 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
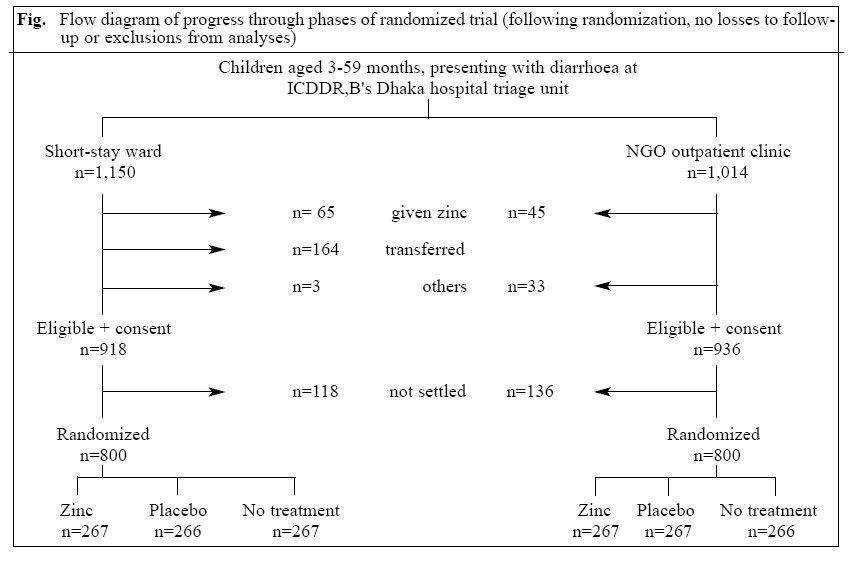
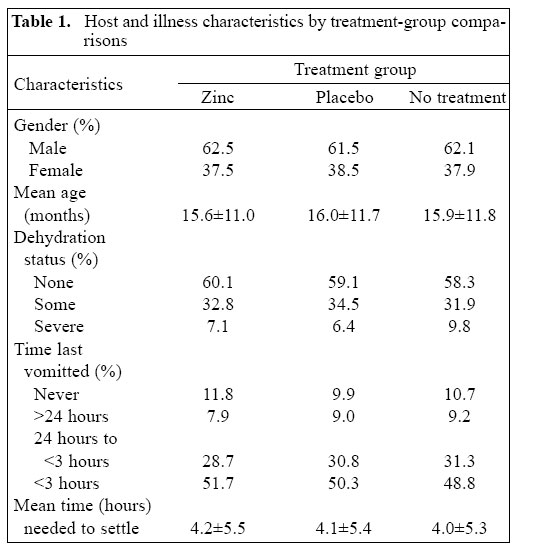
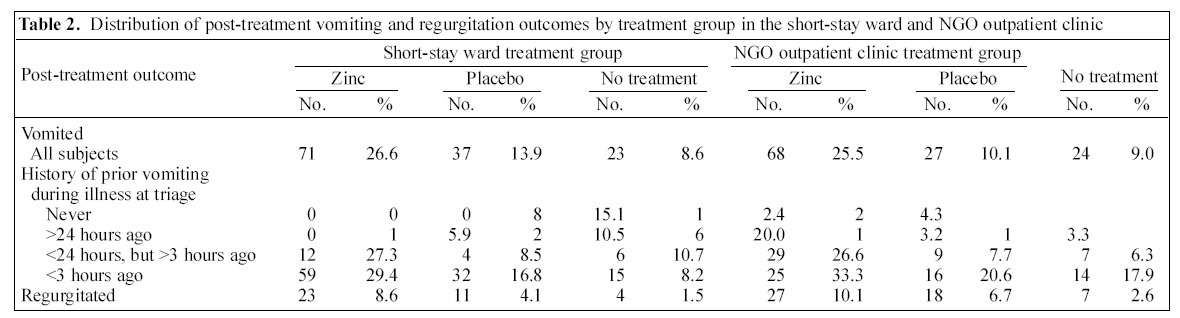
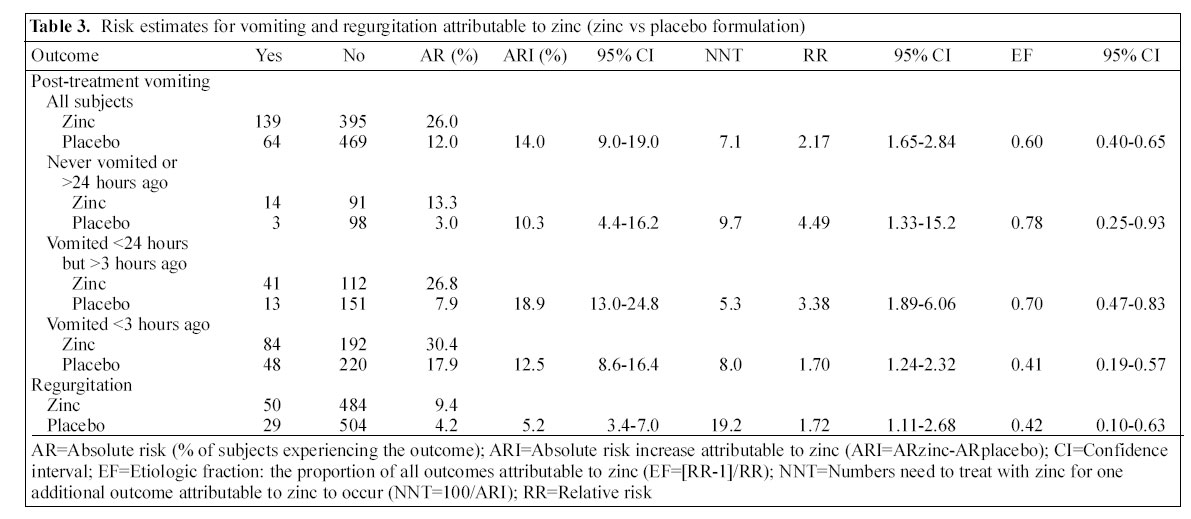
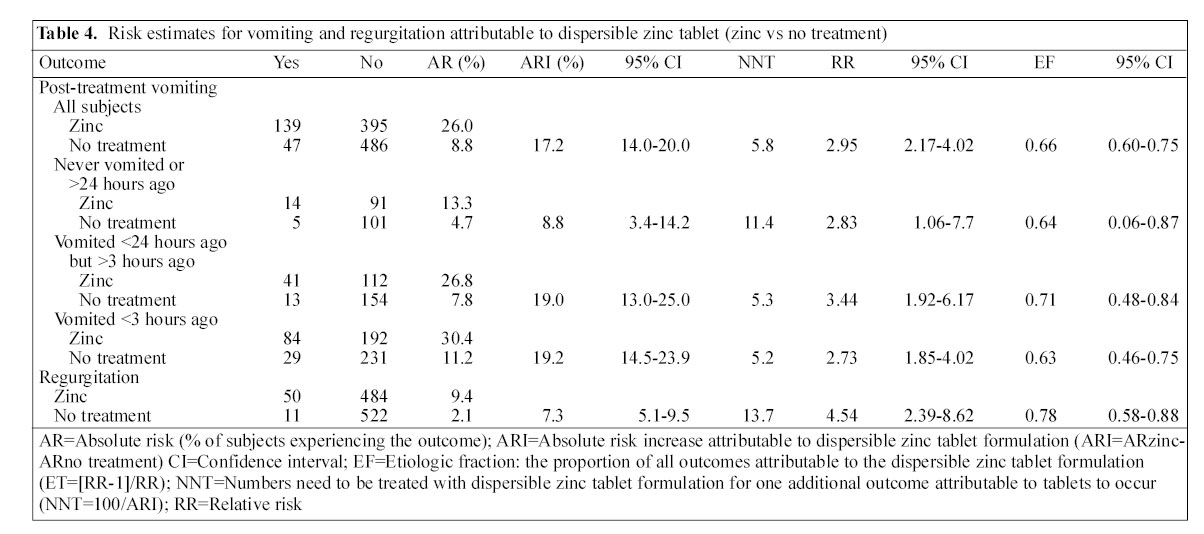
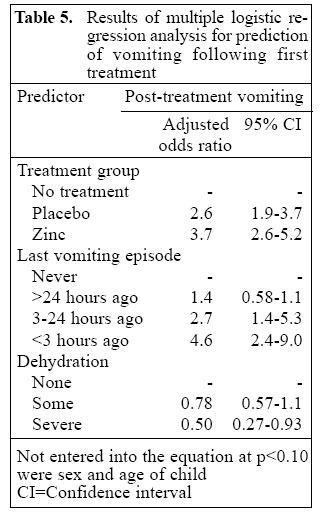
Journal of Health, Population and Nutrition, Vol. ,23 No. 4, December, 2005, pp. 311-319 Initiation of Zinc Treatment for Acute Childhood Diarrhoea and Risk for Vomiting or Regurgitation: A Randomized, Double-blind, Placebo-controlled Trial Charles Palmer Larson1,2, A.B.M. Mominul Hoque1, Charles Philip Larson3, Ali Miraj Khan1, and Unnati Rani Saha1 1ICDDR,B: Centre for Health and Population Research, GPO Box 128, Dhaka 1000, Bangladesh, 2Department of Pediatrics and Department of Epidemiology, Biostatistics and Occupational Health, Faculty of Medicine, McGill University, Montreal, Quebec, Canada, and 3Faculty of Medicine, McGill University, Montreal, Quebec Correspondence and reprint requests should be addressed to: Dr. Charles P. Larson Director Health Systems and Infectious Diseases Division ICDDR,B: Centre for Health and Population Research GPO Box 128, Dhaka 1000 Bangladesh Email: clarson@icddrb.org Fax: (880-2) 8823963 Code Number: hn05042 Abstract The childhood diarrhoea-management guidelines of the World Health Organization/United Nations Children's Fund (WHO/UNICEF) now include zinc treatment, 20 mg per day for 10 days. To determine if a dispersible zinc sulphate tablet formulation is associated with increased risk of vomiting or regurgitation following the initial, first treatment dose, a double-blind, placebo-controlled randomized clinical trial was carried out in the Dhaka hospital of ICDDR,B: Centre for Health and Population Research (n=800) and in an adjacent NGO outpatient clinic (n=800). Children were randomized to one of three groups: no treatment, placebo, or zinc sulphate tablet (20 mg). They were then observed for 60 minutes, and all vomiting or regurgitation episodes were recorded. When compared with placebo, zinc treatment resulted in an attributable risk increase of 14% for vomiting and 5.2% for regurgitation. The median time to vomiting among those receiving zinc was 9.6 minutes and was limited to one episode in 91.2% of the cases. Overall, the proportion of 60-minute post-treatment vomiting attributable to zinc, placebo, and the illness episode was estimated to be 40%, 26%, and 34% respectively. The dispersible zinc sulphate tablet formulation at a dose of 20 mg is associated with increased risks of vomiting and regurgitation. Both are transient side-effects. Key words: Zinc; Zinc therapy; Diarrhoea; Vomiting; Regurgitation; Randomized clinical trials; Placebo; Double-blind method; Bangladesh Introduction It is now one decade since the publication of the landmark article by Sazawal et al. demonstrating the efficacy of orally-administered zinc in the treatment of acute child-hood diarrhoea (1). Since then, several randomized hospital- (2-5) and community-based (6-7) trials have consistently demonstrated the efficacy of zinc treatment for acute or persistent diarrhoea in children aged less than five years. Pooled analyses of published studies clearly demonstrate that zinc reduces the duration and severity of acute and persistent diarrhoea (8,9). The results of these efficacy trials of zinc are now supported by a community-based, effectiveness trial of zinc treatment for acute childhood diarrhoea. In this trial, zinc shortened the duration of illness, reduced the likelihood of a repeat diarrhoea episode, and reduced non-injury mortality by 50% (10). The World Health Organization (WHO) has estimated the burden of global annual mortality attributable to zinc deficiency to be 750,000 deaths per year (11). It is anticipated that over one-half of these deaths could be averted through the successful application of zinc treatment for childhood diarrhoea (12). Given this potential reduction of mortality and the strength of evidence at hand in support of zinc treatment, the WHO/United Nations Children's Fund (UNICEF) issued, in May 2004, a joint statement on updated guidelines for the management of childhood diarrhoea (13). The joint statement includes the recommendation that all children aged less than five years be treated with zinc (20 mg per day if aged 6-59 months and 10 mg per day if aged less than 6 months) for 10-14 days. As health systems proceed with plans to scale up zinc as a treatment for childhood diarrhoea, a common concern that will be expressed among health practitioners is the potential risk for side-effects, particularly vomiting. Transient vomiting or nausea among adults at doses of 50 mg per day or higher are well-known side-effects of zinc (14-16). Whether similar effects at the lower dose of 10-20 mg per day will be observed in children is unclear. Strand et al. reported, in their trial among Nepalese children receiving 15-30 mg of zinc per day, a nearly two-fold increase in vomiting (7). Whether a direct side-effect of zinc or due to inadequate masking of the metallic taste of zinc could not be differentiated. Other trials, including the effectiveness trial of Baqui et al. (10), did not report increased risks of vomiting. In none of the studies cited was the increased risk of vomiting linked to adverse clinical outcomes. At the request of WHO, Rodael Pharma and Nutriset, Ltd. in France developed the technology to produce a dispersible zinc tablet formulation that effectively masks the taste of zinc, is stable at high temperatures and humidity, and can be sold at an acceptable cost. The tablets are distributed in a light weight blister pack of 10-14 tablets. Advantages of the tablets over conventional syrups include their lower cost, much lower weight, ease of distribution, accuracy of dose, and caretaker adherence with a 10-14-day treatment schedule (17). It is anticipated that this dispersible tablet formulation will be used in several scale-up projects throughout the world, with plans already underway for technology transfers in Bangladesh, India, and Pakistan. The aim of this randomized trial was to estimate, at the time of initial administration, the risk of vomiting or regurgitation that can be attributed to the zinc tablet formulation and to differentiate this from the background risk attributable to diarrhoeal illness and any placebo effect. With this information, healthcare providers and caretakers will be better informed of potential side-effects, and providers can carry out appropriate anticipatory counselling. Materials and Methods Study design This randomized, double-blind, placebo-controlled clinical trial was carried out in the short-stay ward of Dhaka hospital of ICDDR,B and in an adjacent NGO outpatient clinic from October to December 2004. Subjects were randomly assigned to receive a 20 mg zinc sulphate dispersible tablet, a placebo dispersible tablet, or neither. Hypothesis That after initiating treatment in settled children, aged less than five years, with diarrhoea, those receiving zinc when compared to those receiving a placebo or nothing will be at increased risk of vomiting and/orregurgitation(p<0.05, one-sided) Study population The source population included children, aged 3-59 months, brought to the Dhaka hospital of ICDDR,B, with a complaint of diarrhoea. On arrival, children are triaged to an intermediate care ward (less than 5%), short-stay ward (50%; those requiring supervised rehydration), or an NGO outpatient clinic located adjacent to the hospital (45%; mild or no dehydration). Any child triaged to the short-stay ward or NGO clinic was eligible for inclusion in the study. Excluded were children returning to the hospital with an ongoing episode of diarrhoea and those who were receiving zinc. Informed, written consent was obtained from the primary caretaker prior to enrollment in the study. Sample size estimation This was based upon a one-sided hypothesis of effect (zinc increases risk) with a level of confidence (1-a) of 95% and a power (1-b) of 80%. The minimal detectable between group difference in the proportion vomiting was set at 0.10 and the baseline probability of vomiting at 0.25. This resulted in an estimate of 231 subjects per group. This was adjusted upwards to 260 per group and stratified for the short-stay ward and NGO clinic settings, thus resulting in a total sample size of 1,560. Randomization A randomization schedule covering 1,600 assignments was prepared based upon the random selection of blocks of six (2 assignments per group). Next, opaque envelopes were numbered and in them was placed the assigned zinc tablet, placebo tablet, or a similar-sized button. The randomization schedule was then placed in a locked cabinet and not opened until completion of the study. Measurement and conduct of trial At entry into the study, a research assistant completed a brief interview to document host and illness characteristics. Either a paramedic or a nurse assessed the enrolled children for eligibility to receive the zinc treatment. Eligibility was defined as having taken oral rehydration solution (ORS) as instructed, no vomiting in the past two hours for the short-stay ward or 30 minutes in the NGO clinic, and no longer dehydrated. At this point, a trained research assistant opened the next available envelope, and the child was given the assigned treatment or nothing. Subjects were then observed for 60 minutes, and all vomiting or regurgitation episodes were recorded. Following one hour of observation, the trial was terminated, and all children were treated with zinc as per the diarrhoea-management protocol of the hospital or the clinic. Rodael Pharma, the French laboratory that developed the dispersible zinc tablet technology, prepared the dispersible zinc and placebo tablets. These are highly sweetened, vanilla-flavoured tablets that have been demonstrated to effectively hide the taste of zinc (17). Vomiting was defined as the forceful emptying of stomach contents. Regurgitation was defined as the unforced return of any amount of the swallowed syrup (within 5 minutes for those receiving a dispersible tablet), liquids, or food.The Ethical Review Committee of ICDDR,B approved the study protocol. Data analysis Data were entered and analyzed using SPSS (PC version 11.0). In a 10% sample of subjects, data were re-entered to verify accuracy. Errors in data entry occurred in less than 0.5% of the entries. Frequencies were run to identify outliers and to reduce the data where appropriate. This was done prior to adding the random treatment group assignment to the dataset. Next, bivariate analyses were run, and crude attributable or relative risks for vomiting or regurgitation with 95% confidence intervals were calculated. These were then adjusted for history of vomiting prior to treatment. Finally, multiple logistic regression models for the prediction of vomiting following initial treatment were tested. Results Over the duration of the study, 1,014 and 1,150 patients were triaged to the NGO clinic and short-stay ward respectively (Fig.). Of these, 936 (92%) clinic and 918 (83%) short-stay ward referrals fit the eligibility criteria, and all consented to participate in the study. As seen, 164 cases of the short-stay ward were eventually transferred to another facility because of co-morbidity. The short-stay ward is a diarrhoea treatment facility, and children with significant co-morbidity are first stabilized and then transferred to the appropriate facility. In each site, enrollment continued until 800 patients were selected for randomization and assigned to one of the three treatment groups (n=534 zinc, n=533 placebo, n= 533 no treatment). We were unable to randomize 118 short-stay ward cases and 136 NGO clinic cases because the child was not settled and, therefore, not randomized by the termination of an observer's shift. Table 1 summarizes the distribution of host and illness characteristics by treatment group. There were nostatistically significant differences between groups. Males were significantly (p<0.001) more likely to be brought to the treatmentcentre. It appeared that vomiting was a major factor affecting the decision to seek help at the centre. Only 10.8% of the subjects reported no history of vomiting during their diarrhoeal illness, and 81.7% reported having vomited in the past 24 hours at the time of triage. Overall, post-treatment vomiting or regurgitation was observed in 15.6% and 5.6% of children respectively. Table 2 summarizes the post-treatment vomiting and regurgitation outcomes by treatment group and further stratifies the vomiting outcomes by vomiting history during illness. In all treatment comparisons, rates of vomiting and regurgitation were higher in those receiving the dispersible zinc tablet formulation. The median duration to the first vomiting episode was 9.6, 9.8, and 13.9 minutes, respectively, in the zinc, placebo and no-treatment groups. Overall, 80% of all post-treatment episodes occurred within 20 minutes. Post-treatment vomiting occurred only once over the 60 minutes of observation in 91.2% of episodes. Table 3 summarizes risk estimates attributable to zinc, based upon a comparison of children receiving the dispersible zinc tab-lets and placebo tablets. Beginning with post-treatment vomiting, overall zinc resulted in a 14% increase in post-treatment vomiting and the numbers needed to treat (NNT: the number of children needed to treat with the zinc tablet to cause one additional episode of vomiting) was 7.1. Com-pared to placebo, the relative risk for vomiting was 2.17 (95% confidence interval [CI] 1.65-2.84) and the proportion of post-treatment vomiting episodes attributable to zinc (etiologic fraction) was 0.60 (95% CI 0.40-0.65). These estimates vary by previous history of vomiting, with the proportion of vomiting attributable to zinc decreasing with more recent pre-treatment vomiting histories (range 0.79-0.41). Regurgitation occurs less frequently, with an attributable risk increase of 5.2%, the NNT being 19.2 and the estimated proportion of regurgitation episodes attributable to zinc being 0.42 (95% CI 0.10-0.63). Table 4 summarizes risk estimates attributable to the dispersible zinc tablet formulation opposed to zinc alone. These estimates are based upon a comparison of children receiving the dispersible zinc tablets with those who received no treatment and, therefore, reflects the combined effect of zinc and other components in the formulation. Beginning with post-treatment vomiting, overall the tablet formulation resulted in a 17.2% increase in post-treatment vomiting and the NNT was 5.8. Com-pared to the no-treatment children, the relative risk was 2.95 (95% CI 2.17-4.02), and the proportion of post-treatment vomiting episodes attributable to the tablets (etiologic fraction) was 0.60 (95% CI 0.40-0.65). These estimates vary by previous history of vomiting, but the proportion of post-treatment vomiting attributable to the zinc tablet formulation was fairly stable across the pre-treatment vomiting strata (range 0.63-0.71). For regurgitation, the absolute risk increase was 7.3.2%, with the NNT being 13.7 and the estimated proportion of regurgitation episodes attributable to the zinc formulation being 0.78 (95% CI 0.58-0.88). Combining the etiologic fraction results in Table 3 and 4, the proportion of post-initial treatment vomiting attributable to zinc, placebo, and the illness episode was 40%, 26%, and 34% respectively. Table 5 summarizes the adjusted odds ratio estimates derived from the testing of a multiple logistic regression model for the prediction of post-treatment vomiting. The resulting equation indicates that both zinc treatment and recent vomiting are important predictors(p<0.001), with dehydration marginally lessening the likelihood of vomiting(p<0.07). Among the latter, those most dehydrated were less likely to vomit. Discussion The scaling up of zinc as a treatment for diarrhoea in zinc-deficient children aged less than five years will require objective guidance from formative and operations research addressing a wide range of issues. Importantly, these include the acceptability of alternative zinc formulations and adherence to treatment instructions. It can be anticipated that both these outcomes will be influenced by the likelihood of side-effects of treatment, even those that are transient and of minimal clinical significance. Randomized clinical trials have been conducted to test zinc efficacy for the treatment of a wide range of adolescent and adult disorders at doses between 50 and 100 mg per day. These include the common cold (18), acne (19), tuberculosis (20), anorexia nervosa (21), and macular degeneration (22). While highly variable in reported frequency, in these trials zinc has been consistently associated with in-creased risks for nausea or vomiting. Whether this is the case with a lower 20 mg dose zinc, but in young children, is, therefore, important to determine and quantify. The results of this study indicate that children who received the dispersible zinc tablet formulation in a dose of 20 mg had about a 14% increased risk of vomiting attributable to zinc following the first treatment dose. This is equivalent to one additional vomiting episode for every seventh child treated. The vomiting does not occur immediately after administration, but about 10 minutes later and is transient in nature, occurring only once in over 90% of children. In addition to zinc, there appears to be two other important predictors of vomiting, this being a recent (less than 3 hours) history of vomiting in association with the illness and better hydration status. Vomiting is a centrally-coordinated neurological reflex (23) that in the case of zinc could be in response to signals from the gastrointestinal tract, excessive sensory stimulation (sight, taste), or toxic blood levels. Local oesophageal or gastric irritation can cause vomiting and regurgitation (24). This explanation is consistent with the timing of vomiting that, on average, occurs about 10 minutes following ingestion. Vomiting in response to a metallic taste would be expected to occur sooner, while toxic zinc blood levels are more likely to lead to a later and repeated occurrences of vomiting. Determining whether or not zinc is associated with nausea or vomiting is particularly problematic in children aged less than five years. Most subjects are not able neither to communicate a sense of nausea nor describe whether this is associated with adverse taste, gastrointestinal irritation, or adversity towards taking a medication. To determine what proportion of vomiting is due to zinc, it must be disaggregated from vomiting due to the illness itself. Children with diarrhoea frequently vomit, and this is even more likely among children whose parents seek help from a health facility. In this study, over 90% of the children enrolled had a history of vomiting during the illness, whereas in a recent community-based study in Dhaka, vomiting was reported in only one-third of the cases (ICDDR,B: national coverage survey, 2004). There is also the placebo effect to consider. A proportion of children will vomit as a response to the ingestion of any medication. Children receiving the placebo tablets also had a significant increase in vomiting. This suggests that the non-zinc components of the dispersible tablet formulation used in this study also contributed to the likelihood of vomiting. There is also the placebo effect to consider. A proportion of children will vomit as a response to the ingestion of any medication. To control for vomiting attributable to the illness or the placebo, two comparison groups were defined: those receiving a placebo and those receiving nothing. Based upon the etiologic fraction estimates comparing the zinc dispersible tablets with placebo and then no treatment, vomiting attributable to the zinc, the non-zinc components (placebo) and the illness in this study population are all important contributors. There are important limitations to this study affecting generalization and clinical interpretation of the findings of the study. The study population were children who were brought to the ICDDR,B hospital, locally known as the 'cholera hospital'. These children are representative of the more severe end of the illness spectrum. While less than one-half presented with signs of dehydration, over 90% had a history of vomiting during the illness and one-half in the three hours prior to presentation. It appears that vomiting is a major factor affecting the decision to seek help at the hospital. Only 11% of the subjects reported no history of vomiting during their diarrhoeal illness, and 82% reported having vomited in the past 24 hours at the time of triage. The absolute increase in vomiting attributable to zinc will likely be significantly less among children treated at home. A second limitation in this study was the short one-hour observation of children. For ethical reasons, it was concluded that children should not be denied zinc treatment; therefore, the decision to restrict the period of time zinc was withheld. This study does not address continued vomiting or vomiting following subsequent doses. The third limitation was that this study used tablets prepared from a single pre-mix shipped from France. It is possible that there are properties unique to this batch that have caused the vomiting. Future studies monitoring side-effects of zinc need to consider alternative treatment protocols. For example, would an initial 10 mg dose given twice during the first day lessen the likelihood of vomiting or regurgitation? Longer-term follow-up is indicated addressing such questions as whether or not vomiting continues to occur with subsequent doses and it continues once the illness subsides. There is also a need to continue to work towards improving zinc formulations that have minimal risk of side-effects. This could include alternative zinc binders, such as zinc acetate. The masking of zinc taste in the tablets is quite effective, but involves a patented technology that does not encapsulate to zinc. This non-encapsulation technique significantly reduces the cost of formulation, but results in direct exposure of the oesophageal mucosa to zinc that can lead to local irritation and vomiting as a consequence. Encapsulated zinc formulations would be better-tolerated; however, lower-cost encapsulation techniques need to be developed. Finally, and most importantly, it needs to be confirmed that any additional risk for vomiting or regurgitation does not result in unacceptable levels of clinically significant adverse outcomes. What are the implications of this study? In terms of anticipatory guidance, health practitioners need to counsel parents about potential, transient side-effects. Operations researchers will need to better understand how these side-effects will influence the success of national scaling-up efforts, both in terms of health providers' prescribing practices and caretakers' willingness to pay or adherence to treatment instructions. It also means that additional efforts are needed to work in partnership with key scale-up gatekeepers, such as national paediatric societies, diarrhoeal disease control programmes, and inter-national or multinational organizations. These constituencies need to be fully informed of the benefits of zinc, which are substantial, and the potential for harm, which at this point appears to be minimal. Acknowledgements This study was supported through the Bill and Melinda Gates Foundation-funded project "Scaling Up Zinc in Bangladesh for the Treatment of Childhood Diarrhea", grant no. 25972. The authors thank Dr. M.A. Salam, Director of the Clinical Sciences Division, ICDDR,B, for his support throughout this trial. The dispersible tablets used in this study were compressed and packaged by Square Pharmaceuticals Ltd., at cost. The authors also thank the research assistants participating in this study, who are largely responsible for the successful integration of zinc treatment into the diarrhoea-management protocol in the hospital. Finally, the authors wish to thank the parents who kindly consented to participate in this study. Conflict of interest: The first author, Charles Palmer Larson, is the principal investigator of the Scaling Up Zinc for Young Children (SUZY) Project. This project has worked with Nutriset, the French company that holds the patent on the dispersible zinc tablet formulation administered in this study. References
© 2005 ICDDR,B: Centre for Health and Population Research |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}