patients who died than in patients who survived. Patients who had cough before admission had a 2.3-time higher chance of death. The presence and duration of diarrhoea and vomiting prior to admission did not differ very much between the cases and the controls. The presence of mucus in stool was more frequent in controls than in cases. Although not significant, bloody stool was more often found in controls than in cases. History of seizures, breastfeeding status, and socioeconomic status were almost similar between the groups. Compared to survivors, the higher number of deceased patients had abdominal distension, absent or sluggish bowel sound, altered consciousness, clinical anaemia, bronchopneumonia, hypothermia, clinical sepsis, low or imperceptible pulse, pulse rate of <90 per minute, and dehydration. Abdominal distension and absent or sluggish bowel sound gave a 1.9- and 3.3-time higher risk of death respectively. The presence of clinical anaemia showed a 2.1-time higher risk of mortality. Altered consciousness on admission was highly associated with death with an odds ratio (OR) of 4.2. A similar effect was seen with hypothermia (OR=7.4). The presence of bronchopneumonia, clinical sepsis, dehydration, and a low or imperceptible pulse volume led to an increased risk of death by 2.8, 4.6, 3.1, and 3.9 folds respectively. The highest OR in univariate analysis was found for imperceptible pulse or a pulse rate of <90 per minute (OR= 10.5). Kwashiorkor, rectal prolapse, and xerophthalmia were not associated with a higher risk of mortality (Table 2). Eighteen patients in the cases and 20 patients in the control group had infection due to S. dysenteriae type 1 (Table 3). S. flexneri was isolated from the remaining patients. The serum creatinine level of >150 mmol/L was more frequently observed in patients with afatalout-come (p<0.001), and hyperkalaemia was alsoprominent(p<0.05) in the fatal cases. Five patients had Shigella-associated bacteraemia, four had bacteraemia with other Enterobacteriaceae, and eight had pneumonia-related species in their blood (4 Pseudomonas, 1 Staphylococcus aureus, and 3 Streptococcus pneumoniae). Double patho-gens were isolated from the blood of one patient only. Haematocrit, white cell, and platelet counts were not positively associated with death in these severely-mal-nourished children with shigellosis. Hypoglycaemia was significantly more common in cases (p=0.00) and was strongly associated with death (OR=6.6). Multivariate analysis A list of variables was considered to identify the characteristics, which were independently associated with death. These variables were subjected to multivariate analysis. Initially, age and cough prior to admission were identified. Abdominal distension, absent or sluggish bowel sound, hypoglycaemia, bronchopneumonia, clinical anaemia, clinical sepsis, hypothermia (<36 °C), and altered consciousness on admission were thought to be probable independent risk factors. Age was included, although age-groups were not significantly associated with death, but age as a continuous variable was significant, and the strong impact of age on mortality was also proved in other studies (3,6). Clinical assessment of dehydration in severely-malnourished children is difficult. Therefore, dehydration status was not considered in the final analysis. Since breastfeeding information was inadequate, it was not considered for multiple logistic regression. Results of multiple regression analysis showed that hypothermia, altered consciousness, hypoglycaemia, and bronchopneumonia were significantly associated with death (Table 4). The number of patients included in the analysis was 139; data for 61 patients were missing. The initial number of variables for which the analysis was done was 11. Age, history of cough, absent or sluggish bowel sound, abdominal distension, clinical sepsis, hyperkalaemia, and clinical anaemia were removed from analysis after they were proved not to be significant. The variables which were not included were: age (adjusted p value 0.60), cough on admission (adjusted p value 0.54), absent or sluggish bowel sound (adjusted p value 0.91), abdominal distension (adjusted p value 0.93), clinical anaemia (adjusted p value 0.11), clinical sepsis (adjusted p value 0.55), and hyperkalaemia (adjusted p value 0.64). DiscussionBoth malnutrition and shigellosis are major causes of deaths of children in developing countries (1,11,12). The risk factors identified in this study would be useful for the treatment of severely-malnourished children with S. dysenteriae type 1 or S. flexneri. Assertive earlier management with appropriate antibiotics, provision of adequate nutritional therapy, close monitoring of temperature, blood glucose, and mental status could prevent complications or secondary infections in these patients. Infection, such as bronchopneumonia, appears to be more predictive for death than severity of colitis. Death of patients with shigellosis in general is most often due to a superimposed infection (4). In addition, malnutrition worsens the prognosis due to reduced immunity (13). In our study, clinical septicaemia as manifested with altered consciousness, low-volume pulse, bradycardia, and hypothermia was significantly more frequent in the fatal cases. Blood and mucus in stool, duration of diarrhoea and vomiting, and severe colitis were more frequent in cases than in controls. Hypothermia and hypoglycaemia were important risk factors for death in children with shigellosis (6) and in children with severe protein-energy malnutrition (13). In previous studies, altered consciousness and unconsciousness were shown to be associated with higher mortality (6,14), and further bronchopneumonia was also recognized as a risk factor (4,6). Four factors have been identified in our study, i.e. hypothermia, hypoglycaemia, bronchopneumonia, and altered consciousness were predictive for death, which confirms results of some earlier studies (6,7). Although S. dysenteriae type 1 is characteristically associated with the highest case-fatality rate compared to other Shigella species, in this study, infection due to S. dysenteriae type 1 was detected in 18 of the 100 cases who died in the hospital and this was detected in 20 patients in the control group. As the patients infected with S. dysenteriae type 1 are more severely ill (6,11), they are often referred to other hospitals for the treatment of complications and are more often likely to be discharged against medical advice. The other reasons might be that its alarming features trigger caretakers to seek medical care at an early stage of the disease, which prevents the development of lethal complications (6,11). S. dysenteriae type 2-20 have less clinical severity than type 1 and ac-count for 8% of all S. dysenteriae types (10). The data used in this study were obtained from admitted patients in the ICDDR,B hospital which is specialized in the management of diarrhoea and, as such, do not fully represent the whole population of severely-malnourished children in Bangladesh. Therefore, the data are likely to differ from those of the average population of the country who suffer from shigellosis. The patients who were referred to other hospitals might have some positive impact by aversion in this study. For cultural reasons, parents prefer that their children die at home rather than outside, and many patients who left against medical advice were critically ill. Similarly, the patients whose complications were not treatable in this hospital were referred to other hospitals. Their condition was critical at the time they were transferred to other hospitals. Results of a previous study suggest that the clinical features of those patients more closely resembled patients who died than those who were discharged alive (6). The results of our study suggest that early diagnosis of shigellosis in severely-malnourished children and assertive therapy for proper management to prevent and treat hypothermia, hypoglycaemia, bronchopneumonia, or altered consciousness are likely to reduce Shigella-related mortality in severely-malnourished children. AcknowledgementsThis research was funded by ICDDR,B: Centre for Health and Population Research and its donors which provide unrestricted support to the Centre for its operations and research. Current donors providing unrestricted support include: Australian International Development Agency (AusAID), Canadian International Development Agency (CIDA), Department for International Development (DFID), UK, Government of Bangladesh, Government of Japan, Government of Sri Lanka, Government of the Netherlands, Swedish International Development Cooperative Agency (SIDA), The Kingdom of Saudi Arabia, and Swiss Development Cooperation (SDC). The authors gratefully acknowledge these donors for their support and commitment to the Centre's research efforts. References
© 2005 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn05033t1.jpg] [hn05033t4.jpg] [hn05033t3.jpg] [hn05033t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}