 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 24, No. 1, March, 2006, pp. 8-16 Defining Episodes of Diarrhoea: Results from a Three-country Study in Sub-Saharan Africa James A. Wright1, Stephen W. Gundry2, Ronan Conroy3, Daniel Wood2, Martella Du Preez4, Anna Ferro-Luzzi5, Bettina Genthe6, Misheck Kirimi7, Sibonginkosi Moyo8 , Charles Mutisi9, Jerikias Ndamba (deceased)8, and Natasha Potgieter10 1Department of Geography, University of Southampton, Highfield, Southampton SO17 1BJ,
UK [and formerly with Water and Environmental Management Research Centre, University
of Bristol], 2Water and Environmental Management Research Centre, University of Bristol,
83 Woodland Road, Bristol BS8 1US, UK, 3Department of Epidemiology and Public Health
Medicine, Royal College of Surgeons in Ireland, Dublin, Ireland, 4Division of Water,
Environment and Forest Technology, CSIR Environmentek, PO Box 395, Pretoria 0001,
South Africa, 5Istituto Nazionale di Ricerca per gli Alimenti e la Nutrizione_INRAN, Via
Ardeatina, 546-00178 Roma, Italy, 6Division of Water, Environment and Forest Technology,
CSIR Environmentek, PO Box 320, Stellenbosch 7599, South Africa, 7Network for Water
and Sanitation International, Magadi Road, Off Langata Road, PO Box 15614-00503,
Mbagathi, Nairobi, Kenya, 8Research and Technical Services, Institute of Water and Sanitation Development, PO Box MP 422, Mount Pleasant, Harare, Zimbabwe,
9Department of Animal Science, University of Zimbabwe, Mount Pleasant, Harare,
and 10Department of Microbiology, University of Venda for Science and
Technology, Thohoyandou, Venda, South Africa Code Number: hn06003 Abstract The study was conducted to assess the effect of definition of episode on diarrhoeal morbidity and to develop a means of adjusting estimates of morbidity for the definition of episode used. This paper reports on a cohort study of 374 children, aged 9-32 months, in three African countries, which recorded frequency and consistency of stool over a seven-month period. Different definitions of episode were applied to these data to assess their effect on annualized diarrhoeal morbidity. Adjustment factors were then derived that corrected morbidity for non-standard definitions of episode. Applying non-standard definitions of episode gave estimates of an annualized number of episodes between 38% and 137% of the internationally-accepted definition. Researchers should be encouraged to use the standard definition of episode of diarrhoea and to use appropriate field protocols. Where this is not possible, correction factors should be applied, particularly where estimates of diarrhoeal morbidity are pooled in systematic reviews. Key words: Diarrhoea; Morbidity; Definitions; Epidemiology; Sub-Saharan Africa Introduction Diarrhoea accounted for an estimated
1.6 million deaths globally among children aged less than five years and
was the third most important cause of death in 2002 (1). Accurate quantification
of diarrhoeal morbidity is important in understanding the global burden of
disease, so that research effort and resources can be targeted towards the
most widespread diseases. In this regard, episodes have been used for measuring
the trends in morbidity, regional burdens of disease, and the cost-effectiveness
of different interventions.
Studies
on diarrhoea often define an episode differently, making inter-study comparison
of morbidity and estimation of burden of disease difficult. The most widely-accepted
standard definition of a diarrhoea-day is one where a subject experiences
three or more loose or watery stools in 24 hours or any number of loose or
watery bloody stools (2). In identifying diarrhoea-days, any standard definition
must also specify the criteria for defining the end of an episode, particularly
where individuals suffer sporadic bouts of diarrhoea over time. Typically,
an individual must experience a minimum number of consecutive diarrhoea-free
days between episodes. Three consecutive diarrhoea-free days has been proposed
as an international standard (2).
A
recent review drew on 27 studies to estimate global diarrhoeal morbidity
(4). As noted by its authors, the studies identified through the review defined
episodes of diarrhoea in different ways with unknown consequences for regional
estimates of morbidity. In some studies in this review, rather than using
consistency and frequency of stool, a local language was used for identifying
diarrhoea-days. For example, a Zimbabwean study used the Shona word ’manyoka’to
identify days on which diarrhoea occurred (3). The effect of definition of
episode on estimates of morbidity has been assessed using artificially-generated
data (5) and using several datasets from the field (2,6,7). No studies have
so far examined the effect of definition of episode on estimates of morbidity
in sub-Saharan Africa.
This paper addresses this definitional problem by analyzing data on diarrhoea from three sub-Saharan African countries. Data on diarrhoea were gathered using a pictorial diarrhoea-diary, which recorded daily frequency and consistency of stool. The diary enables the calculation of the number of episodes of diarrhoea according to any definition and not solely the international standard definition. We were, thus, able to compare the effects of different definitions of diarrhoea on an estimated annual number of episodes. Based on this analysis, we developed a method for standardizing definitions of diarrhoea. Materials and Methods Study areas
The study areas are located
in the Mutale municipality of Vhembe district, Limpopo province in South
Africa, in Kirinyaga district of Central province, Kenya, and Zaka district
in Masvingo province in Zimbabwe. The South African municipality of Mutale
had a population of 69,313 in 2001, of whom 40% have no access to sanitation
(8). The majority (53%) of the population use public standpipes with a
further 14% using rivers, dams, and springs as sources of water. The Zaka
district in Zimbabwe has a population of 184,814 (9). As of 1992 (more
recent 2002 census data are not yet available), 45% of the population in
the district had no access to protected water sources, and 70% had no access
to any type of sanitation facility (10). The Kirinyaga district in Kenya
had a population of 553,123 in 1999. Within the Central province, 45% of
the population had no access to protected sources of water in 1999 (11).
The Zimbabwean and South African study areas have two distinct seasons:
a prolonged dry spell from May to October and a wet season from November
to April.
Data collection
In each study area, we identified
the five health centres with the highest rates of childhood diarrhoea.
We then asked clinic staff to identify the villages with the highest and
the lowest prevalence of diarrhoea in their catchments and selected these
for study. In each of these villages, we randomly selected 12 households,
plus 2 additional households as replacements. Households selected had at
least one child aged 12-24 months, the age cohort most prone to diarrhoea.
The nature and purpose of the study were explained to participants, and
consent was obtained from the head of each household. In South Africa,
14 extra households, unused as replacements, were retained in the study.
The sample size comprised 374 children (Kenya: 120; South Africa 134; Zimbabwe:
120).
To
overcome the problems described above in defining diarrhoea, we developed
a 'smiley' diary to identify episodes of diarrhoea (12). The diary can
be used where adults have only limited formal education. The diary forms
part of a bigger study of water contamination between source and final
point-of-use in the home. The study investigated the linkages between point-of-use
water quality and diarrhoea among young children, as measured using the
diary (13). Adult caregivers (mostly women) were asked to record episodes
of diarrhoea among children whom they cared for using the diary over approximately
30 weeks. In Zimbabwe, monitoring of diarrhoea took place from November
2002 to June 2003 and in South Africa from August 2002 to April 2003. Because
of possible disruption in fieldwork associated with the Kenyan elections
of December 2002, monitoring in Kenya took place slightly later, from February
to September 2003. As a consequence, the children monitored in Kenya were
slightly older than those in the other two study countries.
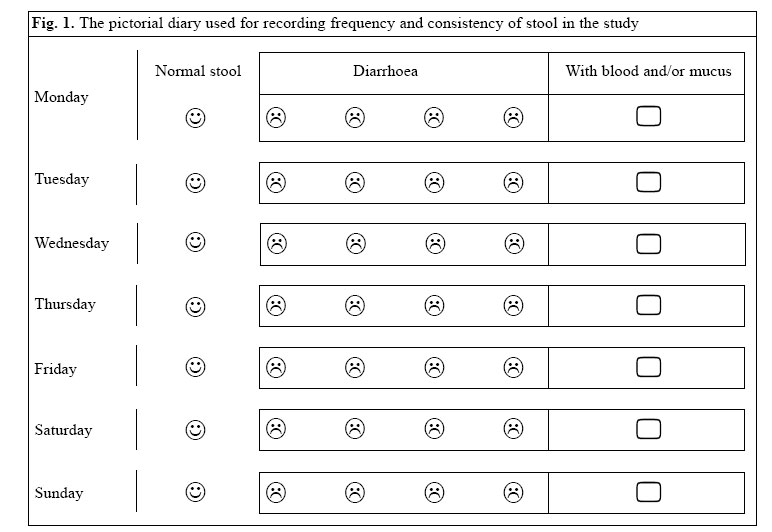
The diary consists of a table
with a separate row for each day of the week (Fig. 1). One smiley face
and five sad faces were drawn on the diary next to each day. If all the
child's stools were normal in a particular day, the caregiver marked the
happy face. Every time the child passed a loose or watery stool, the caregiver
marked one of the sad faces corresponding to that particular day. A loose
or watery stool was defined as one that would take the shape of a container.
The caregiver also marked a box on the right of the diary each day a child
passed blood or mucus in its stools. A different sheet was used for re-cording
episodes of diarrhoea each week.
At the start of the monitoring exercise, a field worker explained the diary
to the women participating in the study. At the end of each week, a field
worker visited the household to collect the sheets, confirm their content
verbally, and check for any problems. The field workers were typically respected
members of the community, such as Village Health Workers, in Zimbabwe. A
project researcher collected and checked the sheets at the end of every month,
which were then computerized.
To
assess the quality of information collected through the diarrhoea-diary,
a trained enumerator asked a sample of child-carers about their children's
diarrhoea status during the preceding 24 hours. This information was
collected, using the standard definition of diarrhoea, during March 2003
in Zimbabwe, May-June 2003 in Kenya, and August-September 2002, and February-March
2003 in South Africa. The trained enumerator was a different individual
to the person responsible for the diary, and this information was collected
independently of the diary in the presence of a senior researcher. We then
cross-checked this information against the entries in the diarrhoea-diary
for the same period.
Data analysis
Effect of definition of
episode on morbidity
Because daily frequency and
consistency of stool were recorded, it was possible to calculate the number
of episodes of diarrhoea experienced by each child in the study according
to various definitions. Each definition varied in terms of the minimum
number of loose or watery stools used for defining a diarrhoea-day, in
terms of inclusion or exclusion of bloody stools, and in terms of the minimum
number of consecutive diarrhoea-free days that defined the end of an episode.
Since
the study was primarily designed to investigate water-quality effects on
health, diarrhoea was monitored for approximately seven months of the year
only. There-fore, the total number of episodes experienced by each child
was scaled up on a pro rata basis to give an annualized number of episodes.
The mean annualized number of episodes per child was then calculated for
each study area and each different definition of an episode of diarrhoea.
In calculating the mean annualized number of episodes, any children for
whom diary-entries were avail-able for less than 60 days were excluded.
Adjusting for non-standard
definitions
We developed a method to standardize
published estimates of morbidity to take into account differences in definition
of episode. Regression analysis was used for assessing how different definitional
components affected morbidity. To do this, we calculated the aggregate
annualized number of episodes according to the different definitions, pooling
data from all countries. We then used ordinary least squares regression
to predict the estimated number of episodes based on the definition used.
The regression analysis examined three components of the definition: (a)
the number of loose or watery stools per day, (b) whether or not bloody
stools were included in the definition, and (c) the number of intervening
diarrhoea-free days defining the start of a new episode.
The
regression coefficients for each of these three definition components could
then be used for standardizing the number of episodes on the internationally-accepted
definition (2).
Evaluating the adjustment
method
We tested the effectiveness
of the adjustment factors. Since we had no access to a similar, independent
dataset from elsewhere to test our methodology, we used village-level data
from our own study to assess our approach. The adjustment factors were,
therefore, derived by pooling data from all three countries but tested
on each village in the study.
To
do this, we calculated the average annualized number of episodes for each
survey village according to the various definitions available. We standardized
the village-level estimates of morbidity for differences in definition
of episode based on the regression analysis described above. For each village,
we then compared the number of episodes according to the standard definition
with the adjusted estimates from the non-standard definitions. To make
this comparison, we used the concordance correlation statistic (14). This
statistic measures the agreement between two sets of measurements without
assuming an underlying distribution. We also measured bias and calculated
limits of agreement using the method described by Bland and Altman (15).
In this context, bias would be a consistent over- or under-estimation of
diarrhoea episodes by the adjustment method (15). The concordance correlation
coefficient can take values between -1 and +1, with +1 indicating perfect
agreement, 0 indicating no agreement, and -1 indicating systematic disagreement.
Results Patterns of morbidity
Of the original 120 children
recruited to the study in each country (134 in South Africa), data on frequency
and consistency of stool were available over a 60-day period or greater
for 83 children in Kenya, 115 children in South Africa, and 111 children
in Zimbabwe. Among children with at least 60 days’diary records,
data on diarrhoea were available for an average of 126 days in Kenya, 195
days in South Africa, and 159 days in Zimbabwe. At the start of the monitoring
period, the Kenyan children had a median age of 26 (range 18-32) months,
the South African children had a median age of 17 (range 9-26) months,
and the Zimbabwean children had a median age of 21 (range 11-26) months.
Fifty-six percent of the Kenyan children were girls compared to 47% of
the South African children and 50% of the Zimbabwean children.
Fisher’s
exact test suggested a significant correlation in Kenya and Zimbabwe between
the diary results and the independently-collected information concerning
childhood diarrhoea (p<0.01 and n=61 in Zimbabwe; p<0.05 and n=34
in Kenya). In South Africa, there was a weak association between the two
datasets (p=0.06; n=57). There were no significant differences in the proportion
of diarrhoea recorded in the diary versus the in-dependent questionnaire
survey.
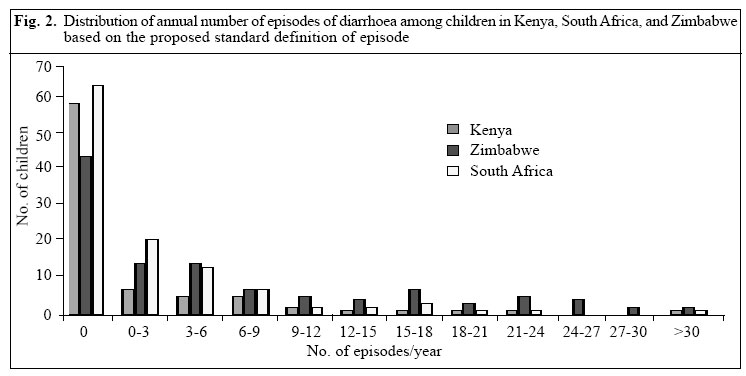
Fig. 2 shows the distribution of the annualized number of episodes of diarrhoea
experienced by children in the three study countries. According to the
standard definition, the mean number of episodes per year was 7.7 in South
Africa, 7.1 in Kenya, and 18.6 in Zimbabwe.
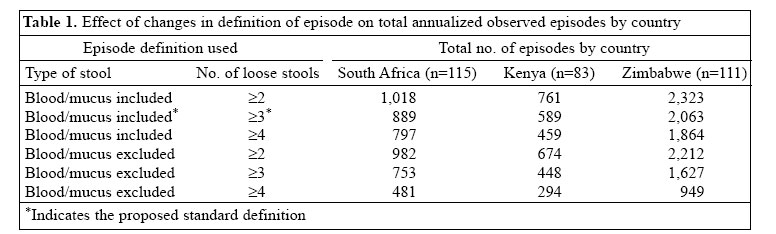
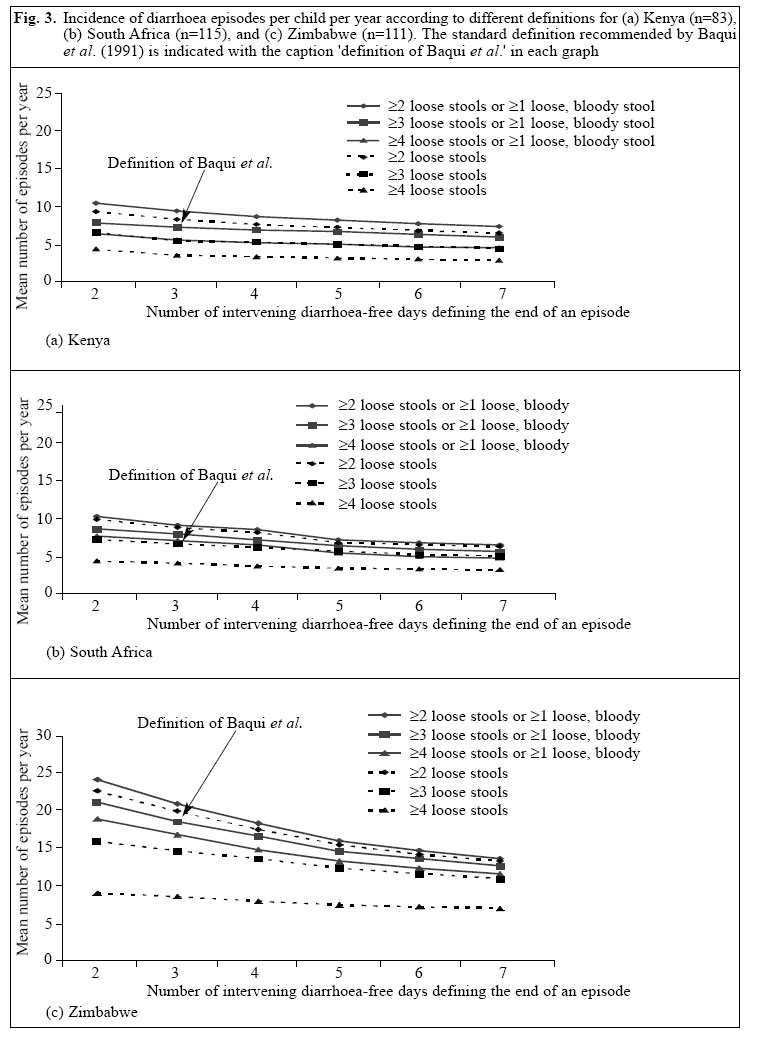
Effect of definition of episode on morbidity Table 1 shows how changes in
the definition of episode affected the total observed number of annualized
episodes in each country. Similarly, Figure 3 shows the annual number of
episodes of diarrhoea per year according to the various definitions in
each country. In all three countries, the definition that gave the greatest
number of annual episodes of diarrhoea was two or more loose/watery stools
per day or one or more loose/watery, bloody stools in a day, and a minimum
of two consecutive diarrhoea-free days defining the end of an episode.
The use of this definition led to an over-estimation of annual episodes
of diarrhoea by 37% (averaging across all 3 countries) compared to the
standard definition. The definition that produced the lowest number of
annual episodes of diarrhoea was four or more loose/watery stools per day
with a minimum of seven consecutive diarrhoea-free days defining the end
of an episode. This definition under-estimated annual diarrhoea episodes
by 62% compared to the standard definition, averaging across all three
countries.
Adjusting for non-standard definitions
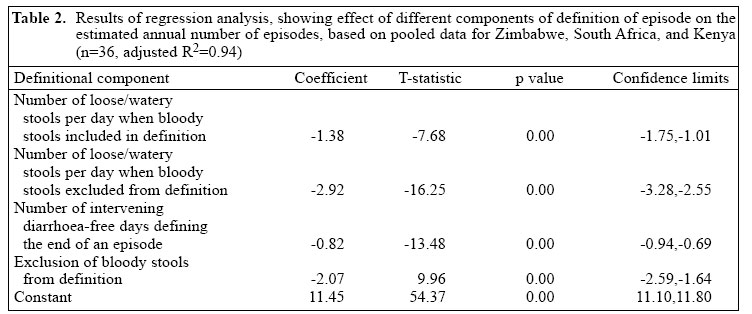
The effect of the three definition
components on the estimated annual number of episodes is shown in Table 2, based on the pooled all-country dataset. The effect of the three definition
components was as follows:
Excluding bloody stools from the definition of diarrhoea significantly reduced the estimated diarrhoeal morbidity by 2.07 episodes per year compared to the standard definition. The estimated annual number of episodes significantly decreased as the number of stools used for defining a diarrhoea-day increased. This effect was greater when bloody stools were not included in the definition. An
increase in the number of intervening diarrhoea-free days that defined
the end of an episode also reduced the estimated annual number of episodes.
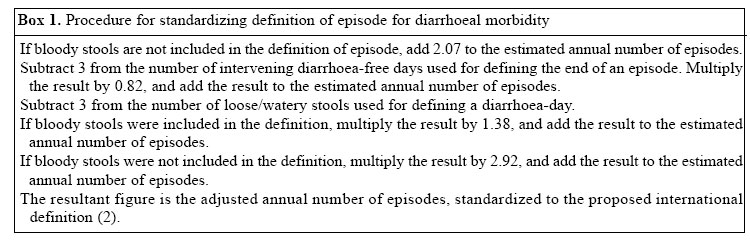
As
shown in Box 1, these regression results could then be used for adjusting
estimates of morbidity to take into account the definition of episode used.
Evaluating the adjustment
method
A comparison of adjusted village-level
estimates of morbidity with their true (standard definition-based) values
gave a concordance correlation coefficient of 0.97 (95% limits of agreement:
-5.3 to 5.4 episodes per year). The unadjusted estimates of morbidity gave
a lower concordance correlation coefficient of 0.95 (95% limits of agreement:
-6.9 to 6.2 episodes per year), when compared with the estimates of morbidity
based on the standard definition. The adjusted estimates of morbidity,
thus, matched the standard definition more closely than the raw, unadjusted
estimates.
Discussion Patterns of morbidity
The estimates of morbidity
for the Zimbabwean study site are high compared to those of previous studies
in Zimbabwe, which have recorded annual episodes of 6.2 and 4.8 (16,17).
Possible explanations for this high morbidity include misreporting through
the pictorial diary, seasonality, and deteriorating socioeconomic conditions
in this study site. Independent questioning of mothers by
different interviewers provided a higher rate of morbidity that was not
significantly different from that derived from the diary. This implies
that the unusually high rate of incidence is not simply an artefact of
misuse of diary, although this remains a possibility. Clinic-based statistics
for Zimbabwe suggest that diarrhoea peaks seasonally during the late rainy
season in January-March and is lowest during July-September (18). Our data
may, there-fore, over-estimate morbidity in Zimbabwe since the low-diarrhoea
season of July-September did not form part of the period monitored here.
The high morbidity may also be due to high prevalence of HIV/AIDS (19),
compounded by deteriorating economic conditions in Zimbabwe.
Although the average annualized number of episodes was high in our study areas, many children remained diarrhoea-free for the whole study period. This finding is consistent with results of studies elsewhere. For example, two Indian studies found 53% and 33% respectively of Indian children suffered from no episodes of diarrhoea (20,21). Similarly, a year-long Papua New Guinean study reported 41% of young children as being diarrhoea-free (6). Effects of definition
of episode
Inconsistencies in the definition
of episode remain a difficulty when comparing the results of different
studies on diarrhoeal morbidity. The results presented here suggest that
such differences can substantially affect the estimated annualized number
of episodes of diarrhoea. Here, non-standard definitions led to over-estimation
of mean annual episodes per child by 37% or under-estimation by 62% compared
to the proposed standard definition (2). The effect of different definitional
components on estimates of morbidity is comparable with earlier studies,
which suggest that the estimated number of episodes decreases as the minimum
number of inter-vening diarrhoea-free days required to define a new episode
increases (2;6).
It
is possible to make an approximate correction for these definitional differences
and, so, improve estimates of the global burden of diarrhoeal disease.
We found that applying the correction factors to village-level averages
produced annualized estimates of episode within -5.3 to +5.4 episodes (95%
limits of agreement) of equivalent figures based on the internationally-accepted
standard definition. Using the ’raw’, uncorrected episode counts
gave estimates of morbidity that were less consistent with the standard
definition, as evidenced by the wider 95% limits of agreement of -6.9 to
+6.2. The adjustment procedure described here, therefore, reduces but does
not eliminate the effect of differences in definition of episode on estimates
of morbidity.
There
are weaknesses in the methodology as presented here. Our cohort study was
primarily designed to investigate the inter-relationship between quality
of water and health outcomes and, so, data on diarrhoea were not collected
over the full calendar year. Diarrhoeal disease varies seasonally in the
tropics (14) and, so, monitoring throughout the year is necessary to estimate
annual morbidity. In this study, data on diarrhoea were collected in both
wet and dry seasons in all three countries, which would mitigate this problem.
The adjustment factors were developed using data for children, aged 12-32
months, in the sub-Saharan African region. It is unclear how far the standardization
method will be applicable to other age-cohorts and regions, where the incidence
of diarrhoea may follow a different pattern. These corrections may only
be used with definitions that are formulated in terms of consistency and
frequency of stool. Findings of studies that rely on local words to define
diarrhoea cannot be adjusted using the definitional correctional factors.
The
results of the analysis presented here suggest that the use of a non-standard
definition of episode can substantially affect estimates of diarrhoeal
morbidity. Future studies on diarrhoeal morbidity should make use of the
proposed standard definition (2), which includes criteria for the end of
an episode and stool frequency. In the interim, most published studies
have used different definitions of an episode. These definitional differences
could be reduced by using adjustment factors similar to those presented
here to published estimates of morbidity. Ideally, such adjustment factors
should be derived from diarrhoea-records for a whole year and drawn from
a broader age-cohort. The adjustment method does not require access to
the original, raw data on diarrhoea.
Acknowledgements This work was funded by the European Union under the INCO-DEV: International Co-operation with Developing Countries Programme (Contract no. ICA4-CT-2000-30039. Title: 'The Policy Implications of Contamina-tion of Rural Water Between Source and Point-of-Use in Kenya, South Africa and Zimbabwe__AQUAPOL'; www.bristol.ac.uk/aquapol/). The authors wish to acknowledge the assistance of final year students at the University of Venda, the Department of Health in Northern Province, South Africa, and the local authorities in Kirinyaga and Zaka districts. The authors also acknowledge the cooperation of the study participants and community leaders in all three study sites, without whose assistance this work would not have been possible. The authors also wish to acknowledge the contributions of their colleague Dr. Jerry Ndamba, who died towards the end of the study. References
© 2006 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn06003f4.jpg] [hn06003t2.jpg] [hn06003t1.jpg] [hn06003f1.jpg] [hn06003f3.jpg] [hn06003f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}