 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
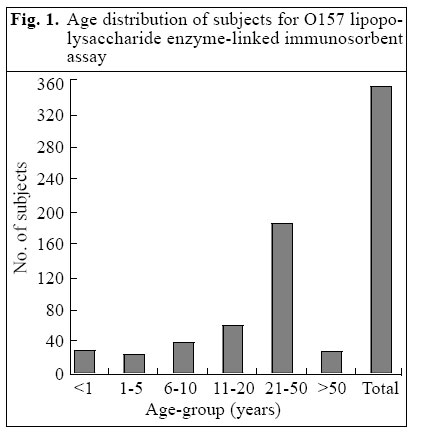
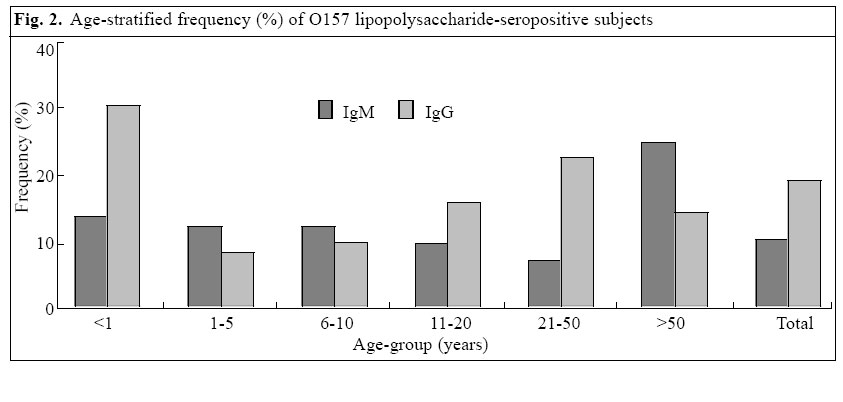
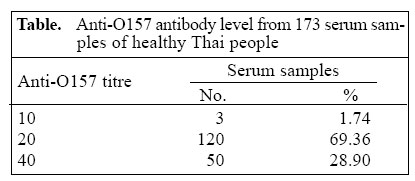
Journal of Health, Population and Nutrition, Vol. ,23 No. 4, December, 2005, pp. 305-310 Antibodies among Healthy Population of Developing Countries against Enterohaemorrhagic Escherichia coli O157:H7 Supayang Piyawan Voravuthikunchai1,2, Chitamas Chaowana1, Prarin Perepat1, Tetsuya Iida3, and Takeshi Honda3 1Department of Microbiology,2Natural Products Research Unit, Faculty of Science, Prince of Songkla University, Hatyai, Songkla 90112, Thailand and 3Department of Bacterial Infections, Research Institute for Microbial Diseases, Osaka University, 3-1 Yamadaoka, Suita, Osaka 565-0871, Japan Correspondence and reprint requests should be addressed to: A/Professor Supayang P. Voravuthikunchai Department of Microbiology and Natural Products Research Unit Faculty of Science Prince of Songkla University Hatyai, Songkla 90112 Thailand Email: supayang.v@psu.ac.th Fax: +66-74-446661Code Number: hn05041 ABSTRACT In Thailand, no reports are available on Escherichia coli serotype O157:H7, a causative agent of severe bloody diarrhoea, sometimes associated with haemolytic-uraemic syndrome and thrombotic thrombo-cytopenic purpura. The reason for the non-identification of infection due to E. coli O157 in this country and in other developing countries has not been rigorously discussed. The aim of this study was to determine the humoral response against the infectious organism. The IgM and IgG antibody responses against E. coli O157 lipopolysaccharide were studied using indirect enzyme-linked immunosorbent assay. Three hundred and thirty-two serum samples obtained from healthy blood donors and patients with diseases unrelated to diarrhoea were investigated. With a cut-off value of mean +2 SDs for each age-group, the frequency of the IgM and IgG responses to O157 lipopolysaccharide was 11.74% (39 of 332 samples) and 22.59% (75 of 332 samples) respectively. Furthermore, agglutination test of 173 subjects revealed titres ranging from 10 to 40 in all the samples. The results suggest possible exposure of the Thai population to cross-reacting antigens from other intestinal organisms in addition to infection due to E. coli O157:H7. Key words: Escherichia coli, Enterohaemorrhagic; Escherichia coli O157:H7; Antibody formation; Immunity; Immune response: Haemolytic-uraemicsyndrome; Colitis, Haemorrhagic; Thrombotic thrombocytopenic purpura;Verocytotoxins; Thailand Introduction Enterohaemorrhagic Escherichia coli (EHEC) or verocytotoxin (VT)-producing E. coli or Shiga-like toxin-producing E. coli is well-recognized as a major foodborne pathogen. Infection, especially in infants and young children, with mainly serotype O157:H7 has recently become a public-health problem of serious concern. Persons infected with E. coli O157:H7 develop haemorrhagic colitis, with characteristic symptoms of bloody diarrhoea and abdominal cramps, that can progress into a more severe, life-threatening complication known as haemolytic-uraemic syndrome and thrombotic thrombocytopenic purpura (1-7). Isolation of E. coli O157 from clinical sources has been reported in China (8), Hong Kong (8), Korea (9), and India (10). The incidence of this bacterium is low in Asian countries, except Japan. The largest outbreak of E. coli O157:H7, acquired mainly through consumption of bovine products, reported to date, occurred among Japanese people in 1996 (11). In Thailand, there have been no reports of haemolytic-uraemic syndrome or haemorrhagic colitis in association with E. coli O157:H7. This infectious agent was not found (12) or scarcely reported (13-14). There are a number of possibilities: (a) in general, the prevalence of EHEC is not high in Thailand; (b) EHEC is present but no infections occur due to the development of some immunity; (c) EHEC is present and cases are also present, but so far they remain undetected because of inappropriate laboratory diagnosis as most routine practices are set up for non-lactose fermenters. Culturing for EHEC can be difficult since EHEC has to be recognized among other E. coli. Relying on the sorbitol reaction is not enough as there are O157 that are not distinct on sorbitol plates. Therefore, developing an enzyme-linked immunosorbent assay (ELISA) for use in diagnostics and epidemiology is of great value. In this study, we first employed an indirect ELISA to detect immunoglobulin M (IgM) and IgG to E. coli O157:H7 lipopolysaccharide. This was followed by determining antibody titre in the sera using a direct agglutination test. The aim of the study was to determine the humoral response against E. coli O157:H7. The results of the study illustrated a significant frequency of E. coli O157:H7 antibodies developed among the Thai population. Materials and Methods Extraction of E. coli O157:H7 lipopolysaccharide Human sera Three hundred and thirty-two serum samples were obtained from the Hatyai Hospital, Songkla province, Thailand, during August 2000-September 2002. Serum samples were randomly selected from healthy blood donors and from patients whosesera were investigated in our hospital for other illnesses unrelated to diarrhoea. Written informed consent was obtained from each adult or care provider of minor ones in every case. The age distribution of Thai subjects is presented in Fig. 1. In addition, 15 sera obtained from healthy adults in Japan were included in the study. All serum samples were immobilized by heating at 56 °C for 30 minutes and were stored at -20 °C until tested. Enzyme-linked immunosorbent assay for antibody to E. coli O157:H7 lipopolysaccharide IgM and IgG to E. coli O157:H7 lipopolysaccharide were detected using the modified indirect ELISA method (18). The diluent and the wash solution were phosphate buffer saline and phosphate buffer saline-0.05% tween 20 (phosphate buffer saline-T) respectively. A 96-well flat-bottom microtitre plate (NUNC 2-69620; GIBCO BRL, Burlington, Ontario, Canada) was coated with 100 μL of purified E. coli O157:H7 lipopolysaccharide (1 μg/mL in phosphate buffer saline) by incubation at 37 °C for one hour and overnight at 4 °C in a humidified chamber. Phosphate buffer saline was substituted for E. coli O157:H7 lipopolysaccharide in the antigen control wells. After re-warming the plates at 37 °C for one hour, the wells were washed three times with phosphate buffer saline-T (200 μL/well), treated with 0.5% bovine serum albumin in phosphate buffer saline (100 μL/well) for 30 minutes at 37 °C in a humidified chamber for blocking and then washed three times with phosphate buffer saline-T. One hundred μL of each sample (diluted 1:320 in 0.1% bovine serum albumin + phosphate buffer saline-T) was added to antigen-coated and control-wells and then incubated at 37 °C for one hour in a humidified chamber. After washing the plates three times with phosphate buffer saline-T, 100 mL of goat anti-human IgG (Fab-specific) and IgM (m-chain-specific), conjugated to alkaline phosphatase (Sigma, St. Louis, Missouri, USA) and diluted 1:1,000 in 0.1% bovine serum albumin + phosphate buffer saline-T was added to each well, and the plates were incubated for one hour at 37 °C in a humidified chamber. After five washes with phosphate buffer saline-T, 100 μL of substrate solution (1 mg/μL disodium r-nitrophenyl-phosphate hexahydrate (Sigma, St. Louis, Missouri, USA) was added to each well, and the plates were incubated at room temperature for 10-30 minutes in darkness. Determination of cut-off values The optical density values at 405 nm were measured in a micro-plate ELISA reader (ELX800, BIO-TEK®, USA). For each assay, the mean optical density values were calculated by averaging triplicate values for each test- and control-well. The latter was subtracted from the former to obtain the net ELISA value. The cut-off values were chosen to be 2 SDs above the mean for each age-group. Determination of anti-O157 antibody titre A direct agglutination test was carried out. Serum sam-ples were immobilized by heating at 56 °C for 30 minutes. They were first diluted 1:10, followed by two-fold dilutions with sterile saline in U-bottom microtitre plates. An equal volume of the antigen solution prepared from heat-killed E. coli O157:H7 was added. Agglutination titre was determined as the reciprocal of the highest dilution of the serum that gave any evidence of agglutination. Results ELISA for IgM and IgG to E. coli O157:H7 lipopolysaccharide To optimize the serum dilution, 10 control sera were tested over a range of dilutions from 1:80 to 1:1,250. A dilution of 1:320 appeared to be optimal and was used subsequently. On the basis of the ELISA cut-off value of mean +2 SDs of each age-group, 39 of 332 subjects (11.74%) and 75 of 332 subjects (22.59%) were positive for IgM and IgG to E. coli O157:H7 lipopolysaccha-ride respectively. The age-stratified frequency (%) of O157 lipopolysaccharide seropositive subjects is summarized in Fig. 2. Limited data with 15 healthy Japanese subjects aged 21-50 years showed no IgM response, and only one serum had IgG response (6.67%). Agglutinating titres against E. coli O157 Of 173 serum samples obtained from subjects aged 21-50 years, all the sera had agglutinating titre ranging from 10 to 40 (Table). Approximately, 70% of the subjects had a titre of 40, with only 1.74% with a titre of 10. In contrast, all the Japanese sera obtained from healthy subjects had agglutinating titre of less than 10 (results not shown). Discussion Our ELISA was similar to that of others described (18-21) for the detection of antibodies to E. coli O157 lipopolysaccharide. Different methods have been approached to establish the cut-off values. Using relatively high numbers of subjects and by subtracting background signals, our cut-off value was set at the mean ELISA value of each age-group +2 SDs. Sera from 332 Thai subjects were tested for the presence of IgM and IgG to E. coli O157 lipopolysaccharide. Overall, 11.74% and 22.59% of the subjects tested were positive for IgM and IgG respectively. This was expected since most rural Thai people are obviously exposed to many Gram-negative intestinal pathogens. Earlier studies reported cross-reaction of E. coli O157 lipopolysaccharide with antibodies to many other pathogens, such as E. hermanii (22), Citro-bacter freundii (23), Yersinia entercolitica O9 (24), Salmonella O:30 (25), and Brucella abortus (26). We propose that high seropositivity among Thai people may also be due to cross-reacting antibodies of many other intestinal pathogens that are very common in Thailand, in addition to E. coli O157. Our environmental study on diarrhoeal stools and food examination for a long period clearly demonstrated no E. coli O157 recovered from 580 diarrhoeal stools, and 3.47% of the organisms were found from 173 suspected beef-dishes (14). In contrast, Y. enterocolitica comprised up to 21.66%, and other non-sorbitol-fermenting colonies were present at 8.92% of 157 colonies tested (14). C. freundii, another pathogen which carries E. coli O157 antigen (23), was also reco-vered from both clinical and food samples in our previous study (14). More than 100 serotypes of EHEC, including O157:H7 associated with haemorrhagic colitis and haemolytic-uraemic syndrome, have been isolated from cattle or their products (27). Thailand is an agricultural country where a large number of people are exposed to faeces of bovine origin, the natural reservoir of EHEC all their lives. Cross-reactivities between the E. coli O157 serogroup and the E. coli O7 and O116 serogroup have previously been described (28). Other workers reported a similar high rate of isolation of E. coli O157 from 4 (4.21%) of 95 cattle and from 1 (1.81%) of 55 bovine faeces and also reported related anti-O157 antibody among the healthy Thai population to the exposure to E. coli O157 (13). On the other hand, other studies have showed the presence of antibodies to O157 lipopolysaccharide in 12% of the population in rural areas where O157 strains are endemic. Similar results were observed in a rural Wisconsin population (29). O157 lipopolysaccharide antibodies were independently associated with increasing age, sex, manure contact, and sheep contact. The incidence of clinically-recognized diarrhoea was similar among children with and without antibodies to O157 lipopolysaccharide, but the rate of clinic visits for diarrhoea was lower among farm-resident children. Their results are consistent with reduced occurrence of clinical illness from repeated an-tigenic stimulation in a farm environment. Presently, it is unclear which components of EHEC O157 (lipopolysaccharide, H-antigens, Shiga toxins, intimin) induce a protective immunity in the host organism. Sheoran et al. reported that human antibody against Shiga toxin 2 administered to piglets after the onset of diarrhoea due to O157:H7 could prevent fatal systemic complications (30). The data presented in this study demonstrate that antibody titres against O157 lipopolysaccharide are in-deed protective. The ELISA technique has been suggested as well-suited to seroprevalence study (18) since other techniques, such as bacterial agglutination (10), passive haemagglutination (31), and indirect haemagglutination (32), are designed mainly for the serodiagnosis of recent infection and to detect mainly IgM antibodies. Analysis of sera from the healthy Thais in this study showed high seropositivity against E. coli O157:H7. In contrast, Japanese sera demonstrated no antibody against this pathogen (titre less than 10). This could explain the cause of outbreaks in Japan. The results of our study on humoral responses, together with our previous findings that E. coli O157:H7 were uncommon, may suggest that, in the general population of a developing country like Thailand, people may develop some antibodies to E. coli O157:H7 via cross-reacting antigens from other intestinal organisms rather than exposure of the population to E. coli O157 strains. The reason for this lack of infection by this organism in Thailand is more likely related to a different external antigen that develops during the first months of life. Acknowledgements This work was partly supported by a fund from Thai Government budget and Research Institute for Microbial Diseases, Osaka University, Osaka, Japan. References
© 2005 ICDDR,B: Centre for Health and Population Research |

{kind=link}
{kind=link}
{kind=link}