 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
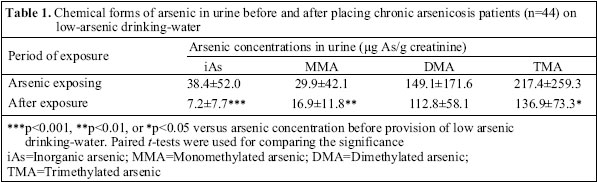
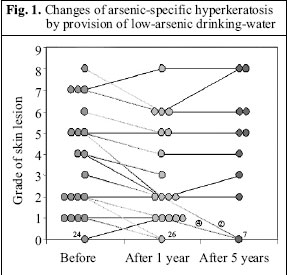
Journal of Health, Population and Nutrition, Vol. 24, No. 2, June, 2006, pp. 176-181 Review Article Current Research Problems of Chronic Arsenicosis in China Guifan Sun, Xin Li, Jingbo Pi, Yang Sun, Bing Li, Yaping Jin, Yuanyuan Xu Department of Occupational Health, School of Public Health,China Medical University, Shenyang 110001, China Correspondence and reprint requests should be addressed to: Prof. Guifan Sun Department of Occupational Health School of Public Health China Medical University Shenyang 110001 China Email: sungf@mail.cmu.edu.cn Fax: 86-24-23261744 Code Number: hn06022 ABSTRACT Chronic arsenicosis is a newly-emerged public-health issue in China and many other Asian countries. Over 200 million people are estimated to be at the risk of high arsenic exposure from drinking-water in the Asian region. To protect people from the hazards of chronic arsenic poisoning, the Chinese Government has been providing low-arsenic drinking-water to some seriously-affected rural areas, such as Inner Mongolia autonomous province. Results of follow-up studies showed that both the average values of arsenic, including inorganic arsenic (iAs), monomethylated arsenic, dimethylated arsenic and trimethylated arsenic, and 8-hydroxydeoxyguanine in urine, decreased significantly after drinking low-arsenic water for one year, and arsenic-specific skin lesions also improved to some extent. However, a five-year follow-up study showed no more significant improvement of skin lesions, while the potential risk of arsenic-induced cancers after cutting off high-arsenic exposure was still uncertain and indefinite. The susceptibility of children compared to adults to chronic arsenic exposure and the need to re-evaluate the appropriate standard of arsenic in drinking-water were also discussed in this paper. Key words: Arsenicosis; Arsenic; Arsenic contamination; Arsenic poisoning; Water pollution; Water supply; Drinking-water; China Introduction Endemic chronic arsenicosis is a serious public-health problem that now affects millions of people in Asian countries, including Bangladesh, China, India, Cambodia, Lao PDR, Mongolia, Myanmar, Nepal, Pakistan, and Viet Nam. Arsenicosis is mainly caused by drinking water from pump-wells contaminated by high levels of arsenic, and in some areas of China, by eating food dried by burning arsenic-rich coal. Chronic arsenic poisoning can impair several systems of the body, giving rise to skin lesions with hyperpigmentation, depigmentation, and hyperkeratosis, arsenic-related cancers of the skin, lung, and bladder (1-2), vascular diseases, such as peripheral and cardiovascular diseases, arteriosclerosis, black foot disease, and hypertension (3-5), non-specific symptoms of the impact on the digestive system, such as abdominalgia, diarrhoea, and dyspepsia, and mental slowing or loss of memory (6). China, Bangladesh, and India are the most severely-affected countries in Asia. Tens of thousands of people in these countries have been diagnosed with arsenicosis. Patients suffering from this are afflicted with hyperke-ratosis on the palms and soles, which impede living and working, and present the danger of carcinogenesis in the future. Arsenic toxicity has complex and far-reaching consequences on developing child, such as cognitive delays, reduced IQ, mental slowing, and poor memory (7). There is no known medical cure so far for arsenicosis or any workable ways and means to alleviate its long-term harmful effects on human beings. The only sure way of preventing this is to cut off the intake of arsenic. The Chinese Government has been providing low-arsenic drinking-water to some seriously-affected rural areas, such as Inner Mongolia autonomous province. This paper mainly focuses on our research in China, especially in Inner Mongolia, and discusses the current problems, such as short- or long-term changes in skin lesions, and the potential risk of arsenic-induced cancers after water improvement projects and changing to low-arsenic drinking-water. We have also discussed the susceptibility of children compared to adults to chronic arsenic exposure and about the need to re-evaluate the appropriate standard of arsenic in drinking-water. Short- and Long-term effects of drinking low-arsenic water In China, about three million people, mostly in rural areas, are exposed to high levels of arsenic, while 30,000 people have been diagnosed with arsenicosis (1). The typical syndromes are known as arsenic-specific skin lesions, which vary from person to person. One type is simple hyperpigmentation, and another is hyperpigmentation combined with depigmentation. In addition, arsenic-specific hyperkeratosis usually involves the palms and soles symmetrically, developing from mini-papules at the early stage to piece-papules subsequently, and eventually decreasing the ability of patients to work. Up to now, there are no effective ways of improving the skin lesions or curing the disease, except stopping people from drinking or consuming contaminated water or dried food. The Chinese Government have now introduced two ways of eliminating the intake of arsenic by: (a) early detection of arsenic contamination in drinking-water, food, and the environment and (b) identifying arsenicosis patients; and at the same time, providing low-arsenic drinking-water and improving ventilated stoves in the vast affected areas and population. We have focused on a follow-up study in an epidemic area of arsenicosis in Inner Mongolia to observe the effects before and after the provision of low-arsenic water supply (6,8,9). In this research, about 20% of 2,080 subjects in the Gangfangying village of Inner Mongolia showed signs of arsenic-specific skin lesions. The average arsenic concentration in well-water of this village was 0.13±0.2 mg/L (range 0.001-1.79 mg/L; 47.2 % of total 303 wells had higher levels of arsenic than 0.05 mg/L). A water-pipe was laid from the village to a well 10 km away, and this well-water (with an arsenic level of 0.037 mg/L) was used instead as the alternative low-arsenic water. Forty-four volunteers who participated in the study showed a decrease in most forms of arsenic in urine one year after switching to low-arsenic water (Table 1). We also observed the reduction of skin lesions after improving the quality of drinking-water. In this case, a trained dermatologist observed the degree of skin hyperkeratosis and made a score from moderate 0 to severe 9 according to the standards set up in advance. Twenty volunteer subjects with skin symptoms were randomly selected and classified into different grades. Results showed that the degrees of skin hyperkeratosis were generally alleviated mostly among 18 patients followed up for one year after the provision of alternative water (Fig. 1-2). Two cases developed a more severe degree of hyperkeratosis. Ten patients remained after a five-year follow-up study. Results were not as expected, and no more significant improvements were observed compared to that of four years before. Two patients had even deteriorated. Although this follow-up study was an elementary observation and needs to be confirmed by more complete human epidemiological data, it seems that provision of low-arsenic drinking-water does have some protective effects on patients, resulting in decreased arsenic levels in urine and in the improvement of arsenic-specific skin lesions to some degree. However, cutting off the high arsenic exposure did not completely stop the progress of arsenic-related injuries, as we showed here that some persons still exhibited no improvement or even aggravated skin symptoms.
Potential risk of arsenic-induced cancer
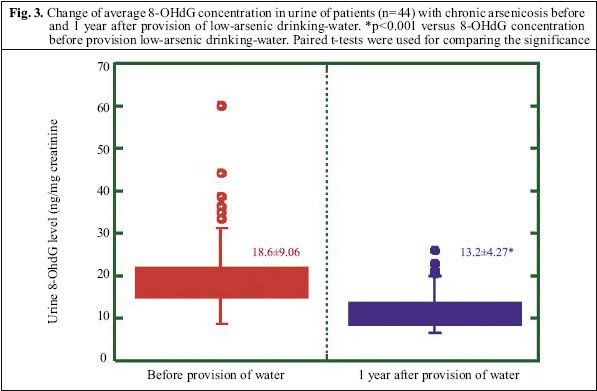
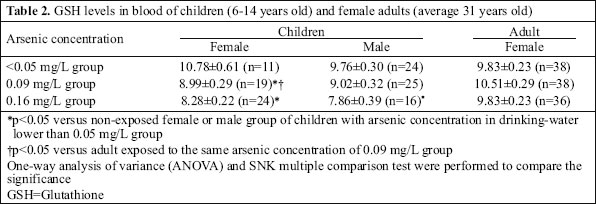
It is well-known based on strong epidemiological data that inorganic arsenic is a human carcinogen. Arsenic exposure in humans is associated with a marked increase in cancers of the skin, lung, liver, kidney, and urinary bladder (10-12). A primary concern for chronic arsenic exposure in human populations is its carcinogenic potential. Mongolia also found proliferative skin lesions, including Bowen’s disease and skin cancer (1). The latency period in humans for inorganic arsenic carcinogenesis is about 20-30 years (8). In China, the average exposure period in most epidemic areas is about 20 years; therefore, there is the potential for a marked increase in arsenic-induced cancer in the very near future. According to the hypothesis of some experts, carcinogenesis may soon become a major factor of the adverse health effects from arsenic exposure in China (13). The mechanism of carcinogen due to arsenic is still unclear, although several mechanisms, including DNA oxidative damage, have been proposed in recent years (14, 15). The metabolic by-product of oxidative DNA damage—8-hydroxydeoxyguanine (8-OHdG)—has been used as an indirect measurement of the extent of such damage (16). Our research group became interested in urinary levels of 8-OHdG as a potential biological indicator of the extent of oxidative DNA damage induced by arsenic exposure in humans. We detected the levels of 8-OHdG in the urine of patients with arsenic-specific skin lesions of hyperkeratosis and pigmentation disorders (8). The average 8-OHdG concentration in these patients (18.6±9.1 ng/mg creatinine) was significantly higher than that of normal healthy people (14.2±9.0 ng/mg creatinine). While one year after the provision of alternative low-arsenic water, the average 8-OHdG concentration (13.2±4.3 ng/mg creatinine) in urine was reduced to normal levels (Fig. 3). This indicates that DNA damage induced by chronic arsenic exposure may be improved when excessive arsenic exposure is stopped. There was still a group of people among the 44 subjects, whose 8-OHdG levels were beyond the upper limit of the average value. This probably indicates that these patients were still at risk of aggravation or even carcinogenesis. In a follow-up cancer-incidence study (2,110 residents) in an arsenic-affected area in the Xinjiang autonomous region of China from 1980 to 1995, six cases of cancer-related deaths were reported in eight years before the supply of low-arsenic water. However, 13 cancer-related deaths in the same area eight years after the water improvement project were put into practice. Nine of the 13 cases had lung cancer, which was obviously a higher incidence than in the drinking-water area not affected by arsenic (17). This also provides evidence that carcinogenesis may continue even after removal of arsenic from drinking-water. Effects of chronic arsenic exposure on children Children sometimes differ from adults in their susceptibility to hazardous chemicals. We have found arsenic-specific skin lesions in infants aged 6-18 months (17). In addition to arsenic-specific hyperkeratosis and pigmentation disorders, other adverse effects of arsenic exposure in children include cognitive delays, reduced IQ, slowing of mental growth, and poor memory. In an epidemiological study, our study group found that non-protein sulfhydryl (NPSH) levels in the blood of the high-arsenicexposuregroupwere 42.4% lower than those in the low-exposure group, and the blood NPSH levels inversely correlated with the concentrations of inorganic arsenic and its methylated metabolites in blood (18). In a recent research carried out in Inner Mongolia, we found that the glutathione (GSH) level in the blood of children exposed to arsenic as high as 0.16 mg/L by drinking water was significantly lower than that in the non-exposed group, while there was no marked difference between the female and the male group of children exposed to the same concentration. The GSH level of children exposed to arsenic as high as 0.09 mg/L was significantly lower than that of adults exposed to the same concentration (Table 2). These data suggest that children are especially susceptible to the harmful impacts of arsenic exposure. The potential mechanism of this susceptibility is not yet completely clear. It has been suggested that the high susceptibility of children is probably due to the higher arsenic exposure per body-weight compared to adults (19). Although no cases were identified where arsenic was transmitted from mother to child, animal-model research has provided evidence that arsenic may be located in infants and their brains through the undeveloped placental barrier and blood-brain barrier, thus indicating the possibility of transmitting arsenicosis from mother to child (20). Millions of children and women are at present, chronically exposed to arsenic in China. The potential impacts of arsenic exposure on children and their future life are an urgent problem confronted by China and most other countries affected by arsenicosis. Contradiction of drinking-water limit for arsenic: 0.05 MG/L or 0.01 MG/L? Since results of epidemiological research suggest that chronic arsenic exposure may induce arsenicosis and the fact that inorganic arsenic is a human carcinogen, the exact drinking-water limit for arsenic has generated much scientific discussion and debate. Whether the limit should be changed from 0.01 mg/L to 0.05 mg/L has drawn much of attention and given rise to many controversies among researchers and governments. Lack of a good animal model, until recently, has forced scientists to rely on human evidence, particularly in studies of cancer in Taiwanese villagers exposed to arsenic from wells from the 1920s to the 1960s. Chiou et al. examined cases of urinary tract cancer in villagers exposed to arsenic levels as low as 0.01 to 0.05 mg/L (21). This study, the first of its kind, found that cancer risk rose with arsenic levels even at these low levels of exposure. Such kinds of important human studies still need to be enriched and repeated in other endemic areas. According to the latest data of the Prevention and Treatment Academy of China, people exposed to arsenic beyond 0.01 mg/L have reached 14.66 million, of whom nearly 9.03 million are exposed to arsenic ranging from 0.01 mg/L to 0.05 mg/L. Therefore, the health hazards and the risks of cancer incidence facing this vast population is one of the very important and imperative problems to Chinese researchers. Detailed studies focusing on these particular populations will provide more convincing evidence for the scientific and appropriate arsenic standard of drinking-water. In fact, establishing the drinking-water limit for arsenic is not only a scientific problem, but also a social problem facing China and other countries. Conclusion As far as the endemic chronic arsenic poisoning in China is concerned, future research and control of arsenic problem in China should mainly include: (a) observation of long-term impacts on population cutting off high-arsenic exposure and trying to explore other effective ways of prevention and treatment; (b) carrying out more detailed epidemiological studies on the potential risks of arsenic-induced cancers; and (c) greater concentration on the potential hazards to children and infants and people exposed to arsenic ranging from 0.01 mg/L to 0.05 mg/L. AcknowledgementsThe authors thank Dr. Takahiko Yoshida, Department of Hygiene, Asahikawa Medical College, Japan, Dr. Yoshito Kumagai, Institute of Community Medicine, University of Tsukuba, Japan, and Dr. Hiroshi Yamauchi, Department of Preventive Medicine, St. Marianna University School of Medicine, Japan, for their excellent contribution to the study. References
The following images related to this document are available:Photo images[hn06022f3.jpg] [hn06022t2.jpg] [hn06022f2.jpg] [hn06022f1.jpg] [hn06022t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}