 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
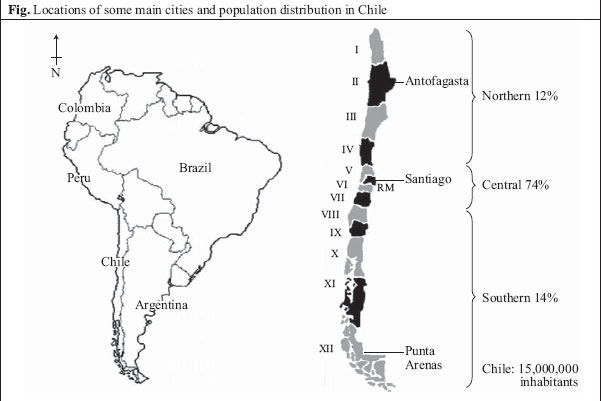
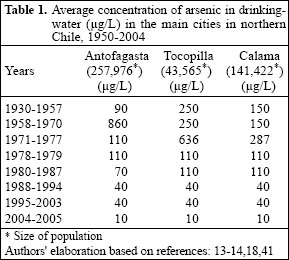
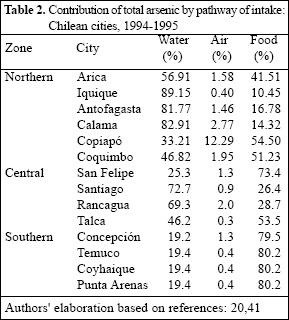
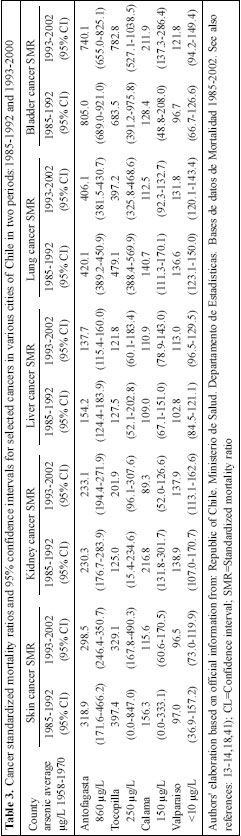
Journal of Health, Population and Nutrition, Vol. 24, No. 2, June, 2006, pp. 164-175 Review Article Arsenic Exposure and Its Impact on Health in Chile Catterina Ferreccio1, Ana María Sancha2 1Departamento de Salud Pública, Facultad de Medicina, Pontificia Universidad Católica de Chile, Marcoleta 434, Santiago, Chile and 2Department of Civil Engineering, Division of Water Resources and Environment, University of Chile, Santiago Correspondence and reprint requests should be addressed to: Prof. Catterina Ferreccio Departmento de Salud Pública Pontificia Universidad Católica de Chile Marcoleta 434, Santiago Chile Fax: 6331840 Email: cferrec@med.puc.cl Code Number: hn06021 Abstract The problem of arsenic in Chile was reviewed. In Chile, the population is exposed to arsenic naturally via drinking-water and by air pollution resulted from mining activities. The sources of arsenic were iden-tified to estimate the exposure of population to arsenic through air, water, and food. Health effects, particularly early effects, observed in children and adults, such as vascular diseases (premature cardiac infarct), respiratory illnesses (bronchiectasis), and skin lesions have been described. Chronic effects, such as lung and bladder cancers, were reported 20 years after peak exposure and persisted 27 years after mitigation measures for removing arsenic from drinking surface water were initiated. Although the effects of arsenic are similar in different ethnic and cultural groups (e.g. Japanese, Chinese, Indian, Bangladeshi, American, and Taiwanese), variations could be explained by age at exposure, the dose received, smoking, and nutrition. Since health effects were observed at arsenic levels of 50 µg/L in drinking-water, it is advised that Chile follows the World Health Organization's recommendation of 10 µg/L. The Chilean experience in removal of arsenic suggests that it is feasible to reach this level using the conventional coagulation process. Key words:Arsenic; Arsenic exposure; Health effects; Impact studies; Chile Introduction Arsenic is present in most eco-systems in northern Chile and in some parts of central Chile, either naturally or by man-made causes, the latter derived from mining activi-ties (1,2,3). The most extensive contamination of arse-nic lies in the region between 17° 30’ and 26° 05’ South Latitude and between 67° 00’ West Longitude and the Pacific Ocean (Fig.). Naturally-occurring arsenic in Chile is associated with the volcanic activity of the Tertiary and Quaternary periods in the Andes Mountains (4). This activity still continues as evidenced in lava flows, geysers, fumaroles, thermal waters, and other geo-thermal phenomena relating to the Pacific’s so-called ’Ring of Fire’. These geological conditions explain the particular chemical characteristics of water in the zone: high pH, variable alkalinity, hardness, moderate-to-high salinity, high silica, and variable concentrations of boron, fluoride, and arsenic (5). Arsenic present in sources of surface water for human consumption corresponds to the species arsenic(V) (6). Historically, concentrations of arsenic in water for human consumption vary, depending on sources of water or arsenic-removal treatments used. The soils of the nor-thern zone also exhibit elevated and variable levels of arsenic and scant plant cultivation in the area (7-10). Intense mining activity, principally copper smelting, generates significant emissions of arsenic into the atmos-phere, which, in turn, precipitates downwind in soils, snow, and waters. The air of some cities in the area is conta-minated with arsenic, and such concentrations are di-rectly related to nearby copper smelting (3,7,11,12). Arsenic exposure Continental Chile is 5,000 km long. The population of 15,000,000 is distributed among the northern, central and southern zones, which account for 12%, 74%, and 14% of the population respectively (13). Only the inha-bitants of the northern zone have been exposed to high concentrations of arsenic. The experience of northern Chile regarding arsenic exposure in drinking-water is a quasi-experiment, marked by a sudden increase in arsenic levels that lasted a few decades until an arsenic-removal plant was built. In as much as this zone is desert, drinking-water supplied by the water-treatment facility is the only source of water for the population (14). At its foundation in 1860, the city of Antofagasta obtained its drinking-water by distil-lation of sea water. As the population grew, they obtained water from rivers coming from mountains. The Siloli River with levels of arsenic between 90 and 100 µg/L was used until the mid-1950s, when the population reached 100,000; the scarcity of drinking-water forced the use of a new water source-the Toconce River with levels of ar-senic ranging from 800 to 900 µg/L. The exception was a few households whose water was supplied since 1871 by the Railway Company which brought water from the Siloli River. In 1892, they represented only 5% of water consumption in Antofagasta; as the population grew, the percentage covered by the Siloli river decreased to negligible amounts (15). During 1950-1978, inhabitants of the northern region were exposed to average concentrations of arsenic from 90 to 860 µg/L. The highest exposure began abruptly in 1958, when the source of water for most of the region’s population changed to the Toconce River and the Hojalar River, both with very high concentrations of arsenic (16). In May 1970, the first arsenic-removal plant began operation, and the arsenic content in drinking-water rapidly dropped to 110 µg/L (17). In 1979, a second water-treatment plant started functioning, and concentrations of arsenic were reduced to 40 µg/L. Since 2003, levels of arsenic have further dropped, reaching 10 µg/L in 2004 (18) (Table 1). Given both geological and anthropogenic conditions in the northern zone of Chile described above, arsenic exposure is multimedia and, perhaps, unique, and cer-tain interesting questions arise: which pathway of the intake of arsenic is the most critical for human population and on which pathway should mitigation measures be focused within the context of a nation with limited economic resources? (19). To answer these questions, an arsenic-exposure study of the entire Chilean population was conducted between 1994 and 1998 (20). An estimate of daily ambient expo-sure was made by combining the information obtained through environmental monitoring, i.e. arsenic concentration per exposure source-air, water, and food-with estimations of volume of air inhaled, water ingested, and foods consumed. The results demonstrated that drinking-water was the principal source of arsenic exposure in the northern and central zones, while foodstuffs were the principal pathway in the rest of the country (Table 2). In numeric terms, arsenic contamination by air was the least significant of the three pathways. Arsenic conta-mination from foodstuffs, except for some isolated cases in the northern altiplano, is relatively constant through-out Chile, largely because the vegetables grown in the central zone and the animal meat, dairy, and wheat pro-duced in the southern zone are supplied to the entire country. Most vegetables cultivated in the northern altiplano are only traded in the local markets for approximately 4,000 people, of mainly atacameños and quechuas ancestors (local indigenous people). For this specific population, food makes a substantial contribution to their total intake of arsenic (7-9). Various studies have demonstrated that foods are the main contribution to total intake of arsenic only when arsenic in water and air is negligible (21-24). Health Impacts There have been a series of reports concerning both early and chronic deleterious health effects attributed to arse-nic contamination of water in north Chile. Early health effects Infant deaths Promptly after the peak exposure years, there was an increase in infant mortality rate in Antofagasta (Region II). This excess was estimated at 18-24% of deaths for the 1958-1965 period (25). Skin lesions In Region II, since 1919, there have been reports of arseni-cosis-leukoderma, melanoderma, and hyperkeratosis- but only associated with workers of nitrate mines (17); two years after the increase of arsenic exposure in drink-ing water, began reports of children presenting arseni-cosis (26,17) and arsenicosis associated with respiratory symptoms, including diffuse and segmentary bron-chiectasis (17). Twenty years after peak exposure, 12% of school children in Antofagasta presented arsenicosis, and 28% presented chronic bronchitis compared to only 4% among children of the non-exposed city of Iquique (16). In the city of Antofagasta, the number of children with arsenicosis bronco-pulmonary disease was 2.5 times higher than among children without such lesions. However, three years after the installation of the arsenic- treatment plant, the prevalence of cough or dyspnea dropped from 38% to 7%. In the general population, there was an excess of respiratory symptoms and vascular problems associated with arsenicosis (27). Respiratory and cardiovascular diseases A few years after peak exposure, children were reported to have peripheral vascular diseases, including Raynaud syndrome and ischaemia of the tongue. Twenty-two percent of patients hospitalized in Antofagasta presented peripheral vascular syndromes, such as achrocianosis, and 30% had Raynaud syndrome compared to none among Iquique patients (16,17). In 1973, researchers concluded that the most frequent clinical complications in children associated with arsenic in drinking-water were respiratory and cardiovascular diseases (28). Be-tween 1967 and 1970, they described a younger age of cardiac infarct in the city of Antofagasta, where 10% of cardiac infarction cases were under the age of 41 years compared to only 1.5% in Santiago; 53% of these younger cases presented arsenicosis (29). In autopsies of children in Antofagasta, peculiar vascular lesions, consisting of intimal thickening of small and medium arteries, were found, mainly in the heart, gastrointestinal tract, skin, liver, and pancreas (30). In 1980, a study comparing autopsies of children from Santiago and Antofagasta concluded that the morbid condition associated with ingestion of arsenic had resulted in: systemic occlusive arterial disease, diffuse hypertrophy of the myocardium, arterial hypertension, arterial thrombosis, bronchiectasis, hepatic cirrhosis, haemangioendotelioma of the liver, chronic diarrhoea, recurrent bronchopneumonia, and bilateral pneumonia. The author postulated that malnutrition interacts with arsenic to cause these morbid conditions (31). Chronic effects The first report of a higher risk of death due to lung cancer in Antofagasta was described for the 1976-1978 period, i.e. 20-25 years after the period of high exposure began. Standardized mor-tality ratios (SMRs) for lung cancer were 503 for Antofagasta and 449 for Tocopilla, i.e. five and four times higher, respectively, than the national average. The authors attributed this disparity to arsenic in drinking-water (32). An ecological study conducted during 1994-1996 generated a database of arsenic exposure and deaths due to cancer for the 1950-1996 period, covering each of the 335 Chilean municipalities (33-35). For each municipality, the lifetime cumulative arsenic exposure (by air and water) was estimated for six age-groups (cohorts), and such exposure was related to mortality due to cancer in the 1985-1992 period. They studied cancer of the lung, bladder, kidney, skin, and liver, and gastric cancer not associated with arse-nic, which was used as a comparison. Arsenic exposure through drinking-water was determined to be a highly significant risk factor (Poisson regression analysis) for all cancers associated with arsenic, but it showed no association with gastric cancer. Airborne arsenic could not explain the excess risks for any of the cancers. They concluded that the most important public-health impact of arsenic in drinking-water was lung cancer (33,35). The main relative excesses of mortality due to cancer, adjusted for age and sex, during 1985-1992, were for bladder cancer (SMR of 805 in Antofagasta), followed by lung cancer (SMR of 420 in Antofagasta). The risk of cancer in Antofagasta persisted high even 20-30 years after the treatment plants were in place; from 1993 to 2002, risks of dying from bladder and lung cancers in Antofagasta were four and seven times higher than the rest of Chile respectively (Table 3). With a similar ecological approach, other authors estimated that arsenic might account for 7% of all deaths among those aged 30 years and above, indicating that this would be the greatest impact ever reported from environmental exposure to a carcinogen in the general population (36). A case-control study of lung cancer conducted during 1993-1996 in North Chile demonstrated a dose-response effect of arse-nic exposure in drinking-water and the risk of lung cancer, inclu-ding a significant interaction between smoking and arsenic in the risk of lung cancer (14). Mitigation measures In the 1970s, treatment processes to remove arsenic from drinking-water sources in the northern zone were initiated. Today, there are three arsenic-removal plants operating (two in Antofagasta and one in Calama). Combined, these installations treat 1,500 litres per second of surface water with average arsenic concentrations of 400-450 µg/L, and in 2004 reduced these to 10 µg [Cáceres A. Personal communication, 2005] of arsenic per litre (Table 1) (37). However, there are still problems of high concentrations of arsenic in water consumed by small, scattered, largely indigenous, communities in the northern Andes (3,000 inhabitants) that are being re-solved as we write this report [Mr. Jorge Molina, Head of Regional Government. Seminario Internacional: El Arsénico en la Segunda Region. 17 November 2005. Universidad de Antofagasta] (38). The Chilean experience in removal of arsenic at treat-ment plants by coagulation processes indicates that re-moval of arsenic is most efficient using FeCl3 as a coa-gulant and that key factors in arsenic removal are: che-mical species of the arsenic present, pH of water; and dosage of oxidizing agent and coagulant, velocity of agitation, and removal processes of the arsenic-flocs formed (5). At the level of individual households and small communities, the experience in Chile has not been so successful. In principle, the devices tested in the field, based on coagulation-filtration processes with low doses of coagulants, reduced arsenic to safer concen-trations. In practice, however, this model has not been implemented in small communities due to lack of moti-vation of people in reducing arsenic because they do not see any health problem in their vicinity relating to drinking-water. Their main concern is about quantity of water, organoleptic characteristics, and sanitary quality (Unpublished observations). DiscussionPublic-health and political management of the arsenic problem Conversations and interviews conducted by the investi-gators in the study with principals in Antofagasta of an earlier era made it clear that the responsible officers of the water utility and health officials in the 1950s were advised that the new sources of water used contained arsenic in excess of the standards. The presence of a chemical, which did not change the colour or odour of water, nor produced any immediate evident health prob-lem among the inhabitants, appeared at that time less of a problem than the need for providing sufficient quantities of water of good microbiological quality. In those years, diarrhoea and malnutrition were the principal causes of infant deaths and shorter life-expectancy in Chile. The National Health Service had only recently come into existence and did not have epidemiologists in the region to initiate health surveillance. The first news and warning signs concerning the health effects attributable to arsenic were revealed by paediatricians and pathologists in hospitals in Santiago, 10 years after the onset of arsenic exposure (26,28,30). Following these reports and the resulting public alarm, mitigation measures were taken (27,39). The case of arsenic in Chile can be explained in part by the sanitation priorities of that time, but also by in-sufficient understanding of the health risks posed by exposure to arsenic in water. This case underlines the critical importance of epidemiologic surveillance in en-vironmental interventions and new housing projects from their outset. It also emphasizes the importance of the precautionary principle with potential health risks. On the positive side, the excellent response of the natio-nal health system in the 1970s should be highlighted. Under the leadership of Dr. J.M. Borgoño, a team of national and local epidemiologists undertook a study which enabled them to characterize the arsenic prob-lem, describe the magnitude of the damage, and advo-cate the immediate installation of a plant to remove the contaminant. Simultaneously, the health system initiated a surveillance programme of drinking-water quality that is in place until today, determining arsenic at multiple points of the city, at different times, every day (18). Characterization of arsenic risk: lessons learnt Excess of lung cancer in the general population was caused by exposure to arsenic in drinking-water In the early 1990s-30 years after the initial arsenic ex-posures and 15 years after installing treatment plants- high rates of lung cancer in Region II sparked new con-cerns among health officials and the public. The suspected cause was airborne arsenic coming from mining acti-vities. At that time, the people did not associate ingested arsenic with lung cancer (40). In 1994, Chilean research agencies (41) funded a multidisciplinary team, which in just three years, demonstrated that the principal source of arsenic exposure for the general population was natu-rally-occurring arsenic in drinking-water and that past exposure was the main cause of the current excess of lung cancer in Region II (14,33-35). Results of various studies showed that most popula-tion of Region II had similar levels of arsenic in air and food as the rest of Chile; content of arsenic in drinking-water was the main difference among the regions (20,42). Although some mining areas of Region II had elevated levels of arsenic in air, as in the copper mine at Chuqui-camata, only 3% of its inhabitants presented arsenicosis compared to 50% of people in the coastal city of Toco-pilla, the latter with high levels of arsenic in water (39). This review, which has focused principally on exposure to arsenic in the general population in Chile, did not con-sider workers in the copper smelters who are exposed to inorganic arsenic in the air, which is known to increase the risk of lung cancer (43,44). When the contamination of drinking-water has been solved in the whole of Region II, arsenic in the air will emerge as a public-health prio-rity in some mining areas and cities of Region II (i.e. the city of Calama). Arsenic interacts with smoking to increase the risk of lung cancer In 1981, Pershagen demonstrated the multiplicative eff-ects of tobacco and arsenic exposure in air among smel-ter workers (45). Results of our studies showed a signifi-cant interaction between smoking and arsenic exposure in drinking-water (14). Rates of smoking and lung can-cer in Chile are increasing countrywide; it is possible that the rate of lung cancer in II Region will not decrease because the past exposure to arsenic will interact with the growing smoking rates. An active anti-smoking cam-paign should be put in place in the region. Paradoxical effect of arsenic in risk of bladder cancer In our case-control study of bladder cancer (manuscript in preparation), we found that bladder cancer odds ratio (OR) for arsenic in drinking-water were smaller (OR: 2.2, 95% confidence interval [CI] 1.2-4.3) than the SMR for bladder cancer seen in Antofagasta (SMR: 743, 95% CI 527.1-1,038.5). We hypothesize that arsenic may not increase the incidence of bladder cancer but cause a more serious evolution of the disease (33-35); further research is needed to clarify this issue. Arsenic may interact with nutritional status to increase health effects Cases of bronchopneumonia among arsenic-exposed children have been associated with severe malnutrition (29). In his description of arsenicosis in Antofagasta, Zaldivar concluded that malnutrition interacted with arsenic, increasing the prevalence of bronchiectasis and recurrent bronchoneumonia (31). Mazunder, in 1998, found that skin lesions were a little higher in people with poor nutrition, although not statistically significant (46). A recent case-control study in West Bengal demonstrated that low intake of calcium, animal protein, folate, and fibre increased susceptibility to arsenic-caused skin lesions, doubling the risk in the lowest intake (47). Stu-dies in Chile have not provided sound data about the association between nutrition and arsenic due to lack of nutritional research in the high-risk period and high uncertainty in current research based on retrospective assessment of nutrition. Skin lesions present a dose-response relationship with arsenic exposure; effects of arsenic may be partly reverted In the high-exposure period, 35% of the population of Antofagasta presented skin lesions (17,28,39). Zaldivar estimated that the incidence rate of skin lesions in 1968 was 145.5 and 168 per 100,000 males and females res-pectively, dropping to 9 and 10 per 100,000 respectively in 1971, only one year after the operation of the treat-ment plant (29). Soon after treatment was in place, a marked reduction in arsenicosis and respiratory symp-toms was also described by Borgoño (27). Concentration of arsenic in drinking-water has also been associated with skin lesions in a dose-response manner in West Bengal, India (46,48-49), and Mexico (50). Recent stu-dies have demonstrated that the peripheral vascular effects seen at exposures of 180 µg/L of arsenic are also reverted after arsenic dropped to 37 µg/L (51). Dose-response and reversal of effects (skin, respiratory, and vascular) after removal of the agent are strong causal criteria not fre-quently found in environmental research. Skin lesions may be a marker of arsenic susceptibility Coldness of fingers, abdominal cramps, and respiratory signs in Chile were significantly higher among people who presented arsenicosis of the skin (28,39). Mazumder, also with same observation in West Bengal, demonstrated that respiratory symptoms were associated with skin arsenicosis (52). Among patients treated with Fowler's solution, the excess of bladder cancer only occurred in cases with arsenicosis (53). In Chile, 44% of lung can-cer cases and 8% of controls presented skin lesions; 3.3% of cases and 0.2% of controls had previously been diag-nosed with skin cancer (54). People with skin lesions deserve medical advice to avoid other risk factors and proper follow-up for early detection of an arsenic-associated malignancy. Andean communities do not differ in susceptibility to arsenic Some researchers reported that Andean communities exposed to high levels of arsenic did not present arseni-cosis or cancers when assessed in cross-prevalence stu-dies, concluding that indigenous people may have some genetic resistance to arsenic (55,56). Nevertheless, a few pieces of information indicate that they, in fact, may have the same risk as the general population in Region II: in our case-control studies of lung and bladder cancers (14,33-35), we identified two cases of bladder cancer and six of lung cancer in individuals who had lived in San Pedro; twice as many as expected (unpub-lished observations). Smith showed that skin lesions were as frequent as expected among this population (57), and results of methylation studies suggest that their me-tabolism is similar to that of other populations (58-59). Some data suggest that methylation patterns aggregate in families and are correlated in siblings (r=0.3-0.8) (60), which could, in part, explain why skin lesions also aggre-gate in families (57). Although the high risk may not be evident in small communities, public-health officers should offer them the same protection as they do in large urban communities. Health effects are very similar in different ethnic and cultural groups Populations exposed to arsenic in drinking-water have been reported in the USA (61,62), Mexico (50,63,64), Argentina (65-67), India (52,68), Bangladesh (69-71), Taiwan (72-77), and Japan (78). Skin, vascular and respiratory effects, and cancers seen in this Chilean population have also been described in those populations (79-84). We have not seen an increase in risk of diabetes, hypertension, or neurological diseases described by others (69,75,83). Data from the 2003 National Health Survey in Chile showed that the prevalence of hypertension and diabetes in Region II are either similar to or lower than the national average, adjusting for age and sex (85). We have not studied the impact of arsenic on the intellectual function of children, which some authors have recently described (86). We do not have evidence regarding the effects of calcium, animal protein, folate, and fibre in susceptibility to arsenic-induced skin lesions as others have postulated (47). We have seen peripheral necrosis (27-30) but have not found the Blackfoot disease as described in Taiwan (87). Some differences in reported health effects may be due to study design and some may be real, and due to interaction of arsenic with genetic and environmental factors. Biomarkers of arsenic The Andean populations exposed to arsenic have an increase in micronuclei in exfoliated bladder cells, indi-cating that arsenic is inducing genetic damage (88-89) as also described in West Bengal (90) and reviewed by Chen (91). A recent report described elevated-but not statistically significant-micronuclei in buccal cells in exposed populations in Region II; micronuclei were unrelated to ethnic background (92). The differences in findings among studies may be related to variations in the study methods, the type of tissue studied, or to the chemical form of arsenic. It is necessary to learn more at the molecular level to identify early biological markers of exposure, susceptibility, and results. Current standard of 50 µg/L of arsenic in drinking-water may not be a safe level for Chile Our studies showed a decrease in birth-weight (-57 g) among newborns of mothers exposed to water with 40 µg/L of arsenic (93). We recommend that the arsenic- removal plants currently operating in Chile continue to be closely monitored to optimize, in a sustained man-ner, the efficiency of the present arsenic-removal pro-cesses. These have very recently been shown to be capable of producing water with 10 µg/L residual arsenic, i.e. at the maximum concentration recommended by the World Health Organization (94). The key parameters in efficient removal of arsenic are strict control of pH and accurate doses of the coagulant agent, controls for which technology is available (95,96). Arsenic is not a new contaminant in Chile. The ori-ginal American settlers of these lands were exposed to this chemical element. Arsenic has been being removed from drinking-water in the northern region for 35 years using coagulation processes with simple technology and at a reasonable cost. This has enabled the control of ar-senic exposure in drinking-water in urban areas, reducing it between 1988 and 2003 to concentrations averag-ing 40 µg/L. More recently (2004-2005), arsenic levels have fallen to 10 µg/L through the automatization of the dosage levels of chemical agents-Cl2 and FeCl3-and better control of the pH of water treated. Despite our broad arsenic-removal experience and the great progress achieved to date, it has not yet been possible to resolve satisfactorily the problem of arsenic exposure in drinking-water of small, isolated Andean communities. These small communities of people in the northern Altiplano, until recently, continued without adequate solution due to technical or economic limitations. In our field work, it has become apparent that removal of arsenic is just one of the problems for which these populations require solutions. First and foremost, they need to be able to count on sound programmes of environmental sanitation and health education which could facilitate the acceptance and commitment of the community to the prog-ramme of arsenic removal from their water. AcknowledgementsThe authors wish to express their gratitude to FONDEF/ CONICYT for supporting the research "The environ-mental regulation of toxic substances: the case of arsenic in Chile". The authors thank FONDEF researchers: Guillermo Marshall, Nella Marchetti, Patricia Frenz, Raúl O`Ryan, Pablo Ulriksen, Jack Wiertz, and Claudia Gonzalez and also Alessandra Gederlini who collaborated with the authors for statistical analysis. References
The following images related to this document are available:Photo images[hn06021t1.jpg] [hn06021t3.jpg] [hn06021f1.jpg] [hn06021t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}