 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
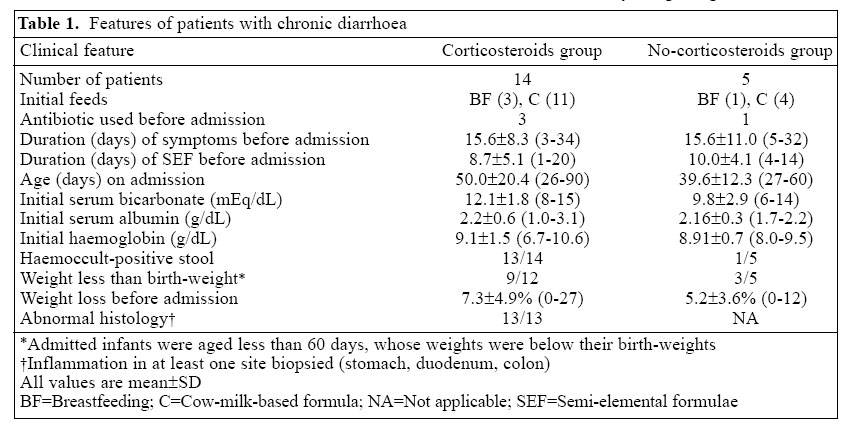
Journal of Health, Population and Nutrition, Vol. ,23 No. 4, December, 2005, pp. 331-338 Corticosteroid-responsive Enteropathy of Infancy Steven N. Lichtman1, Katherine B. Freeman1, and J. Marc Rhoads2 1Department of Pediatrics, School of Medicine, University of North Carolina at Chapel Hill, Chapel Hill, NC 27599-7220, USA and 2Department of Pediatrics, Ochsner Clinic Foundation, New Orleans, LA 70124 Correspondence and reprint requests should be addressed to: Dr. Steven N. Lichtman Department of Pediatric GastroenterologySchool of MedicineUniversity of North Carolina at Chapel Hill5141 Bioinformatics Building, 200 Mason Farm RoadChapel Hill, NC 27599-7220, USA Email: lichtman@med.unc.edu Fax: 919-966-8641 Code Number: hn05044 ABSTRACT Nineteen American infants aged less than three months developed persistent diarrhoea, acidosis, hypoalbuminaemia, and malnutrition, without evidence of enteric pathogens. Symptoms began 11-59 days before admission to the University of North Carolina Children's Hospital, and infants were fed semi-elemental formula. Despite further treatment with amino acid-based formula by continuous nasogastric infusion, diarrhoea persisted. Endoscopic biopsies showed inflammation in the stomach, duodenum, and/or colon. A trial of intravenous corticosteroids was initiated in 14 infants. Corticosteroids were associated with rapid resolution of diarrhoea (duration after corticosteroids=3.8±1.7 days [mean+SD]). In contrast, five infants with identical history were not treated with corticosteroids. In three infants, diarrhoea lasted for 92-147 days versus 31±3 total days in the treated group. In the other two infants, diarrhoea worsened after discharge, but were treated later with corticosteroids, with rapid resolution. Corticosteroids were uneventfully weaned over a four-month period. The results suggest that a trial of corticosteroids in infants with unresponsive persistent diarrhoea of unknown origin is beneficial and deserves prospective evaluation. Key words: Diarrhoea, Chronic; Diarrhoea, Persistent; Diarrhoea, Infantile; Corticosteroids; Acidosis; Hypoalbuminaemia; Retrospective studies; United States Introduction We recently noted the appearance of a condition characterized by chronic diarrhoea, weight loss, hypoalbuminaemia, and acidosis in infants aged less than three months. These were all previously healthy infants with normal feedings who developed acute diarrhoea that became protracted. Many developed severe dehydration, and nearly half of the infants were initially admitted to the intensive care unit at their local hospital. We present 19 infants with protracted diarrhoea and suggest that corticosteroids dramatically corrected the problem in 16 infants who received this treatment. Materials and Methods During 1 January 1999-31 July 2002, 19 infants aged less than three months were admitted to the University of North Carolina Children's Hospital (UNC Hospital) with chronic diarrhoea, weight loss, acidosis, and hypoalbuminaemia. Charts were reviewed retrospectively. Protracted diarrhoea was defined as diarrhoea that persisted for longer than 14 days even after feeding with semi-elemental and amino acid-based formula. All infants had the following laboratory studies: serum electrolytes, calcium, magnesium, phosphate, total protein, albumin, liver enzymes, serum trypsinogen, IgG, IgM, IgA, blood urea nitrogen, and creatinine. Each infant had a sweat chloride test and complete blood count. Eight infants had IgE RAST testing for cow-milk and soy-proteins. Each infant had a barium contrast study of the upper gastrointestinal tract to rule out malrotation, partial obstruction, or stagnant loop. Stools were examined for rotavirus using EIA (Premier Rotaclone, Meridian Bioscience Inc, Cincinnati, OH), Clostridium difficile toxin, ova and parasites, culture and sensitivity, including Escherichia coli O157:H7, white blood cells (WBCs), and haemoccult. Endoscopy of the oesophagus, stomach, and duodenum (EGD) and colonoscopy with biopsies were performed in 13 infants. Twelve patients were tested for HIV. Patients were hospitalized at the UNC Hospital and put on parenteral nutrition and/or continuous nasogastric feeding with Neocate (SHS International, Gaithersburg, MD), an amino acid-based formula. When a decision was made to start corticosteroids, they were initially administered intravenous solumedrol 2 mg/kg per day. As infants responded, they were transitioned to oral prednisone 2 mg/kg per day and eventually slowly weaned over 2-4 months.Weight gain was defined as gaining 20 g per day for at least one week. Resolution of diarrhoea was defined as when stool frequency was less than four formed stools per day, and there was no need for intravenous fluids. Results Description of patients Of the 19 infants identified over a 3.5-year period, 15 were male, and 15 were African-American (12 were African-American male) (Table 1). None was born pre-maturely or with parental consanguinity. Initial feeding included breastmilk in four and cow-milk-based formula in 15 infants. All infants received amino acid-based formula within 24 hours of admission to the UNC Hospital but had not received it earlier. Fourteen infants received treatment with corticosteroids ('corticosteroids' group). Five infants did not receive corticosteroids initially because parents refused treatment ('no-corticosteroids' group).Diarrhoea began 7-73 days after birth and did not respond to 1-20 day(s) of feeding with semi-elemental formulae (SEF, Alimentum, Ross Laboratories, Colum-bus, OH, and Pregestimil, Mead Johnson, Evansville, IL) prior to admission to the UNC Hospital (Table 1). All infants had significant weight loss, hypoalbuminaemia, and acidosis when first admitted to the institution despite prior intravenous fluid treatment at referring hospitals. Six infants were transferred directly to the paediatric intensive care unit at the UNC Hospital, but for other infants, transfer to the UNC Hospital was delayed because they appeared vigorous, well-fed, and well-hydrated clinically. Parents of five infants declined corticosteroid treatment, parenteral nutrition, and endoscopy. They left the hospital without resolution of diarrhoea of their infants. These infants appeared to be stable with respect to hydration, and there was cessation of weight loss at the time of discharge, but they had not gained weight at the UNC Hospital. Two infants returned to the UNC Hospital 16 and 20 days after discharge with further weight loss and severe acidosis. Their parents subsequently accepted corticosteroid treatment, but they did not consent to endoscopy with biopsies. The other three infants were followed every 2-4 weeks and slowly improved (Table 2). The only initial difference between the no-corticosteroids group and the corticosteroids group was that 13 of 14 infants in the corticosteroids group had either visible blood with WBCs (n=9) or WBCs without gross blood (n=5) in stool, but only one of five infants in the no-corticosteroids group had blood or WBCs in stool. On admission, both the groups had a history of significant weight loss despite coming from referral hospitals where they were treated with intravenous hydration and semi-elemental formulae. Twelve of the 17 infants who were admitted before 60 days of age weighed less than their birth-weight. No patients had received parenteral nutrition at the referral hospitals. However, seven of the corticosteroids group received parenteral nutrition at the UNC Hospital. Since they were not improving on amino-acid formula and parenteral nutrition, they underwent endoscopic biopsies 15.2±7.9 days after admission to the UNC Hospital, and corticosteroid treatment was started 16.6±8.8 days after admission. Laboratory findings Despite low levels of serum albumin (Table 1), no infants were oedematous. Serum blood urea nitrogen ranged from 5 to 24 mg/dL, and all patients had a normal serum creatinine. Within 1-3 day(s) after admission to the UNC Hospital, aggressive intravenous rehydration and initiation of amino-acid-based formula by continuous nasogastric feeding resulted in a normal serum bicarbonate in all the infants. No patients had significant peripheral blood eosinophilia. All stool cultures, including those for Salmonella, Yersinia enterocolitica, Shigella, Campylobacter jejuni, and E. coli 0157:H7, rotavirus EIA, tests for ova and parasites, and C. difficile toxin assays were negative at the UNC Hospital. All values of sweat chloride test and all upper gastrointestinal contrast barium studies were normal. All 12 patients tested for HIV were negative. Similar features for the no-corticosteroids group and the corticosteroids group included age on admission, duration of symptoms before admission, duration of feeding with semi-elemental formulae before admission, percentage of weight loss, serum bicarbonate on admission, serum albumin, and haemoglobin concentration (Table 1). Histological findings Endoscopic biopsies were performed of the stomach, duodenum, and colon in 13 infants 2-38 days after ad-mission to the UNC Hospital and prior to corticosteroid therapy (Table 3). At least one site was histologically abnormal in all infants biopsied, but the findings were not pathognomonic of any specific process. The major finding was mild-to-moderate inflammation. In addition, severe duodenal villus blunting was noted in four infants. Five infants had inflammation in all three sites biopsied. Only one patient had tissue eosinophilia which was colonic. The figure, a photomicrograph of a duodenal biopsy, demonstrates villus blunting and monocytic cell infiltra-tion in the lamina propria. There is crypt hyperplasia and focal cryptitis. Response to treatment The corticosteroids group included a subset of seven infants who received parenteral nutrition. The mean duration of admission for infants receiving parenteral nutrition was 24.3±11.0 days. The duration of admission to the UNC Hospital for seven other infants in the corticosteroids group who did not receive parenteral nutrition was13.1±4.0 days (p<0.001).The difference in duration of admission occurred because the infants on parenteral nutrition started corticosteroids after 16.6±8.8 days (10-41 days) compared to those without parenteral nutrition who started corticosteroids only 6.3±3.6 days (2-12 days) after admission(p<0.005). The duration of admission to the UNC Hospital was not significantly different for infants in the no-corticosteroids group (12.2±2.7 days) compared to infants treated with corticosteroids who did not receive parenteral nutrition (13.1±4.0 days). However, diarrhoea had not resolved when the infants in the no-corticosteroids group were discharged, but diarrhoea was totally resolved in the corticosteroids group when discharged. Table 4 compares the recovery rates of the cortico-steroids and no-corticosteroids groups. The patients in the corticosteroids group had symptoms for 3-34 days before admission. They received semi-elemental formulae for 1-20 day(s) prior to admission to the UNC Hospital and then amino-acid-based formula for further 2-41 days after admission, when corticosteroids were started. Therefore, the patients in the corticosteroid group received semi-elemental formulae plus amino-acid-based formula for 15-48 days prior to starting corticosteroids which was 17-59 days after symptoms began. Stool frequency and consistency became normal 2-8 days (3.8±1.7 days, mean±SD) after corticosteroids were initiated. Weight gain of more than 20 g per day began 3-15 days after corticosteroids were initiated. Se-rum albumin increased to greater than 3.5 g/dL 3-30 days after treatment with corticosteroids. Therefore, for the corticosteroids group, the total duration of diarrhoea, time for weight gain, and normalization of albumin from the initial onset of symptoms were 31±11, 32±11, and 39±14 days (mean±SD) respectively. In contrast, three infants were never treated with corticosteroids, and their loose stools and hypoalbuminaemia were normalized 92-141 days after onset of symptoms (Table 2). Consistent weight gain was not observed until 55-95 days after discharge from hospital. The three patients in the no-corticosteroids group required three times longer to normalize stool pattern and gain weight and albumin compared to the corticosteroids group. Parents of two patients initially refused corticosteroid treatment. Their infants subsequently returned to hospital with further weight loss, acidosis, and severe diarrhoea 16 and 20 days after discharge. These infants responded with cessation of diarrhoea after three and four days of corticosteroid treatment and normalization of serum bicarbonate within 48 hours and albumin within seven days (Table 2). Once initial severe diarrhoea was stabilized, all infants were exclusively fed amino-acid-based formula for at least four months but none required amino-acid-based formula or semi-elemental formulae after eight months. None of these infants relapsed after corticosteroids were discontinued. After eight months, all infants tolerated normal diets without feeding amino-acid-based formula or semi-elemental formulae. The duration of follow-up has been 2-5 years without relapse in diarrhoea, weight loss, or acidosis, and all children are taking a normal diet. Discussion This paper presents a series of infants with protracted diarrhoea, weight loss, hypoalbuminaemia, and acidosis. The infants had histological evidence of inflammation, but it was not consistent in site or severity. Patchy intestinal lesions that did not predict outcome have been described in cases of protracted diarrhoea in infancy (1). We confirmed this finding in our study. After treatment with amino-acid formula and corticosteroids, but not with amino-acid-based formula alone, all infants improved dramatically, and none required long-term amino-acid-based formula or semi-elemental formulae or corticosteroids. Ten patients presented to the referral hospital with severe dehydration but responded quickly to intra-venous fluids. Subsequently, they consumed adequate volumes of semi-elemental formulae and looked well-hydrated but developed significant acidosis, low albumin, and further weight loss at local hospital. Most referral physicians treating these infants did not recognize the severity of their illness until serum bicarbonate and albumin were checked. Results of a previous study showed that clinical assessment of hydration in small infants was difficult (2). Management protocols have been devised by investigators in countries where diarrhoea is a major cause of infant mortality (3,4). These protocols include oral rehydration; antibiotic therapy as indicated; and administration of locally-available cereals, vegetable oil, minerals, animal milk, and yogurt. For those who fail to respond, the diet is changed to cereals plus lactose-free carbohydrates (4). In developed countries, algorithms have not been developed, but many administer protein hydrolysate formulae that are less allergenic than cow-milk-based formulae, often by continuous feeding, which reduces diarrhoea and improves absorption (5). In severe cases, infants are administered amino acid-based formula with or without parenteral nutrition (6). Although chronic diarrhoea in developed countries may be perceived as a self-limiting illness, this series demonstrates that the illness can be very severe, resulting in acidosis (100%), weight loss (100%), and severe dehydration (48%). The major finding of this study is that 14 infants (corticoisteroids group) with severe diarrhoea for 17-59 days dramatically improved within 2-8 days of treatment with corticosteroids. The three infants who never received corticosteroids eventually recovered with a total duration of symptoms three times longer than the corticosteroids group. The differential diagnosis includes formula protein allergy. However, none had peripheral blood eosinophilia, and only one patient had eosinophilic infiltration that was found in the colon. None had other manifestations of allergy, such as eczema or wheezing. In this study, eight infants were tested for allergy to cow-milk and soy-proteins using RAST IgE, and all had negative results. All patients received semi-elemental formulae for 1-20 day(s) before admission to the UNC Hospital but did not benefit, with persistence of diarrhoea, low serum albumin, and weight loss. Infants then received amino-acid-based formula for another 2-41 days, still without any improvement. All infants were being fed a normal diet from eight months of age without any relapse. None of these features is consistent with formula protein allergy. Seven patients in the corticosteroids group received parenteral nutrition, and the length of their admissions was 24±11 days compared to the other seven patients in the corticosteroids group whose duration of admissions was only 13±4 days(p<0.001). This difference was not due to allocation of more serious patients in the parenteral nutrition group but was due to the time at which corticosteroids were started. In those infants with parenteral nutrition, corticosteroids were started 17±9 days after admission, whereas for infants who did not receive parenteral nutrition, corticosteroids were started 6±4 days after admission. Our original treatment protocol for infants with diarrhoea included placement of a central venous catheter and administration of parenteral nutrition, but as we became more confident with the use of corticosteroids, this treatment was initiated earlier, and infants improved so that parenteral nutrition was unnecessary. We propose that the use of parenteral nutrition and its complications may be avoided by early diagnosis by endoscopic biopsy and treatment with corticosteroids. It is unlikely that what we are calling corticosteroid-responsive enteropathy of infancy represents a true auto-immune enteropathy because only four (27%) of 15 biopsied patients had severe intestinal villus atropy. Furthermore, no patients relapsed when corticosteroids were withdrawn (7). However, tests for anti-enterocyte antibodies were not performed. It is unlikely that these infants had such congenital diarrhoeas as tufting enteropathy, microvillus inclusion disease, glucose-galactose malabsorption, or congenital disaccharidase deficiencies because these entities do not respond to corticosteroid therapy and are not self-limiting. During a three-year study, Catassi and colleagues re-ported 32 cases of protracted diarrhoea, of which seven patients died (8). Age of onset was less than three months in 19 cases. Their study included patients with auto-immune enteropathy (n=8), ultrastructural abnormalities of the enterocyte (n=7), multiple food intolerances (n=3), post-enteritis syndrome (n=2), and others. Nine children recovered, but their course of treatment and diagnoses were not described. Twelve patients were given corticosteroids, but the effect of this treatment was not discussed. Some cases in their population may have had a syndrome similar to those described in this study. Furthermore, our patients may have had Type 1 intractable diarrhoea as described by Goulet and co-workers (9). Their patients had villus atrophy, inflammation of lamina propria and intestinal auto-antibodies. They were not syndromic, as were most patients in Type II that included tufting enteropathy. Fifty-five percent of patients described by Goulet and co-workers died (9). Corticosteroids were used in their patients without success. All patients in the present study had stool cultures, tests for ova and parasites, C. difficile toxin assay, and rotavirus EIA studies which demonstrated no active infection at the time of admission. Of the 18 infants tested for these stool pathogens at referral hospital, only one had a positive rotavirus EIA. This condition could represent a form of postinfectious enteropathy (10) because either stool studies were inadequate or were poorly timed. Our patients may fit the description of Avery and colleagues of "chronic protracted diarrhea of infancy" (11). This non-specific term may represent a variety of different conditions. Ours is the first report showing the beneficial use of corticosteroids in protracted diarrhoea in infancy. A major limitation to the study is that it is retrospective with no prospectively-designated control group. The no-corticosteroids group served as an age-matched control group that demonstrated eventual resolution of symptoms over 88-141 days in the absence of corticosteroids (n=3). In addition, two patients who did not receive corticosteroids initially later returned to hospital because of worsening diarrhoea and weight loss. They subsequently responded dramatically to corticosteroids within 4-6 days. There are several reasons why corticosteroids may have been beneficial for these infants. Corticosteroids have powerful effects on intestinal absorption and digestive enzymes that could be beneficial for patients with enterocolitis. Na+ transport in the colon and small intestine is stimulated, secondary to increases in mucosal Na,K-ATPase activity, increases in colonic apical Na+ channels, and reduced inflammation (12). In neonates, corticosteroids stimulate rapid developmental changes in mucosal disaccharidase activities (13) and absorption of glucose-coupled Na+ (14). Even in rotavirus-infected piglets, treatment with corticosteroids did not prolong illness or viral excretion; instead, treatment with corticosteroids promoted early regeneration of the absorptive surface and absorption of glucose-coupled Na+ (15). In addition, corticosteroids generally decrease inflammation and inhibit cytokine release from inflammatory cells. A key lesson from these cases is that it is important to monitor serum bicarbonate and albumin in infants with diarrhoea and poor weight gain, even if they look 'clinically well'. We recommend the following plan for infants aged less than three months, who present with protracted diarrhoea and with either low albumin or low bi-carbonate. These infants should be referred to a tertiary-care centre with paediatric gastroenterological services. Continuous nasogastric feeds with amino-acid-based formula should be started, and a thorough search for infectious agents performed. Early endoscopic biopsies should be obtained and, if inflammation is present in either the stomach, duodenum, or colon, a trial of corticosteroids should be implemented. All the infants in this study responded to corticosteroids within eight days. If an infant has not responded within eight days, we recommend that corticosteroids be weaned. If there is a significant response, treatment with 2 mg/kg per day should be continued for 4-8 weeks, followed by slow weaning. Our results suggest that treatment with amino-acid-based formula and corticosteroids hastens the resolution of prolonged neonatal enteropathy with acidosis, reducing the need for parenteral nutrition. However, close observation and supportive care may also result in resolution of this condition over an extended time. A double-blind prospective study is warranted to confirm these findings. Acknowledgements The authors acknowledge paediatric inpatient and ICU nursing staff (headed by Dr. Melanie Edwards), Dr. John Woosley, Pathology Department, and Dr. Angela Maynor, Registered Dietician, for helping with the management of the patients. References
© 2005 ICDDR,B: Centre for Health and Population Research |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}