 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. ,23 No. 4, December, 2005, pp. 377-387 Effectiveness of Depot-holders Introduced in Urban Areas: Evidence from a Pilot in Bangladesh GAZI, Dr. Rukhsana; Alec Mercer; Jahanara Khatun; Ziaul Islam; Health Systems and Infectious Diseases Division ICDDR,B: Centre for Health and Population Research GPO Box 128, Dhaka 1000, Bangladesh Correspondence and reprint requests should be addressed to: Dr. Rukhsana Gazi Health Systems and Infectious Diseases Division ICDDR,B: Centre for Health and Population Research GPO Box 128, Dhaka 1000 BangladeshEmail: rukhsana@icddrb.orgCode Number: hn05050 ABSTRACT Depot-holders are women from the community who promote good health practice and use of clinics. They keep a stock of contraceptives and oral rehydration salts to supply other women and are paid some incentives. In 2003, the NGO Service Delivery Program (NSDP) introduced depot-holders in three types of urban area in Bangladesh as a pilot. This evaluation study was carried out to: (a) establish a baseline for measuring the impact of activities of depot-holders on a comprehensive range of indicators in the long-term, (b) make a preliminary assessment of the impact on the use of selected services of the essenial services package (ESP) and other indicators at the end of the pilot phase, and (c) assess the cost of introducing depot-holders and running their activities for a year. Data from the baseline and end of pilot household surveys, together with service statistics from the intervention and comparison areas, were used for assessing the changes in clinic use and commodity distribution. The study found evidence that the depot-holders transferred knowledge to women in the community, provided services, and referred women to clinics run by non-governmental organizations (NGOs). There was a large increase in the number of client contacts at the NGO clinics and in the quantity of oral contraceptive pills and oral rehydration salts distributed by the NGOs, mostly attributable to the activities of the depot-holders. The estimated cost per depot-holder per year was Tk 15,241 (US$ 262). Overall, the performance of the depot-holders in the pilot phase suggests that they can be introduced in different types of urban area and can be effective in their dual role as providers and promoters of services. Key words: Health services; Cost analysis; Depot-holders; Community-based distribution; Family planning; Essential services package; Evaluation studies; Urban; NGOs; Bangladesh Introduction Community-based volunteers, and local women, who are paid a small financial incentive, have been used in many parts of the world. In the 1990s, female community volunteers were introduced by the governments to improve access to family-planning services in rural areas of Nepal (1) and in a pilot programme in Bangladesh (2). They have been used for improving access to oral rehydration salts (ORS) in Peru (3) and for the distribution of iron and folic acid tablets in India (4). They were effective for increasing access to postpartum care in Colombia (5) and for community-based tuberculosis, malaria and filiariasis programmes in different countries (6-11). Volunteers have also been used in urban areas, for example in Lagos, Nigeria, for promotional, curative and preventive primary healthcare activities (12). In Bangladesh, 'depot-holders' have been used for improving access to family-planning services in rural areas. These are women from the community, who keep a stock of commodities (contraceptive pills, condoms, ORS) in their home to supply other women, and promote good health practice and use of clinics. They are not strictly volunteers, since they receive some financial incentives. The Government introduced them in 64 sub-districts (upazilas) in the 1990s (13). The Rural Service Delivery Partnership (RSDP), a non-governmental programme, provided health services in rural areas from 1997, with depot-holders working at village level promoting the use of satellite and static clinic services. The programme served over 11 million people each year and employed over 6,000 depot-holders throughout the country (14). In 2002, it became part of the NGO Service Delivery Program (NSDP) which provides most services of the Government's essential services package (ESP) in certain rural and urban areas through 41 local partner NGOs. The ESP covers five types of services: reproductive health and family planning, child health, control of communicable diseases, limited curative care, and behaviour change communication. A major aim of service delivery of the ESP is convenience and accessibility for women, children, and the poor. The Health and Population Sector Programme (HPSP) 1998-2003 of the Government focused on improving access for the poor to the ESP, but only in rural areas. The urban poor are particularly deprived in terms of child healthcare services, and studies have reported high prevalence of diarrhoeal diseases and acute respiratory infection (ARI) among children, low use of oral rehydration therapy (ORT) and immunization, and high infant mortality (15,16). Many parts of towns and cities in Bangladesh lack government health-care facilities and outreach services, and NGO clinics provide most services. Results of studies in Dhaka in the early 1990s showed that female community volunteers improved access to health facilities and ORT, particularly in areas served by NGO clinics, and mothers found their services to be useful (17). Based on these findings, the NSDP introduced depot-holders in three urban areas in 2003 as a pilot aimed at improving access to the ESP, particularly among the poor. ICDDR,B: Centre for Health and Population Research worked with the NSDP to design a study to: (a) establish a baseline at the beginning of the pilot intervention for measuring the impact of activities of depot-holders on a comprehensive range of indicators of the use of health and family-planning services in the long-term, (b) monitor the activities of depot-holders and use of services and conduct a follow-up at the end of a pilot phase to make a preliminary assessment of the impact of the activities of depot-holders on the use of selected ESP services and other indicators, and (c) ascertain the cost of introducing depot-holders and running their activities for a year as a basis for a longer-term assessment of cost-effectiveness in the future. Materials and Methods
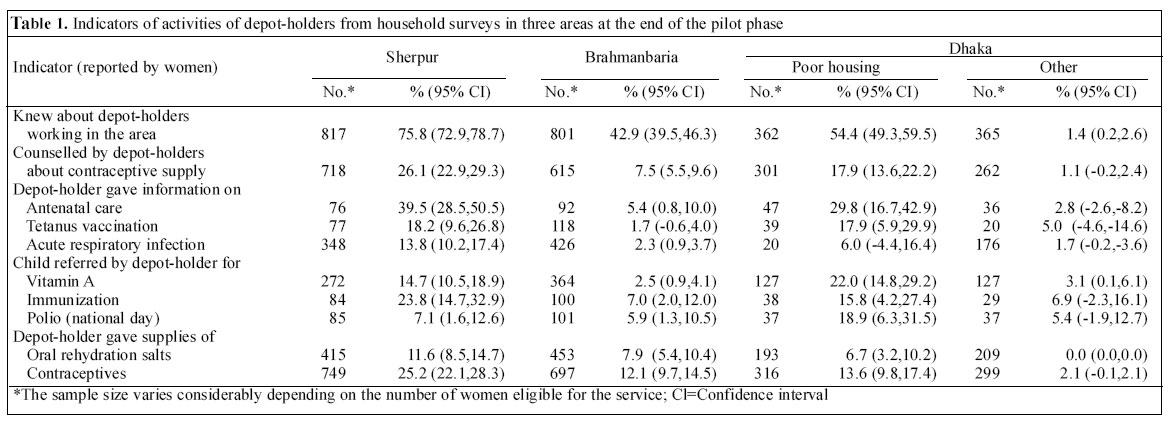
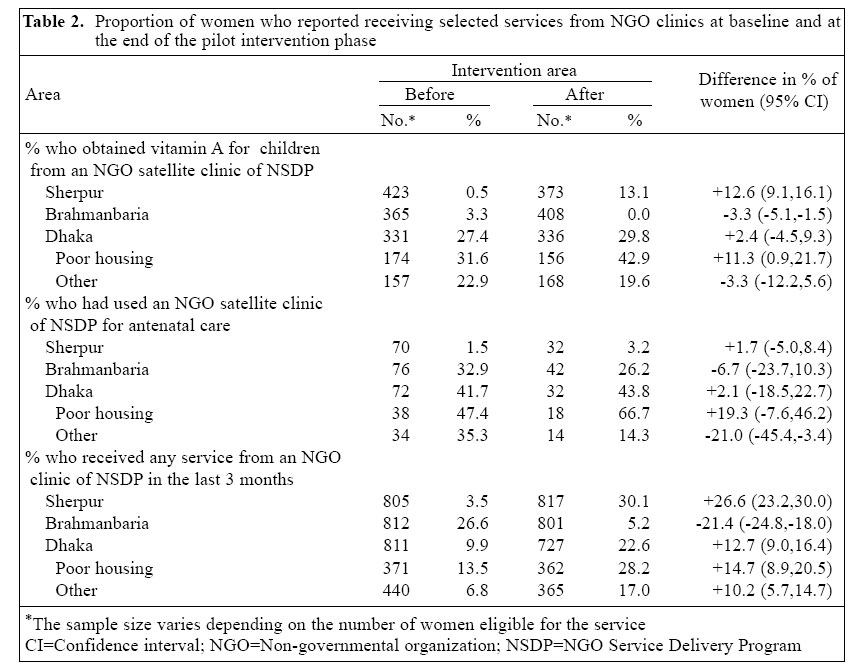
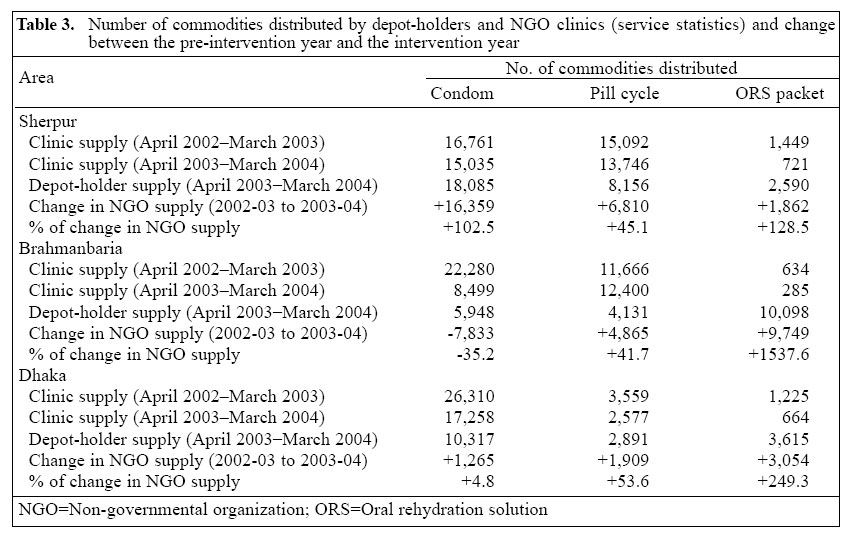
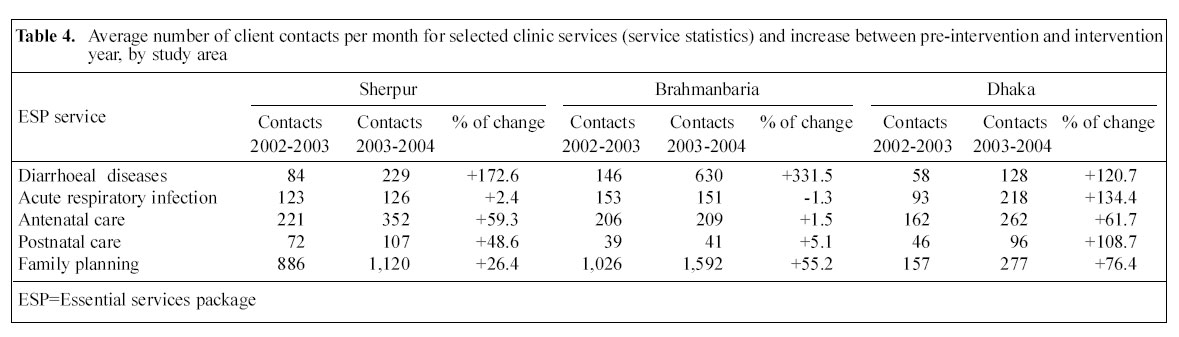
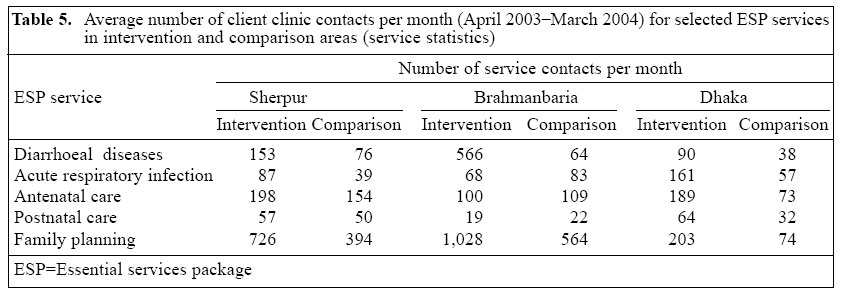
Study design The study design for this preliminary assessment of the impact of depot-holders was based on measurement of selected indicators before and after the pilot intervention period in the intervention and non-intervention (comparison) areas. For the intervention areas, three NSDP partner NGOs each selected 20 women from the community, who were trained for six days and allocated a group of households around a satellite clinic (350-450 couples eligible for family planning). They were paid an honorarium of Tk 200-500 per month (US$ 4-8), a commission of 50% of profits from the sale of commodities, and 50% of service charge for customers they referred to the NGO clinics. The existing NGO staff (community health promoters) working in the three areas supervised them. Study areas and population The study was conducted in three types of urban area: municipal type A-city corporation (Rayer Bazar in Dhaka city); type B-district town (Brahmanbaria in Chittagong division); and type C-upazila (sub-district) (Sherpur in Dhaka division). The NSDP selected the study areas, which had ESP almost exclusively provided by their partner NGOs. The district-level government hospital was 8-12 km away, although, in Dhaka, a private medical college hospital was located near the study area. The partner NGOs decided which half of the study area would have depot-holders and which would be the comparison area (demarcated by ward, village [para/ moholla] and/or natural boundaries, such as major roads). The intervention and comparison areas were intended to have approximately the same size of population, and the number of satellite clinics was similar in the three areas. An NGO static clinic was located in each of the intervention areas, although it served the whole study area. The study population included all married women of reproductive age (15-49 years) and their children aged less than five years, particularly those covered by the activities of depot-holders. The NGOs estimated that there were about 15,000 such women in the Sherpur and Brahmanbaria study areas and 25,000 in Dhaka. Sampling Interviewers conducted an initial enumeration of married women of 15-49 years to provide the sampling frame. In Brahmanbaria and Sherpur, married women in about 350-450 households around each satellite clinic (depot-holder catchment area) were listed. An equal number of married women were selected at random from each of the satellite clinic lists using the appropriate sampling fraction to obtain a sample of 800 in each area. For the survey in Dhaka, sampling was stratified to allow an assessment of the impact on some indicators (e.g. use of NGO clinics) among a lower socioeconomic group. A sample of 400 women was selected in each intervention and comparison area from those identified in the list as living in 'poor housing' and 400 from those in other housing. Dwellings that had any three of the following characteristics were classified as 'poor housing': jhupri (bamboo walls/roof), kancha (mud-walls), dilapidated condition, or under construction (people living in a building site). People in poor housing also shared latrines and a communal water source. There were five main sources of data: (a) cross-sectional household surveys of married women aged 15-49 years using a structured questionnaire, (b) cross-sectional surveys of depot-holders using a structured questionnaire, (c) service statistics from the NGO management information system (MIS) and depot-holder registers, (d) in-depth interviews with women conducted before and in the eighth month of the pilot phase to ascertain their views on services of depot-holders; and in-depth interviews with a sub-sample of 10 purposively-selected depot-holders (representing age and marital status groups) and 10 NGO staff (managers, service providers, and supervisors); and (e) a focus-group discussion with 10 depot-holders in each area half way through the pilot phase to gather information on their experience, which was used for development of activities. Preliminary activities began in February 2003; the baseline household survey was conducted in June-July 2003; and the endline survey was conducted in March 2004. Although the service statistics for the intervention and comparison areas were collected in the year of the pilot phase (April 2003_March 2004), data were not available for the separate areas for the previous year. However, it was possible to assess the changes in ser-vice use for the intervention and comparison areas combined since the previous year (April 2002_March 2003) when no depot-holders were working. For the intervention year, data on the use of services in the intervention and comparison areas were compared. Data from the household survey in the comparison areas were not used for this assessment of impact in the pilot phase, although these will be used for a longer-term assessment of intervention-related changes in indicators (the change in the intervention area minus the change in the comparison area). Study indicators Cost analysis To determine the additional programme costs of the intervention, data from the NGO and NSDP central offices were used (clinic-records and service statistics). All additional resources used for implementing the intervention were identified, quantified, and valued following the ingredients approach. The total cost was calculated by multiplying the quantity of individual inputs by the corresponding price and summing. Average cost per depot-holder (i.e. unit cost) was calculated by dividing the total cost by the number of depot-holders. Inputs used in the intervention were categorized to assess capital and recurrent costs. Inputs that had a useful lifetime of one year or more were considered capital inputs (e.g. signboard, trunk, umbrella, bag, logo, and training and recruitment). For estimating the annual cost of capital items, current market price, useful lifetime, and a 5% discount rate were applied. The annualization factors were taken from a standard table, and the annual value was calculated by dividing the current price by the appropriate factor. Inputs purchased or provided regularly by the intervention clinics and used up during the course of the intervention were considered recurrent. The corresponding costs were calculated, including apportioned staff costs for supervision and meetings, monthly honorarium of depot-holders, and contraceptive supplies (market price). The costs for the staff of the intervention clinics, who conducted the recruitment process and who organized the training of depot-holders, were apportioned, based on the estimated time spent. Results Sociodemographic characteristics of women in depot-holder areas There was a considerable variation in the composition of samples of women interviewed in the communities, although this is unlikely to affect the assessment of activities of depot-holders. About two-thirds of women interviewed in the baseline and endline surveys were aged 15-34 years, and others were aged 35-49 years. The educational level was relatively high among women in Dhaka compared to those of other areas: the proportion with no formal education ranged from 12% in the comparison area of Dhaka (post-intervention survey) to 64% in the comparison area of Sherpur (post-intervention). About 3-11% of women had no children, and 30-60% had 1-2 living child(ren). About 30-60% had an average length of residency of more than 10 years. Most (81-97%) respondents were housewives, although 11-51% were involved in credit programmes run by the NGOs. Most (69-93%) women in Sherpur and Brahmanbaria resided in their own house, while 75-86% in Dhaka reported living in rented accommodation. 40-84% of women reported an average monthly family income of less than Tk 5,000 (< US$ 85), and the income was generally higher in Dhaka than in other areas. Evidence of activities of depot-holders from household surveys of women The household surveys showed evidence of the activities of depot-holders (Table 1). The proportion of women who knew about depot-holders working in their area was the highest in Sherpur (75.8%) and among women in the poor housing group in Dhaka (54.4%). The proportion of women who had had counselling from a depot-holder about family planning, had received information on antenatal care, tetanus toxoid (TT) vaccination, and ARI, had been referred to a satellite clinic for child immunization, or supplied with ORS and contraceptives, was also the highest in Sherpur (10-40%). There was evidence of the effectiveness of the promotional activities of depot-holders (Table 2). There were statistically significant increases in the proportion of women who reported that they had obtained vitamin A for their children from an NGO satellite clinic in the last three months in Sherpur (from 0.5% to 13.1%) and among women with poor housing in Dhaka (from 31.6% to 42.9%). The proportion of women who received any service from an NSDP satellite or static clinic in the last three months also increased significantly in Sherpur (from 3.5% to 30.1%) and in Dhaka (from 9.9% to 22.6%), and the proportion of women who reported receiving antenatal services at an NSDP clinic increased significantly among poor women in Dhaka (from 47.4% to 66.7%). Commodities distributed by depot-holders and NGO clinics Review of service statistics showed that there were in-creases in the quantity of commodities supplied by the NGOs in the year of the pilot intervention (2003-2004) compared to the pre-intervention years (2002-2003) (Table 3). In Sherpur, there was a considerable increase in the total quantity of condoms (97.6%), pill cycles (45.1%), and ORS packets (128.5%) distributed by the NGOs. There was a large increase in the distribution of pill cycles (41%) and ORS packets (1538%) in Brahmanbaria and in Dhaka (53.6% and 249.3%). In all cases, a decrease in clinic supply was more than offset by the new distribution by the depot-holders, whose distribution ac-counted for a high proportion of the commodities supplied by the NGOs in 2003-2004, despite depot-holders working only for part of the year. The proportions of condoms, pill cycles, and ORS packets distributed by the depot-holders in the intervention years were 55%, 37%, and 22% respectively in Sherpur; 41%, 25%, and 97% in Brahmanbaria, and 37%, 53%, and 84% in Dhaka. Use of NGO clinic services Between the pre-intervention year and the intervention year, there was an increase in the average number of clinic contacts per month for each of the selected services in Sherpur and Dhaka and for diarrhoeal diseases and family planning in Brahmanbaria (Table 4). These data are for the intervention and comparison areas combined, as separate data were not collected during the pre-intervention year. The number of contacts more than doubled for diarrhoeal diseases in all the three areas and for ARI and postnatal care in Dhaka. There was an increase in the number of contacts for family-planning services at the NGO clinics in Dhaka (76%), Brahmanbaria (55%), and Sherpur (26%), in addition to the increase in contraceptive distribution by the depot-holders themselves. For the intervention year, separate data on clinic contacts were collected for the intervention and comparison areas (Table 5). In Dhaka, the monthly average number of contacts for each type of service was about 2-3 times higher in the intervention area than in the comparison area. In the Sherpur intervention area, the monthly average for some services (diarrhoeal diseases, ARI, and family planning) was about double that in the comparison area. In Brahmanbaria, it was almost 10 times higher in the intervention clinics, and the number of contacts for family planning was 82.3% higher than in the comparison clinics. Findings on other aspects of the activities of depot-holders Interaction of depot-holders with the communityTo perform their activities effectively, depot-holders re-quire the support of their families and of the community in general. They did not report any problems in managing their housework, and most (over 80%) reported sup-port from their family for their work. In the preliminary stages, the NGOs had to inform local landlords, ward commissioners, members of different clubs, and local leaders about their activities and to overcome problems with local gangsters (mastans) demanding extortion money (chanda). Most depot-holders reported covering about 300-500 eligible couples, spending 3-4 hours per day visiting 20-30 households. They provided services mainly to women and children from poor and some middle-income households. Most depot-holders in Dhaka repored that women from 'rich' families were not interested in receiving their services, and some had difficulty in gaining access to apartment buildings where the better-off lived. However, in general, the depot-holders reported that most people in the community welcomed their activities, and this was confirmed by in-depth interviews with women. Women in the community reported that the depot-holders were generally valued for being from the community, building good relations, being available most of the time for counselling, and for referring women to clinics and accompanying them, if necessary. Women who used their services valued their accessibility and lack of transportation costs, and knew the main services provided at the NGO clinics. On the other hand, non-users were not aware of the activities of depot-holders or the availability of the range of NGO services. Many women considered the NGO clinic services to be expensive, and some very poor women went outside the area to other NGO facilities that charged less or nothing. Some better-off women preferred private clinics, or service providers with a health card scheme, qualified doctors and pathological tests, and they bought their contraceptives from a pharmacy. Income and incentives of depot-holders As most depot-holders were from very low-income households, incentives could be an important factor for sustainability of their services. Most (> 80%) depot-holders reported an average monthly household income of less than Tk 3,000 ( < US$ 86), while the monthly income from their depot-holder activities was about Tk 700 (US$ 12) at endline. This included an honorarium of Tk 300-400, Tk 50 for transport, and money from sales and referrals. Many depot-holders considered the earnings too small, and two dropped out for this reason. Some reported that they were embarrassed that their earnings were lower than for housemaids and suggested that Tk 1,000-1,200 would be more acceptable. Some depot-holders also requested identity cards, clothes, and free treatment for themselves and for their family members. Many wanted to provide more services, which would give them more income (e.g. iron tablets, vitamin A capsules, other brands of contraceptive, and some basic medicines, such as paracetamol, antacid, and medicine for cough). Others wanted training to record blood pressure and temperature and to provide injectable contraceptives. Job satisfaction and drop-out of depot-holders Despite the low earnings, most depot-holders interviewed in depth liked the work, wanted to continue, and to have more responsibilities. They expressed pride in providing a formal service for people's benefit, which also brought them social benefits, such as scope to talk with many people, to learn new things, and become well-known and respected in the community. Several depot-holders-two in Brahmanbaria, three in Sherpur, and about half (10 of 20) in Dhaka-dropped out mainly because of another job, marriage, out-migration, sickness, and a greater volume of work than expected. The NGOs terminated four depot-holders because of their unsatisfactory performance. Supervision of depot-holders Retention and satisfactory performance of depot-holders may also depend on the quality of supervision.Most(>80%) depot-holders were satisfied with the frequency and quality of support from their supervisors, with whom they met twice a week, at the satellite clinic and at the depot-holder's house. They also attended monthly meetings at the NGO office to discuss activities, problems, distribution of commodities, work schedules, and particular services. However, no depot-holders used written workplans for visiting clients, and they rarely updated their registers. Some NGO staff members mentioned the need for more supervision and performance review, including spot-checks, more official meetings, and formal evaluations. The supervisors generally valued the depot-holders as they knew the locality and could motivate people to use the NGO services. They recognized that, as a result of the activities of depot-holders, the number of users had increased in the intervention year. Cost of introducing depot-holders An important programmatic consideration (if the depot-holder programme is to be scaled up) is the cost of introducing and sustaining their activities. The main capital costs of the intervention were for materials (Tk 40,081) and for training and recruitment (Tk 100,138). The total recurrent cost (Tk 804,726) was mainly for supplies (47.5%), honorarium (31.2%), and supervision (16.6%). The total additional cost of the deport-holder intervention for one year was estimated to be Tk 944,945 (US$ 16,292), an average cost per depot-holder per year of Tk 15,241 (US$ 262). The total revenue generated by the depot-holders from selling contraceptives and ORS packets and through service-fees for referred clients was Tk 210,824 (US$ 3,635). It is difficult to calculate cost-recovery as, to some extent, services of depot-holders replaced those provided by the clinics, which tended to reduce the cost-recovery of clinics. An additional profit of about Tk 50,000 (US$ 862) was generated for the NGO clinics and a similar amount for the depot-holders themselves, after deducting the related costs. Discussion
This study, as a pilot to introduce depot-holders in urban Bangladesh, found evidence of effective activities in all the three areas. In the endline household survey, a higher proportion of women was aware of the depot-holders, and they were identified as a source of information on ARI, antenatal care, and vaccination of tetanus toxoid. A reasonably high proportion of women had received services from the depot-holders, such as supplies of ORS, pills, or condoms, and many reported that their children were referred to the NGO clinics for vaccination and vitamin A. In general, there was improved knowledge among women in the community about the NGO services, increased use of satellite clinics, and an increase in the amount of commodities supplied by the NGOs. The service statistics indicate a much higher number of client contacts for key ESP services in the intervention year than in the pre-intervention year. It is difficult to quantify how much of this was directly attributable to the activities of depot-holders as no separate data were available for the intervention and comparison areas for the pre-intervention year. In the intervention year, there were considerably more contacts for antenatal and family-planning services in the intervention areas than in the comparison areas, although this may partly reflect the location of the static clinics in the intervention areas. The increases in contacts for diarrhoeal diseases in all the three study areas, and the increase for ARI in Dhaka, could also partly reflect changes in morbidity. However, the large overall increase in client contacts for reproductive health services at the NGO clinics in the study areas suggests an impact of the promotional activities of depot-holders. There is stronger evidence of direct impact in terms of increases in all the three study areas in the total quantity of ORS packets and pills distributed and of condoms in Sherpur and Dhaka. In all cases, a decline in distribution by the clinics was more than offset by the new distribution by the depot-holders them-selves. There were differences in indicators of the effectiveness of depot-holders among the three areas, with generally better performance in Sherpur and Dhaka than in Brahmanbaria, which could reflect the character of the areas and programmatic factors. Most people of Sherpur upazila actually live in rural villages. The relatively good performance there may reflect the experience of the NSDP with depot-holder services in rural areas and strong organizational capacity and commitment of the NGO staff to support the activities of depot-holders. On the other hand, the study area in Dhaka was very different, being an inner city area with slums, security problems, and a more socioeconomically-heterogeneous population. Most performance indicators relating to women living in poor housing were almost as good as in Sherpur, despite the high drop-out of depot-holders. One advantage for the depot-holders in Dhaka was that their areas were densely populated. They were able to visit households without walking a great distance, which was a constraint in Brahmanbaria where households were very spread out. In Brahmanbaria, several factors may have contributed to a weaker impact on some indicators. The working areas were not equally distributed among the depot-holders, and three depot-holders who were replaced did not receive the six-day training. In the intervention areas, the number of monthly sessions held in the satellite clinics was lower than that in the comparison areas, reflecting staffing problems. One of the two paramedics was on leave for three months with no replacement, and the medical doctor at the static clinic was absent for two months in the pilot phase. Brahmanbaria is also considered to be more culturally conservative, and some women found it difficult to discuss family planning. Restrictions on movement of women could also affect their ability to visit a depot-holder's house or comply with referral to a clinic. Despite these factors, there was a considerable increase in the total distribution of pills and ORS packets as a result of depot-holder provision, and a large increase (55%) in the number of client contacts for family planning at the NGO clinics. Socioeconomic composition of the population in the study areas could also affect some indicators of the performance of depot-holders. Generally, better-off people were not interested in receiving their services, particularly in Dhaka. Consequently, much of the impact of depot-holders in Dhaka was among women living in poor housing. On the other hand, some very poor women were also unwilling to use the services of depot-holders, as they could get the same services free or at low cost from other NGOs, or by going to the government facilities in another area. Social factors may also affect communication, and depot-holders of a lower educational level may be preferable for working in slum areas to reduce social distance and facilitate communication with service-users. In other countries, community volunteers have been valued in different settings as health agents who can break down sociocultural barriers between the formal healthcare system and the community (18). However, this requires effective communication skills, and specific training may be needed for this in Bangladesh. Retention was clearly more of a problem in Dhaka, which probably reflects more alternative work opportunities (albeit very low-paid) compared to the other two areas and also greater involvement of people in the cash economy. Commitment is also likely to be important, and it has been associated with good performance of volunteer family-planning workers in other countries (19). Although most depot-holders liked their work, which gave them new knowledge and social status, a few had not anticipated the amount of work involved. Clearly, adequacy of incentives, commitment, and socioeconomic status need to be taken into account in recruitment and training. Greater financial and other benefits may be required to avoid high drop-out, particularly in a large city, such as Dhaka. Further training and new skills would enable depot-holders to supply more commodities and services, which could contribute to generation of greater revenues and hence sustainability of the programme. Extending their activities would have workload implications for other NGO staff, and some supervisors already mentioned the extra work involved. Nevertheless, to be effective and provide quality services, depot-holders will require good supervision, with a regular review of their performance and use of checklists for monitoring. If the intervention is to be scaled up in Bangladesh, these and other programme issues will need to be ad-dressed. The working areas of depot-holders should be clearly demarcated and equally distributed, and clear guidelines need to be given for identifying potential clients. The record-keeping system will need to be standardized to collect data for monitoring intervention-related improvements and poverty focus. Since better-off women in Dhaka were less interested in receiving services from depot-holders, the socioeconomic composition of potential intervention areas will have to be assessed. The number and circumstances of the extreme poor, who may require free services, also need to be taken into account if the intervention is to be truly poverty-focused. The presence of facilities run by the Government or other NGOs will have to be taken into account, in view of the potential impact on the use of their services. With the exception of training, most programmatic requirements for scaling up would not incur much additional unit cost. The estimated cost of introducing and sustaining depot-holders for one year (US$ 262) was quite low, taking into account the population covered (less than 1 US$ per household). The depot-holders also generated some profits for the NGO clinics and for them-selves, after taking into account the related costs. In conclusion, this study found that, in an eight-month pilot intervention period, the depot-holders were effective as service providers and promoters of health services in different types of urban setting. The variation in the impact on the use of different services in the three types of area probably reflects local conditions, population characteristics, and programmatic factors. This cautions against generalizing the likely impact of similar interventions in other countries. Nevertheless, the evidence suggests that urban depot-holders can increase the number of service contacts at clinics through promotion and referral and can achieve very large increases in community-based distribution of oral contraceptive pills and ORS. The baseline data and survey instruments used in this study provide a basis for a longer-term assessment of the impact and sustainability of activities of depot-holders in these urban areas. Further evaluation should assess the quality of their services, a wider range of indicators of use and coverage of services, poverty-focus, and cost-effectiveness. Acknowledgements This research was supported by the Office of Health, Infectious Diseases, and Nutrition, Global Health Bureau, United States Agency for International Development (USAID) under the terms of the Cooperative Agreement no. 388-A-00-97-00032-00 with ICDDR,B: Centre for Health and Population Research. The views expressed in this paper are those of the authors and do not necessarily reflect the views of USAID and ICDDR,B. The authors acknowledge the valuable contributions of other members of the research team: Dr. Bushra Amena, Mr. Md. Kamrul Ahsan, Mr. Humayun Kabir, Ms Monowar Jahan, Mrs. Hasin Sultana, and Mr. Nirod Chandra Saha References
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}