 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 23, No. 3, Sept, 2005, pp. 275-281 A Comparison of Two Systems for Chlorinating Water in Rural Honduras Amy K. Henderson1 , R. Bradley Sack1 , and Erick Toledo2 1 Johns Hopkins Bloomberg School of Public Health, Baltimore, MD 21205, USA, and
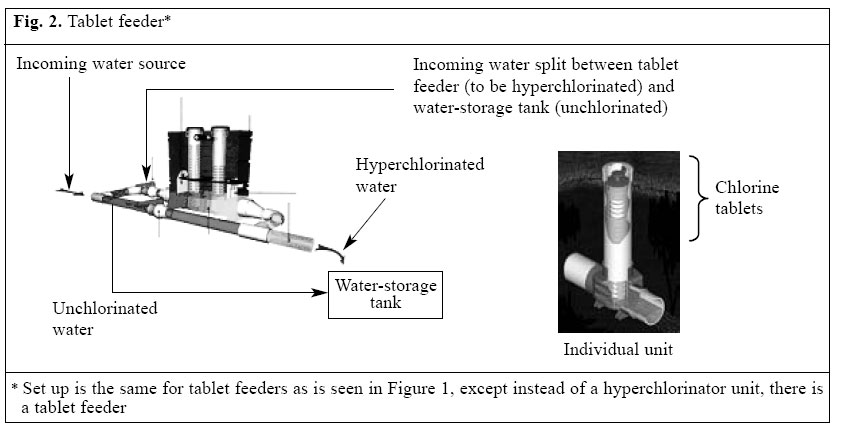
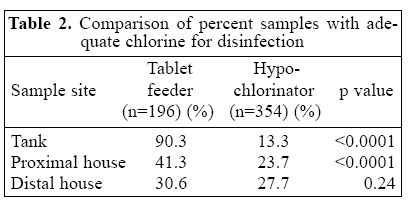
2 International Center, 731 8th Street, S.E. Washington, DC 20003, USA Code Number: hn05035 ABSTRACT This study investigated a small subset of the two community water-disinfection systems - hypochlorinators and tablet feeders - in rural Honduras. Levels of residual chlorine were assessed at three locations within the distribution system: the tank, the proximal house, and the distal house. The levels of residual chlorine were compared with the standard guidelines set by the Pan American Health Organization and the Inter-national Rural Water Association for potable water that require a minimum of 1.0 (tank), 0.5 (proximal house), and 0.2 (distal house) ppm for each location. The levels of residual chlorine were also compared across systems, e.g. hypochlorinators to tablet feeders. At the tank and proximal house, tablet feeders had significantly higher mean values for levels of residual chlorine (measured in ppm) than hypochlorinators (tank: 1.20 vs 0.67; proximal house: 0.44 vs 0.32, p<0.001 for both) with no significant difference at the distal house (0.16 vs 0.16). At the tank and proximal house, tablet feeders were more likely to meet recommended standards than hypochlorinators (90.3% vs 13.3%, p<0.0001 and 41.3% vs 23.7%,p<0.0001) with a smaller difference seen at the distal house (30.6% vs 27.1%, p=0.24). The apparent dichotomy in chlorine levels of tablet feeders (e.g. between tank/proximal house and distal house) is discussed. The results suggest that tablet feeders may be more effective than hypochlorinators in supplying clean water in rural, resource-poor settings and possibly serve as an alternative technology for water disinfection. Further research on techniques for empowering and building capacity within community water boards will help organize and introduce sustainable water systems in developing countries. Key words: Drinking-water; Chlorine; Diarrhoea; Water supply; Water quality; Water microbiology; Observational studies; Honduras Introduction The population of Honduras is largely concentrated in rural areas (1). Although the Government of Honduras has sought to implement sustainable water systems in rural areas, the prevalence of diarrhoeal disease in children continues to be high. In 1996, the National Survey of Epidemiology and Family Health in Honduras found diarrhoeal disease to be one of the top three leading causes of death among children aged less than five years (2,3). In the same year, the prevalence of diarrhoeal disease in children aged less than five years was 21% (2,3). In 2000, 81% of rural and 95% of urban populations had access to clean water (4). These statistics can be misleading, however, as they represent only the proportion with access to a government-established water system and not the proportion of systems functioning at acceptable standards of water quality (2,3,5-8). Having access to a water disinfection system is not necessarily equivalent to having access to clean water. Studies have left the relationship between provision of clean water and reduction in rates of childhood diarrhoeal disease controversial. While several studies have shown a relationship, those that conclude no difference in rates of diarrhoeal disease suggest that clean water, in and of itself, is not sufficient without behavioural modifications and improvements in sanitation (10-20 and Caudill H. Personal communication, 2003). It is generally agreed upon, however, that clean water should still be a priority for all communities, and this will, whether alone or in conjunction with environmental changes, contribute to a reduction in the overall burden of diarrhoeal disease. Despite the continuing problem of provision of clean water throughout the developing world, we are unaware of any published studies that have com-pared different types of disinfection systems. In this study, we examined a small subset of the two most commonly-used systems - hypochlorinators and tablet feeders - in Honduras in an effort to generate data and discussion towards the improvement of clean water provision systems not only in Honduras, but throughout the developing world. Chlorine disinfection systems Chlorine is the most widely-used water disinfectant in the world. There are three forms of chlorine currently in use: granulated, tabular, and liquid. Liquid chlorine is only being used in selected homes and not for disinfecting community water supplies and will not be discussed further here. The two most widely-used systems in Honduras are those that use granulated chlorine, termed 'hypochlorinators', and those that use tablets, called 'tablet feeders'. Irrespective of the form of chlorine, the principles of system function are the same. Each community has one or more large tank(s) for water storage attached to a distribution system of lead or plastic piping. Atop each tank is a smaller vessel, called a hyperchlorinator which houses the chlorine (Fig. 1) (8,9). Incoming water sources (e.g. from streams, rivers, surface water, etc.) enter the system by gravity feed or pump, and the majority of water is diverted to the tank for storage without passing through the chlorinating mechanism. A smaller proportion of incoming water enters the hyperchlorinator where it is hyperchlorinated and fed into the larger storage tank. This hyperchlorinated solution diffuses through the water in the storage tank yielding a potable drinking-water source with appropriate levels of residual chlorine for continual disinfection during distribution (8,9). Hypochlorinators Hypochlorinators have been used in Honduras for over 30 years and are managed centrally by the Government (9,10,11 and Banegas P. Personal communication, 2004). They use granular chlorine which is both inexpensive and often produced locally. Once placed in the hyper-chlorinator, the granulated chlorine disinfects the water but typically dissipates quickly (Fig. 1) (5,8,12 and Caudill H. Personal communication, 2003). This requires frequent maintenance by plumbers (volunteers in the community responsible for maintaining water systems) (5,8). Granular chlorine is heavy and generally settles to the bottom of the hyperchlorinator (8,9,11). Unless the granulated chlorine is regularly mixed with incoming water (e.g. by hand or some other means), it will not be completely solubilized. The resulting water source will be unpredictably and inadequately chlorinated. The granulated nature of the chlorine also makes it prone to obstructing or corroding the exit tubing, thereby reducing the quantity and quality of the hyperchlorinated water that enters the storage tank (7,8). Tablet feeders Tablet feeders have been used in Honduras for just over five years and are managed privately by the Honduran Association of Management Boards of Water Systems (AHJASA) (9,11,12 and Banegas P. Personal communication, 2004). They currently supply clean water to 10% of the population throughout Honduras (9,11,12). Com-pared to granular chlorine, tabulated chlorine is more expensive (1.5 US$ per person per year compared to 0.60 US$ for granular chlorine) and largely manufactured outside the country of need (10,11 and Caudill H. Personal communication, 2003). Each tablet feeder holds several chlorine tablets (number determined by the size of each system) allowing for fewer chlorine replenishments over a given period of time (5,8,9,10,11). Tablets are firm and dissolve much slower than granular chlorine, thereby functioning as a 'time released' system of chlorine (Fig. 2) (5,10,11). This allows for more consistent levels of residual chlorine in the water (10-12). Materials and Methods Study area The study was conducted within the Department of Francisco Morazon in Honduras. Francisco Morazon was chosen for logistical reasons as most of its rural communities are within driving distances from the capital city Tegucigalpa. Study design Sampling and data collection We selected five tablet feeders and eight hypocholorinators in communities that were felt to be similar in population, level of sanitation, and water source, e.g. rivers, streams, surface water, etc. Samples were drawn from the two systems on a weekly basis from 24 July to 20 December 2003. Communities were not aware of the time/day that samples were taken to minimize local plumbers from refilling chlorine supplies in anticipation of testing. Twelve students were chosen from the Environmental Sciences Department of the Universidad de Catolica in Tegucigalpa to perform the sampling. Students were trained in data collection, documentation, and reporting and were supervised locally by the dean of their department. Levels of residual chlorine were measured for each sys-tem at three locations: (i) the water tank, (ii) the first home in the distribution system (termed 'proximal' for data recording and analysis), and (iii) the last home in the distribution system (termed 'distal' for data recording and analysis). Samples from the water tank were taken from the storage tank, not the hyperchlorinaters (Fig. 1-2). Vials were capped and placed in the calibrated Hach meter. During each site visit, the colorimeter was first calibrated using a vial of water provided by the Hach Company. Samples at the house were taken only from the tap and not water stored within the home (to avoid variation in mean levels of residual chlorine secondary to differences in water-storage time and/or the types of water-storage containers) (20). The tap was allowed to run 3-5 seconds before vials were placed for sample collection. To reduce subjective bias in measurement of chlorine, a digital device measuring chlorine levels to two decimal places was used - called the Hach DR/890 (Hach Company, PO Box 389, Loveland, CO 80539, USA). Although most people living in rural communities are accustomed to having their water checked, it was emphasized during training that permission be obtained prior to checking water at the homes (12). Trainees were advised to inform people that they were working on a water-quality project and would re-visit on a weekly basis. Upon first-time arrival at each community, trainees were to contact local community plumbers to direct them to tanks and proximal/distal homes within the distribution system. Documentation Measurements of residual chlorine were documented in the field on pre-printed templates and transferred weekly to Excel spreadsheets. All paper copies were kept for verification. Data were submitted electronically for analysis, and preliminary results were transmitted back to the students to demonstrate study progress and enhance the quality of their education. Data analysis Levels of residual chlorine were evaluated based on para-meters set for safe drinking-water by the Pan American Health Organization (PAHO) (Rojas R. Personal communication, 2004), International Rural Water Association (IRWA) (Stottlemyer F. Personal communication, 2004), and Environmental Protection Agency (EPA) (Banegas P. Personal communication, 2004). The standard parameters require levels of minimum residual chlorine of 1.0 ppm in the tank, 0.5 ppm at the proximal house, and 0.2 ppm at the distal house. (Rojas R. Personal communication, 2004; Banegas P. Personal communication, 2004). Patrick Banegas, Superintendent of the Anthony Water and Sanitation District in New Mexico for EPA and a member of the Board of Directors for the IRWA, stated that, in the United States, "EPA drinking water regulations require that they maintain at least a 0.2 mg/L (mg/L equivalent to ppm) at the end of the line…. In order to maintain a 0.2 mg/L residual at the last connection, a 1.0 mg/L residual must be present and maintained at the storage tank" (Stottlemyer F. Personal Communication, 2004; Banegas P. Personal communication, 2004). In Latin America, the standards are similar. According to Ricardo Rojas from PAHO - Latin America, "The concentration of water from the tank to the distal house should remain within 0.2 to 1.0 mg/L. In cases of emergency, however, a minimum level of 0.5 mg/L is recommended at the distal house" (Rojas R. Personal communication, 2004). PAHO considers 0.6-1.0 mg/L an appropriate range for potable water at the level of the tank (21 and Rojas R. Personal communication, 2004). Mean and standard deviations of levels of residual chlorine for each system (broken down by tank, proximal house, and distal house) were calculated, and the student's t-test was used for comparing means. A variation of the sign test was also used for determining the percentage of samples in each system that met the standard recommendations for clean drinking-water. The standard levelofsignificance(p<0.05) was used for both the tests. Results Levels of residual chlorine at each of the three sample sites were compared across the two systems and to the published guidelines. In total, 196 tablet feeder and 354 hypochlorinator samples were taken (Table 1). At the tank and proximal house, tablet feeders had significantly higher mean values for levels of residual chlorine (measured in ppm) than hypochlorinators (tank: 1.20 vs 0.67;proximalhouse: 0.44 vs0.32,p<0.001 for both). There was no significant difference in the mean levels of residual chlorine at the distal house (0.16 vs 0.16). Hypochlorinators also demonstrated a greater degree of variance in levels of residual chlorine between communities than did tablet feeders (tank: 0.50 vs 0.06; proximal house: 0.32 vs 0.33; and distal house: 0.22 vs 0.09) at the level of the tank and distal house (Table 1). Although the range of levels of residual chlorine was zero to over one in both the communities, the percentage of samples that met the minimum recommended chlorine levels for disinfection was markedly different between the two systems (Table 2). At the level of both tank and proximal house, the percentage of samples that met the minimum recommended level of chlorine was 90.3% in the tablet feeders compared to only 13.3% in thehypochlorinators (p<0.0001) and 41.3% and 23.7%(p<0.0001) respectively at the proximal house. As expected from the mean data, there was a small difference at the distal house between tablet feeders and hypochlorinators (30.6% and 27.1% respectively, p=0.24), but this difference was not statistically significant (Table 2). Discussion This study sought to determine if tablet feeders were more effective than hypochlorinators in disinfecting water in resource-poor settings. The data demonstrated that tablet feeders do yield potable water at significantly higher rates than hypochlorinators at the level of both tank and proximal house. Although tablet feeders also demonstrated adequately-chlorinated water at slightly higher rates at the distal house, the difference was not statistically significant. Based on the evidence from this small observational study, we conclude that tablet feeders seem to chlorinate water as (if not more) reliably and effectively as conventional hypochlorinators. The distal house Both the systems had low levels of residual chlorine at the distal house. This was expected in the hypochlorinator communities, since they also demonstrated low mean levels of residual chlorine at the tank and proximal house. This outcome was not expected with tablet feeders, how-ever, as levels of chlorine were generally high at the tank and proximal house. The IRWA suggested that the novelty of tablet feeders was likely to account for the paradox (10 and Stottlemyer F. Personal communication, 2004). Plumbers are still learning how to determine the number of tablets needed per community which can change quickly with the addition of new homes to the distribution system, for example. New homes increase the distance water must travel from the tank to the tap and, because chlorine dissipates over time as a gas, the detectable levels of residual chlorine also decrease (1,5, 6,9,10 and Stottlemyer F. Personal communication, 2004). Limitations of the study There were many limitations of the study that must be considered in the analysis of data. Although we were able to detect statistically significant differences in the two systems with sufficient power, it would have been ideal to examine more systems. Although the initial design had incorporated more systems, several factors cur-tailed the numbers used. Systems are very difficult to access as many roads into rural communities are unpaved and require four-wheel drive vehicles. Systems that function by gravity feed sit atop mountains which require up to an hour's hike to reach. These factors were further complicated by the rainy season which limits access to entire communities for several months. The systems chosen to study, however, were representative of similar regions of Francisco Morazon to generate a fair distribution in terms of geography, access, level of sanitation, and source of water, e.g. rivers, streams, surface water, etc. It should also be emphasized that tablet feeders and hypochlorinators are managed differently. The Honduran Association of Management Boards of Water Systems (AHJASA) privately manages tablet feeders in a decentralized fashion compared to the Government which centrally manages hypochlorinators. As with many types of community health initiatives, a more decentralized approach to water provision generated more community ownership, capacity-building, quality assurance, super-vision, and accountability. The AHJASA has a very effective and innovative system for provision of water in resource-poor settings, and further research comparing the two forms of management could prove useful in establishing/organizing sustainable water systems in rural areas of developing nations. Differences in management could also contribute to differences in quality and consistency of function seen in each of the two systems. Application In theory, because hypochlorinators and tablet feeders use chlorine, they should be able to disinfect water equally well - provided each system is functioning at standard. We have noted both through field visits and documented evidence that hypochlorinators tend to require more frequent maintenance, repair, and replenishments of chlorine. In this regard, tablet feeders, from a purely technologic vantage, are superior. Tablet feeders are more expensive; however, each community must examine the cost-benefit ratio carefully. For many communities, the benefits will outweigh additional costs. Plumbers in most developing countries are volunteers and rely on their regular full-time jobs for income-generation. This often requires them to travel to urban centres for a week or more at a time typically leaving none to monitor the water. When they return, the water is checked, and additional chlorine is added as needed. In these settings, predictable performance is of paramount importance for the safety of the community. A system that requires frequent replenishments of chlorine and/or presents with repeated malfunctions is likely not to receive the attention necessary to assure the predictable output of potable water to the community. This can result in community-wide outbreaks of diarrhoeal disease in children with the most devastating impact on children aged less than five years (2,12,16,18, 20). Depending on the type and number of systems over-seen and the geographical limitations, a high level of quality assurance may simply be too difficult to maintain, especially when systems are managed centrally and staff tend to be over-stretched and under-paid (5-10,13 and Caudill H. Personal communication, 2003). Technological efficiency and reliability becomes increasingly important, and communities may decide that the additional costs are worthwhile for the safety of the community. The results of the study suggest that tablet feeders may be more effective than hypochlorinators in supplying clean water in rural, resource-poor settings and possibly serve as an alternative technology for water disinfection. Further research should examine additional systems and techniques for empowering and building capacity within community water boards - both of which will help organize and introduce sustainable water systems in developing countries. Acknowledgements The authors thank the International Center in Washington, DC, for providing the financial support for the study; the university students and dean at the Universidad de Catolica, Tegucigalpa, Honduras, for collecting the samples, documenting, and reporting their findings; and Hach for donating one of the Hach DR/890 chlorine colorimeters used in the project. The authors also thank both National Rural Water Association and Dr. Kellogg Schwab at Johns Hopkins Bloomberg School of Public Health for serving as technical consultants for the study. References
© 2005 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn05035t1.jpg] [hn05035f1.jpg] [hn05035f2.jpg] [hn05035t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}