 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 24, No. 1, March, 2006, pp. 17-24 Under-nutrition Affects Time to Recurrence of Gastroenteritis among Aboriginal and Non-Aboriginal Children Andy H. Lee1, Michael Gracey1,2, Kui Wang1, and Kelvin K.W. Yau3 1School of Public Health, Curtin University of Technology, GPO Box U 1987, Perth,Western Australia, Australia, 2Unity of First People of Australia, Perth, and
3Department of Management Sciences, City University of Hong Kong, Hong Kong SAR Code Number: hn06004 ABSTRACT This study investigated whether under-nutrition affected time to hospitalization for recurrence of gastroenteritis in Australian children. Linked hospitalization records of all infants, born in 1995 and 1996 in Western Australia, who were admitted for gastroenteritis during their first year of life (n=1,001), were retrieved. A survival frailty model was used for determining the factors influencing the recurrent times over the subsequent seven years. Aboriginality and under-nutrition were significantly associated with an increased risk of recurrence (hazard ratios of 2.59 and 1.28). Hospitalizations due to gastroenteritis were common among Aboriginal children who had a higher mean re-admission rate and much shorter intervals between re-admissions than other patients. The proportion of patients with recurrence was also significantly higher for Aboriginals (38.5%) than for other patients (14.2%). Gastroenteritis remains a serious problem in Aboriginal children. This presents a complex challenge to be addressed with public-health principles, political determination and commitment, and adequate resources. Key words: Gastroenteritis; Diarrhoea, Infantile; Aborigines; Infant nutrition disorders; Retrospective studies; Cohort studies; Australia Introduction Gastroenteritis is common worldwide
even in industrialized countries, such as the United States where approximately
200 million episodes of acute diarrhoea occur each year (1). It is much more
serious and life-threatening among infants and young children in tropical
and developing countries, often in association with malnutrition (2-4). It
is also prevalent and much more severe in other disadvantaged groups, particularly
those living in over-crowded and unhygienic conditions in otherwise affluent,
hygienic and healthy societies. This is so for Australian Aboriginal infants
and children, particularly those who live in remote and tropical regions
(5-7). Although deaths from gastroenteritis are now rare in Aboriginal children,
their hospitalization rates in Wes-tern Australia are several times higher
than those for their non-Aboriginal peers (5-7).
The
bi-directional interactions between infection and under-nutrition have been
recognized for more than 30 years (8). Infection negatively affects nutritional
status by suppressing dietary intake, increasing catabolism and, especially
in the case of diarrhoeal infections, increasing the losses of nutrients
that are needed for growth and tissue maintenance. Conversely, malnutrition
can increase the risk of infection because of negative impacts on immune
protective mechanisms, for example at the gastro-intestinal mucosa (9). These
interrelationships are very complex and difficult to disentangle, partly
because of the possible effects of confounding variables. Under-nutrition
has been linked to prolonged diarrhoea, its severity, and the likelihood
of subsequent death, particularly in developing countries (9).
Western
Australia is a good location for a study on recur-rent gastroenteritis and
under-nutrition in Aboriginal children because of its accurate and comprehensive
demographic information, its efficient hospitalization data recording, the
routine identification, during hospitalization, of Aboriginal status, and
the capacity to link these data with other characteristics, such as co-morbidities
of patients, and with maternal information (10).
To
investigate the effects of clinical and aetiological factors on the incidence,
prevalence, and recurrence of childhood gastroenteritis in Western Australia,
linked hospitalization records were retrieved to derive the out-come measures,
associated co-morbidities, and other demographic variables for a cohort of
children. Specifically, all infants, born in Western Australia in 1995 and
1996, who were admitted for gastroenteritis during their first year of life
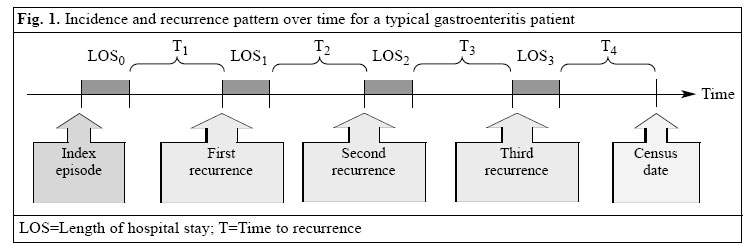
were included in the cohort. Census date was set at 31 May 2002. Figure 1
depicts the incidence (index episode) and recurrence (re-admissions due to
gastroenteritis) pattern over time for a typical gastroenteritis patient
and the associated outcome measures.
Previous studies by our group have examined factors that influence the number
of recurrent episodes of gastroenteritis causing re-admission (11), and
the length of time that infants and children stay in hospital using a baseline
model for repeated length of hospital stay records (12) and advanced frailty
models allowing auto-correlation between observations (10) and clustering
of patients within health districts in a multi-level setting (13). Previously-published
studies by ourselves and others, however, have paid less attention to the
possible impact of under-nutrition on the risk of hospitalization for recurrence
of gastroenteritis episodes in vulnerable groups. The aim of the present
study was to analyze the duration between successive hospitalizations of
infants and children for recurrent gastroenteritis, i.e. the recurrence
times Ti between episodes as shown in Figure 1. The determination of pertinent
factors affecting recurrent hospitalizations is required by health planners
and providers to improve strategic planning and resourcing of prevention
of diarrhoea, related health promotion, and clinical and infrastructure
services to help lessen the burden of gastroenteritis in communities and
at primary and secondary healthcare levels.
Materials and Methods Linked hospitalization
data
The sources of data for this
retrospective cohort study were the Western Australia Hospital Morbidity
Data System (14), the Western Australia Midwives’Notification of
Births, and the mortality database of Australian Bureau of Statistics.
A cohort-study design was chosen because information on hospital separations
is routinely collected for all episodes of hospitalizations through-out
Western Australia. The Health Information Centre of the Department of Health,
Western Australia, extracts linked hospitalization and birth-records of
each individual. Record linkage is used for retrieving the medical history
of each patient from the diagnostic information recorded
on hospital separation summaries. A unique patient number (anonymous) is
attached by record link-age to all hospital separation records for the
same individual to facilitate retrieval of the patient’s information.
The quality of the hospital morbidity-data linkage has been assessed, with
the proportions of invalid and missed links estimated to be 0.11% (15).
All
infants, born in 1995 and 1996, who had an index gastroenteritis admission
during their first year of life were included in our cohort. This group
was followed up until 31 May 2002 to document their recurrent hospitalizations
for gastroenteritis. There were no deaths in this group through the study
interval that were attributed to gastroenteritis or its complications.
The total number of patients was 1,001 after removing eight deaths from
other causes that occurred during the observation period.
In
this study, admissions due to gastroenteritis were de-fined according to
the ICD9-CM codes (before July 1999) and ICD10-AM codes (after July 1999)
for principal diagnoses of diarrhoeal diseases which were: bacterial and
viral diarrhoea, diarrhoea not otherwise specified, protozoal intestinal
diseases, salmonellosis, shigellosis, bacterial food-poisoning, acute amoebic
dysentery, chronic amoebic dysentery, non-dysenteric amoebic colitis, and
candidal enteritis. Acute hospital-discharge data on age, sex, indigenous
status, place of residence, admission type, birth-weight, and co-morbidities
were extracted from the linked records for each patient in the cohort.
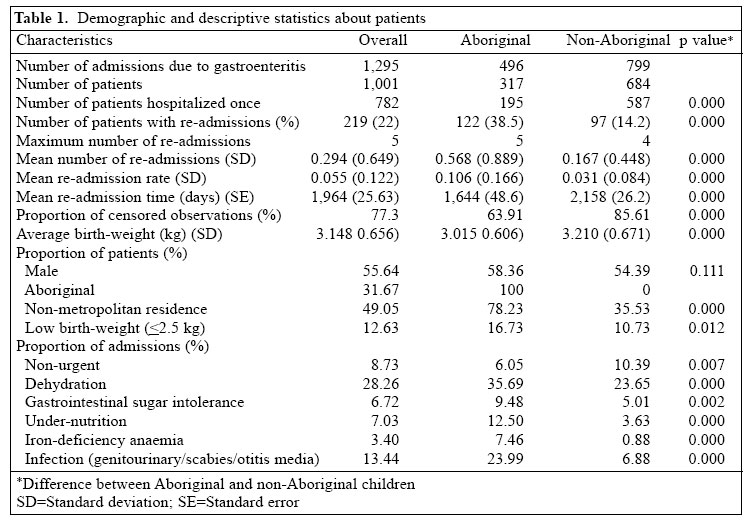
The birth-weights were the checked and recorded measurements of midwives. Trained hospital staff obtained these weights using standard methods and with standardized calibrated equipment, i.e. Avery digital and checked electronic scales. There was only one birth-weight recorded for each individual in the Western Australia Midwives’Notification of Births registry. The nutritional status was assessed based on body mass measurements taken with standardized digital scales (to 100 g) after initial rehydration and in light clothing, and according to age, sex, and body length (to 2 years) or height using standard methodology (16). Under-nutrition was classified according to the ICD9-CM (263.9) and ICD10-AM (E46) codes. Gastrointestinal sugar in-tolerance was detected and recorded if the patient had persistent fluid diarrhoea when on a diet containing sugars, most often lactose, and with evidence of acidic stools, a positive Clinitest examination of the fluid part of a fresh stool specimen, and a clinical response to elimination of lactose or other relevant carbohydrates from the diet (17). Infections were documented, on clinical and microbiological grounds, indicating the presence of otitis media, scabies and/or infections involving the genitourinary tract. Iron-deficiency anaemia was documented on the basis of iron-deficiency (plasma ferritin <10 mg/L, elevated transferrin saturation, mean corpuscular volume, and mean corpuscular haemoglobin readings), and a haemoglobin value <110 g/L. Statistical modeling Linked hospitalization records enabled determination of multiple hospital admissions for each patient during the observation period. For this data setting, the use of Cox’s proportional hazards model that assumes independence of observations becomes inappropriate. By pooling the hospital re-admission episodes, a proportional hazards frailty modelling approach (18) was adopted to determine the factors influencing the recurrence times Ti. The method is a generalization of the Cox’s regression model for time-to-event outcomes in survival analysis but adjusting the within-patient correlation among hospital re-admissions of the same child. This approach has been previously employed to analyze length of hospital stay (12,19). The model-fitting procedure has been built into the S-Plus statistical package (20). The proportional hazards frailty method is applicable to time-to-event data in the presence of both censored and repeated observations. In this study, the time from the hospital separation date of each patient’s last episode of gastroenteritis to the census date (31 May 2002) was considered censored. The frailty approach preserves the semi-parametric nature of the Cox’s regression model and, hence, is robust to misspecification of the baseline hazard function. It improves statistical power by incorporating all available information, including random patient variations. The differences in patient characteristics as a source of extra-variation are accommodated and adjusted in the random component of the frailty model. Effects of potential risk factors on the repeated outcomes can be assessed through the adjusted hazard ratio, with a hazard ratio exceeding 1 implying a higher risk of recurrence relative to its reference category. Determination of pertinent factors would benefit health professionals and clinicians to assess the risk of recurrent gastroenteritis after adjusting for case-mix and the inherent dependency of observations. Results There were 1,001 patients--317
(32%) of Aborigines and 684 (68%) non-Aborigines--among 1,295 total gastroenteritis-related
admissions monitored, of which 38.3% were for Aboriginal and 61.7% for
non-Aboriginal children (Table 1). Hence, the re-admission rates were higher
in the former ethnic group by a differential of 38.5% to 14.2% (p<0.001).
The mean number of re-admissions and the mean re-admission rate among Aboriginal
patients were much higher (p<0.001 for each measure), whereas their
mean elapsed time to re-admission was significantly shorter (p<0.001).
The average birth-weight of Aboriginal patients was significantly less
than that of other patients (p<0.001). There was a highly significant
trend for Aboriginal patients to reside in non-metropolitan areas, and
their rate of low birth-weight was higher (p<0.05). The non-Aboriginal
patients were more frequently admitted non-urgently (p<0.01). Dehydration,
under-nutrition, and infections, such as otitis media, or those involving
the genitourinary tract or the skin, were significantly more common among
Aboriginal patients (p<0.001), and they had significantly higher rates
of gastrointestinal sugar intolerance (p<0.01).
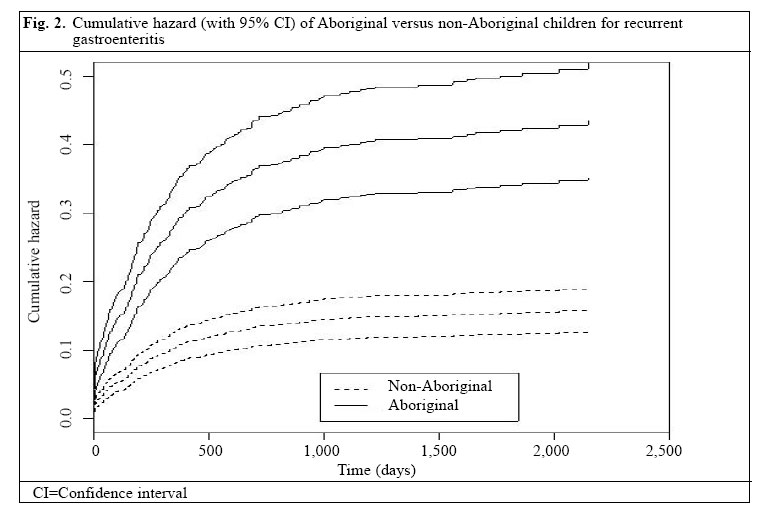
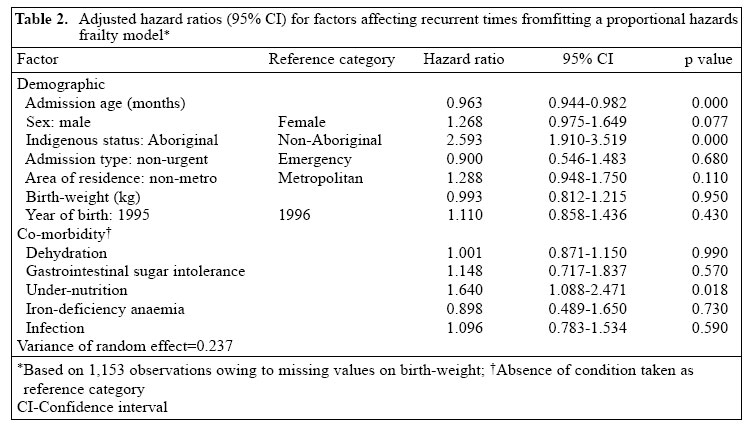
Figure 2 shows the cumulative hazard of recurrent gastroenteritis by indigenous status. The cumulative hazard of recurrence of gastroenteritis was, in general, higher for Aboriginals, especially during the first three years following hospitalization from the previous episode. In the framework of proportional hazards frailty modelling, adjusted gastroenteritis re-admission hazard ratios are shown in Table 2. The effects of confounding factors have been incorporated in the statistical model, while observations with missing birth-weight values were removed in the analysis. Older children experienced a lower risk of recurrent gastroenteritis, with a reduced hazard of 3.7% per month of age or equivalently reduced by 36.4% per year of age. Aboriginality and the presence of under-nutrition were significantly associated with a higher risk of recurrence, with hazard ratios of 2.59 (95% confidence interval [CI] 1.91-3.52) and 1.64 (95% CI 1.09-2.47) respectively. The random component variance estimate of 0.237 suggests moderate extra-variation among the repeated observations from some patients. Such variations in frailty among patients have demonstrated the usefulness of applying the frailty modelling approach to analyze the time to recurrent event data. Discussion Aboriginal people comprise
only 3.2% of Western Australia's population of 1.85 million (Australian
Bureau of Statistics' 2001 Census of Population and Housing). Compared
to the rest of the population, they generally have much more serious health
problems, including high infant mortality, very high rates of infections
and nutritional disorders, and reduced life expectancy (5,21-23). This
study has shown that young Aboriginal patients experienced a much shorter
duration between re-admissions for these infectious diarrhoeal diseases.
Approximately, 32% of patients and 38% of hospital admissions came from
this numerically small minority group. Re-admissions were also significantly
much more frequent among Aboriginal patients, and their average time to
re-admission was much shorter than that for other patients, especially
in the first three years after their previous episode of hospitalization
(Fig. 2).
There
were some other important characteristics that were different between the
two groups of patients. The mean birth-weight of Aboriginals was significantly
lower, and more of them resided in non-metropolitan locations in this vast
state (area=2.5 million sq km). Complicating medical conditions, such as
dehydration, under-nutrition, and gastrointestinal sugar intolerance, were
significantly more common in the Aboriginal cohort, whereas clinically-important
co-morbidities, including iron-deficiency anaemia and a wide range of infections
of the skin, ears, and genitourinary tracts, were very significantly more
common among Aboriginal patients. Although these are not new observations,
they help explain why Aboriginal patients were hospitalized and re-hospitalized
more frequently than non-Aboriginal patients for gastrointestinal infections
and parasitic infestations. This may also help explain why proportionately
more non-Aboriginal patients were hospitalized non-urgently; that is, because
there were relatively fewer complications or co-existing diseases among
them. Re-admission was significantly associated with indigenous status
of patients and the existence of under-nutrition (Table 2). The positive
association between pre-existing under-nutrition and later hospitalization
for recurrent episodes of gastroenteritis suggests that compromised nutritional
status is a contributing factor to recurrent episodes of infectious diarrhoea,
notwithstanding the complex interacting synergistic and antagonistic relationships
between nutrition and infection that were first proposed by Scrimshaw in
the late 1960s (8) and have been reviewed by him recently (24).
Several
limitations should be considered when interpreting the findings of this
study. First, it is possible that inadequate primary healthcare services
closer to home may help explain the excess hospitalization rates of rural
Aboriginal children. Regrettably, information was not available on the
distance from the children's homes to the nearest primary healthcare facility.
Second, only episodes of infectious diarrhoea or gastroenteritis requiring
hospitalizations were included. Data on children attending outpatient clinics
are not captured by the Hospital Morbidity Data System. Third, information
on such factors, as feeding patterns, dietary adequacy, and micronutrient
deficiencies that are typically obtained by nutritional surveys, was not
available from the accessible databases.
Our
experience shows that diarrhoeal diseases are prevalent in infants and
children of this particular ethnic group, namely Australian Aborigines.
Others working with other ethnic groups, including indigenous populations,
have reported similar experience. For example, results of pioneering work
of Mata among Mayan children in the Guatemalan highlands showed that their
early lives were punctuated by repeated episodes of infections, including
those involving the gastrointestinal tract and that these were associated
with under-nutrition and growth failure (25). Sack, Santosham, and their
colleagues showed that diarrhoeal diseases were major public-health problems
among native American Apache children living in reservations in southwestern
parts of the United States; they remarked that the epidemiologic and microbiological
patterns of disease were similar to those found in developing countries
(26,27). Later work among American Indian and Alaskan native children demonstrated
that diarrhoea-related hospitalizations for these children from 1980 to
1995 declined to levels similar to those in the national US population
(28). Such improvements have not occurred among Aboriginal infants and
children in Western Australia over recent years (6). Examples of other
ethnic groups in which diarrhoeal diseases have been well-documented include
children in northeastern Brazil (29), in the West African nation of Gambia
(30), and in Pakistan (31) and many other parts of the Indian sub-continent,
including India and Bangladesh. Many of these studies have concentrated
on particular aspects of childhood diarrhoeal illnesses, such as their
epidemiology, aetiologic agents, the causes of persistent diarrhoea (32),
co-morbidities, methods of treatment, and preventive public-health measures,
including the use of vaccines. In the vast literature on child-hood infectious
diarrhoeas, few authors have focused on this issue as a particular problem
of indigenous populations within generally affluent and otherwise healthy
nations, such as Australia.
The heavy burden of infectious diarrhoeas among Australian Aboriginal infants and children is very complex and multi-factorial. Many of these infections are transmitted by the faecal-oral route and, therefore, are prevalent where living conditions are overcrowded and unhygienic, where sewage and waste disposal are inadequate, and where personal, family and community levels of hygiene behaviour are risky for the transmission of infecting microorganisms or disease-carrying vectors, such as flies (6,33,34). Understanding about transmission of infectious diseases and prevention of related ill-nesses among members of affected families is often poor. This increases their risk of exposure to a range of infectious illnesses, including diarrhoea, particularly among infants and young children. This can result in delayed transfer to clinic or hospital, thus necessitating hospitalization rather than brief treatment as an outpatient or in a day clinic or at home under supervision (6,21). Furthermore, Aboriginal people in remote parts of Australia tend to live long distances from hospitals and have limited access to primary and secondary health-care compared to other Australians. These factors and health and nutrition promotion and provision of clinical services at primary and secondary levels are needed to help overcome this serious problem. Acknowledgements The authors thank Diana Rosman, William Pyper, and Peter Somerford of the Department of Health, Western Australia, for providing data and coding information, and Dr. Valerie Burke, Department of Medicine, University of Western Australia, for statistical advice. Thanks are also due to the Editor and anonymous reviewers for their constructive comments and suggestions. The authors are grateful to the Office of Aboriginal Health of the Department of Health, Western Australia, for supporting this project. This research was supported financially by research grants from the Australian Research Council (Project ID DP0559204) and the Research Grants Council of Hong Kong SAR.
© 2006 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn06004t2.jpg] [hn06004f1.jpg] [hn06004t1.jpg] [hn06004f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}