 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
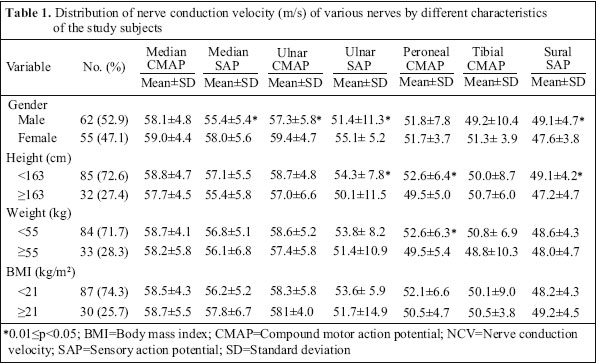
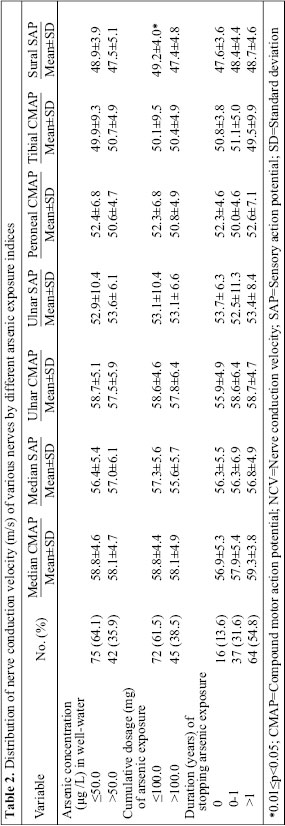
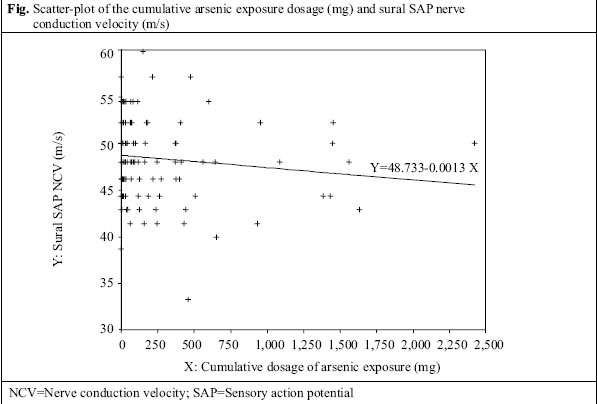
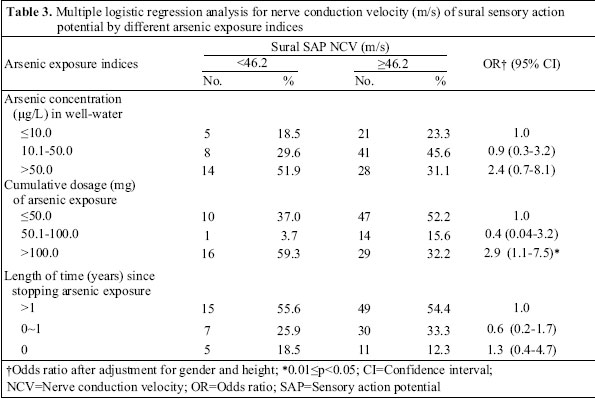
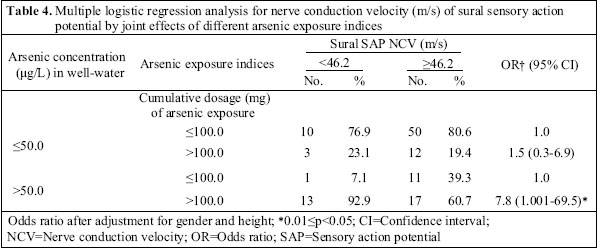
Journal of Health, Population and Nutrition, Vol. 24, No. 2, June, 2006, pp. 182-189 Association between Chronic Exposure to Arsenic and Slow Nerve Conduction Velocity among Adolescents in Taiwan Hung-Pin Tseng1, Yuan-Hung Wang2, Meei-Maan Wu2, Hee-Wen The2, Hung-Yi Chiou2, and Chien-Jen Chen3 1Department of Neurology, Lo-Hsu Foundation, Inc., Lotung Poh-Ai Hospital, 83 Nan-Chan Street, I-Lan 265, Taiwan and Ching-Kou Institute of Management and Health, 336, Fu-Shing Road, Gee-long 203, Taiwan, 2School of Public Health, Taipei Medical University, 250 Wu-Hsing Street,Taipei 110, Taiwan, and 3 Graduate Institute of Epidemiology, College of Public Health, National Taiwan University, Taipei 100 Correspondence and reprint requests should be addressed to: Dr. Hung-Yi Chiou School of Public Health, Taipei Meical University 250 Wu-Hsing Street, Taipei 110 Taiwan Email address: hychiou@tmu.edu.tw Fax: +886-2-23779188 Code Number: hn06023 ABSTRACT The association between chronic exposure to arsenic and peripheral neuropathy has been controversial in previous studies, which may be due to the influence of factors, such as age, gender, chronic diseases, occupational injuries, and arsenic exposure. To clarify the question of this association, a cross-sectional study was designed. In total, 130 junior high school students aged 12-14 years were included and exami-ned for the motor and sensory nerve conduction velocity of peripheral nerves in their right-upper and lower limbs. Concentrations of arsenic in well-water and history of drinking well-water were retrieved from a baseline database created in 1991. After adjustment for gender and height, a significant odds ratio of 2.9 (95% confidence interval [CI] 1.1-7.5) was observed for the development of slow nerve conduction velocity of the sural sensory action potential (SAP) among the study subjects with a cumulative arsenic dosage of >100.0 mg. In addition, a borderline statistical significance with odds ratio of 7.8 (95% CI 1.001-69.5) for the development of slow nerve conduction velocity of sural SAP was also observed among the study subjects who drank well-water containing arsenic concentrations of >50.0 μg/L and with a cumulative arsenic dosage of >100.0 mg. The study found that chronic exposure to arsenic might induce peripheral neuropathy. It also found that the slowing of the nerve conduction velocity of sural SAP might be an early marker of chronic arsenic neuropathy. Key words: Arsenic; Arsenic exposure; Nerve conduction velocity; Sensory action potential; Cross-sectional studies; Taiwan Introduction Arsenic is a widely-distributed element in the environment. It is mainly transported into the human body through the intake of seafood or well-water (1). Chronic exposure to arsenic has been associated with various health effects, including internal cancers (2), skin hyperpigmentation and hyperkeratosis (3-4), hypertension (5), diabetes mellitus (6), ischaemic heart disease (7,8), cerebrovascular disease (9), and peripheral vascular occlusive disease (10). Peripheral neuropathies—acute or chronic—are affected by many factors and are easily induced by occupational injuries (11) and chronic diseases (12,13). Previous reports have found that acute exposure to arsenic is associated with peripheral neuropathy with both axo-nopathy and demyelination (14-16). Chronic arsenic exposure, in contrast, was not found to be consistently associated with peripheral neuropathy. The different results obtained in previous studies for chronic exposure to arsenic might be due to a small sample size, a lack of consideration regarding the potential influences of chronic diseases and occupational injuries, or an absence of a correlation between peripheral neuropathy and arsenic exposure dosage. Positive (17-19), slightly-positive (20), and negative (21) results have been reported. Results usually appear as a polyneuropathy with symptoms of distal axonopathy and predominant sensory involvement. Histologic reports for chronic neuropathy relating to arsenic exposure are rare. A study exploring histologic changes on sural nerve biopsy of chronic arsenic neuropathy reported a reduction of both myelinated and unmyelinated fibres associated with axonal degeneration (22). No demyelination of nerve fibres was noted in this study. The histologic discrepancy between acute and chronic arsenic peripheral neuropathy might suggest different mechanisms in their pathogenesis. Arsenic neuropathy can be detected by the slowing of the nerve conduction velocity (NCV) in an electrophysiological examination. The NCV results may be affected by age, sex, body height (23), body mass index (BMI) (24), body surface temperature (25), occupational injuries, and chronic diseases. In our present study, we chose teenagers, who had similar age distribution and had low possibility of chronic diseases or injuries, as our study subjects. The male gender and taller body height were taken into consideration as these factors may make the NCV slower. After adjusting for sex and height, a dose-response relationship between periphe-ral neuropathy and inorganic arsenic exposure indices through drinking well-water was investigated among the residents of Lanyang Basin in Taiwan. Materials and Methods Subjects Residents living in the Lanyang Basin, a region in northeastern Taiwan, who have been drinking well-water for decades, were used as subjects. Although a tap-water system exists, some residents still use well-water for economic reasons. In our previous study, 8,102 residents (4,056 men and 4,046 women), who were more than 40 years old and who agreed to participate in the study, were interviewed in their homes during October 1991–September 1994 (9). All residents lived in four townships, namely Chiaohsi, Chuangwei, Wuchieh, and Tungshan. The junior high school located in Chungwei was randomly sampled, where 162 students from Grades 1 and 2, aged 12-14 years, were selected. A detailed illustration of the study and a informed consent paper were given to every student. After obtaining consents from students and their parents, the students were included in the study. The illustrator did not know the arsenic exposure indices of invited students, and the involvement of participants was totally dependent on the agreement they and their parents made on the informed consent paper. One hundred thirty students and their parents agreed to participate in the studyandcompleted the questionnaire, which included requesting information on personal basic data, history of well-water usage, residential and disease history. The rate of participation was 80.25%. The 32 students who did not join the study had no difference in age, gender, and body-weight compared to the 130 participants who did join the study. The reasons for choosing adolescents as study subjects were: (a) to exclude the influences of occupationalinjuries and chronicdiseases, especially diabetes mellitus, which occurs in adults (occupational injuries and chronic diseases may affect the NCV severely and mask the changes) and (b) to include subjects (adolescents) who could understand the questionnaire and research purposes and cooperate in the examination of nerve conduction velocity. Estimation of arsenic exposure Concentration of arsenic in well-water was measured in a previous large-scale endemic survey (9). A detailed history of residential consumption of water, including water source, duration and amount of consumption, was obtained from the questionnaire-interview. In total, 3,901 well-water samples (one sample from each household) were collected during home-interviews and immediately acidified with hydrochloric acid and then stored at -20 °C until the subsequent assay. Hydride generation combined with flame atomic absorption spectrometry was used for determining concentrations of arsenic in these samples. Arsenic levels ranged from undetectable levels (<0.15 ppb) to 3.59 ppm. Arsenic exposure indices The arsenic exposure level of each study subject, who had been drinking well-water, was derived from the concentration of arsenic found in well-water of each household. Concentration of arsenic in well-water was stratified into two groups as ≤50.0 and >50.0 μg/L. The cumulative dosage of arsenic exposure (mg) was calculated as: concentration of arsenic in well-water (μg/L) × volume (mL/day) × drink year (years) × 365 (days/year) × 10-6; this was then stratified into two groups as ≤100 and >100 mg. The length of time since stopping arsenic exposure was stratified into three groups as 0, 0-1 and >1 years. Examination of nerve conduction velocity The NCV was examined by an NCV machine (ISA1004EP, Micromed Company). Since the correction of temperature was necessary to measure NCV, an electric heater was used for maintaining room temperature at 25 °C to condition body surface temperature. Median, ulnar, peroneal, and tibial compound motor action potentials (CMAPs) and median, ulnar, and sural sensory action potentials (SAPs) of the right-upper and lower limbs were recorded for each study subject. We used supra-maximal current, which made the amp-litude of action potentials of stimulated nerves stable and as big as possible and then calculated the NCV of each nerve. The SAP was measured by an anti-dromic method. Statistical methods The NCV in different groups of concentration of arsenic in well-water, the duration of arsenic exposure, the cumulative amount of arsenic exposure, and the length of time sine stopping arsenic exposure were examined by t-test. Linear regression analysis was applied to estimate the association between cumulative arsenic exposure dosage (mg) and sural SAP NCV. NCV data were analyzed according to quartiles of sural SAP measurement; the first quartile (46.2 m/s) was used as the cut-point and stratified into two groups (<46.2 m/s and ≥46.2 m/s). In further analysis, gender- and height-adjusted odds ratios and their 95% confidence intervals (CIs) for arsenic-related neuropathy by different groups of long-term arsenic exposure indices were calculated through multiple logistic regression analysis. A p value of <0.05 was considered statistically significant. Results In total, 130 students were invited to participate in the study. Due to the technical difficulty of the sural SAP NCV measurement, nine students could not be detected precisely. In addition, four students without sufficient data (including arsenic concentration of well-water, years of arsenic exposure or volume of drinking well-water) were also excluded from the study. Finally, 117 students (62 males and 55 females) were included in sequent analysis. The distribution of NCV by gender, height, weight, and BMI is presented in Table 1. A significantly decreased NCV, including median SAP, ulnar CMAP, ulnar SAP, and sural SAP, was observed among the male group. Those with more height (≥163 cm) had a significantly decreased NCV, including ulnar SAP, peroneal CMAP, and sural SAP compared to those with less height (<163 cm). There were no significant influences of weight and BMI on NCV, except for a significantly decreased NCV of peroneal CMAP among the study subjects with a body-weight of ≥55 kg. The distribution of NCV by different arsenic exposure indices is shown in Table 2. Among subjects who drank water from well with a concentration of arsenic >50.0 μg/L, there was a slight but not significant decreased NCV, including median CMAP, ulnar CMAP, peroneal CMAP, and sural SAP. In terms of cumulative dosage of arsenic exposure, only subjects with a cumulative dosage of >100.0 mg had a significant decreased NCV of sural SAP. In addition, as the duration of stopping arsenic exposure increased, there was a non-significant increased NCV of the studied nerves. On the other hand, the higher cumulative arsenic exposure dosage was associated with a decreased sural SAP NCV (β=-0.0013 and p=0.1749) (Fig.). Table 3 shows the association between the risk of slow NCV of sural SAP (<46.2 m/s) and three arsenic exposure indices. A statistical significance of gender- and height-adjusted odds ratio of 2.9 (95% CI 1.1-7.5) was observed among the study subjects with a cumulative dosage of arsenic exposure of >100.0 mg. Compared to the reference group of study subjects who drank well-water containing arsenic concentrations of ≤10.0 μg/L, the gender- and height-adjusted odds ratio of 2.4 (95% CI 0.7-8.1) was observed among the study subjects who consumed well-water with arsenic levels of >50.0 μg/L. Moreover, compared to the study subjects who had stopped drinking arsenical well-water for more than one year, a statistically non-significant gender- and height-adjusted odds ratio of 1.3 (95% CI 0.4-4.7) was observed. The study subjects who drank well-water with arsenic levels of >50.0 μg/L and whose cumulative dosage of arsenic exposure was >100.0 mg had a borderline statistical significance of gender-and height-adjusted odds ratioof 7.8 (95% CI 1.001-69.5, p=0.0487)fordecreased NCV of sural SAP (Table 4). Moreover, a non-significant gender- and height-adjusted odds ratio of 1.5 (95% CI 0.3-6.9) was also observed among the study subjects who drank well-water with arsenic concentration of ≤50.0 μg/L and whose cumulative dosage of arsenic exposure was >100.0 mg. Discussion Although 130 junior high school students were initially invited to participate in the study, 13 of them who did not provide adequate information were excluded. Nine of the 13 students had undetectable sural SAP NCV and four students did not have sufficient data regarding arsenic concentration, years or volume of drinking. Finally, 117 students were included in sequent analysis. With regard to the measurement of NCV, CMAP, produced by muscle contraction with larger amplitude (unit: mV), is easily measured; SAP, produced by potentials passing the peripheral nerve with much smaller amplitude (unit: µV), is easily affected by the environment and is more difficult to measure. The median and ulnar nerves have fixed locations and are just under the finger skin. Their SAP can be measured without much difficulty by ring electrode, which circumscribes the finger. The sural nerve, on the contrary, has variable location and is beneath the adipose tissue of the skin. It can only be measured by surface electrode and may be immeasurable due to technical problems. This study found an effect of arsenic exposure on peripheral nerves, especially for sural SAP. Our findings on the effects of gender on NCV are consistent with those of previous reports (23). Since measurements of NCV might be different among various adolescent groups due to the effects of hormones and daily activity, we recruited the first and the second grade junior high school students as study subjects. Although only parts of the results were significantly different for height (ulnar SAP, peroneal CMAP, and sural SAP), our data showed a decreasing pattern of NCV in taller individuals and the general concept of NCV recommendation. In a previous study, chronic arsenic exposure-related neuropathy of sensory involvement was more predominant than motor involvement (17). The incidence of polyneuropathy diagnosed by the slowing of NCV of nerves in the lower limb was higher than those in the upper limb due to the longer length of nerves in the lower limb. These two reasons might explain why sural SAP was the only significantly involved nerve in our study. We suggest that the slowing of sural SAP NCV might be an early disease marker of arsenic-related neuropathy. However, because occupational injuries and chronic diseases may affect the NCV severely and mask changes in sural SAP, this finding cannot be directly generalized to adults, who constitute a large proportion of the general population and are of great interest. A study by Rahman MM et al. was conducted on chronic arsenic neuropathy, which included 413 subjects who were examined for clinical manifestations, such as paraesthesia and muscle weakness (20). The study found arsenic-related neuropathy in 37.3% (154/413) in one group and in 86.8% (33/38) in another. Most cases had mild and predominantly sensory neuropathy. Only 88 (21.3%) subjects were electrophysiologically examined, and the influences of other neuropathies could not be ruled out due to the lack of a control group. Of these, 30% had sensory neuropathy, and 7.3% had motor components (of a sensorimotor type) as well. The difference between our study and the previous study might be due to the different metabolisms and nutritionalstatuses of our study’s adolescents, and influences of chronic diseases and injuries in Rahman’s study. A study in Alaska, conducted among 147 adults aged less than 60 years, showed no dose-response relationship between arsenic ingestion and peripheral neuropathy (21). Of the six subjects with symptoms or physical findings suggestive of sensory neuropathy, NCVs of five subjects were normal. The authors concluded that ingestion of arsenic from well-water does not result in clinical or sub-clinical neuropathy. The study could not exclude the effects of chronic diseases and daily injuries of the adult on sensory neuropathy. These diseases might mask mild changes induced by chronic arsenic exposure. The study also emphasized the importance of placebo control, because the subjective symptoms and neuropathy with other aetiologies would make a false-positive conclusion. The electrophysiological study may be more scientific than subjective symptoms for identifying the presence of chronic arsenic neuropathy. Although arsenic biotransformation and toxicology have been well-documented in many aspects, the mechanisms of chronic arsenic-induced peripheral neuropathy are still unclear. Although there have been animal studies exploring the changes in the central nervous system and neurotransmitters as a result of arsenic exposure (26), no studies have been conducted on acute or chronic peripheral neuropathy. Several reports indicate that arsenic-related neuropathy is developed under an acute high-dose exposure. Lack of nerve demyelination in chronic exposure to arsenic may also suggest different neuropathy-producing mechanisms compared to those from acute arsenic intoxication. Methylation of inorganic arsenic is regarded as the major metabolic pathway in humans (27). It may produce intermediate metabolites, such as monomethylarsonic acid [MMA(III)], which is quitetoxic but has a short half-life. The final metabolites—monomethylarsinic acid [MMA(V)] and dimethylarsinic acid [DMA(V)]—are less toxic than inorganic arsenic (28,29). Methylation may also increase the excretion from urine and has been considered for many years to be a detoxification mechanism (30). According to the result of a scatter-plot of the cumulative dosage of arsenic exposure and sural SAP NCV (Fig.), the sural SAP NCV decreases with the increase of cumulative dosage of arsenic exposure. In addition, the increasing tendency was not statistically significant (β=-0.0013 and p=0.1749). However, the study subjects with a cumulative dosage of arsenic exposure greater than 100.0 mg had a statistically significant 2.9-fold risk of slow conduction velocity of sural SAP compared to the reference group (Table 3). It might imply the non-linear effect of arsenic exposure on the toxicity of sural SAP. In addition, our study also found a higher toxicity of arsenic on NCV due to high-dose and long-term intake of arsenic, showing a borderline statistical significance of odds ratio of 7.8. Based on these findings, we suggest that long-term arsenic exposure could induce the risk of slower sensory NCV, especially the NCV of sural SAP. Since different pathways and arsenic exposure indices might induce a variable severity of arsenic-related neuropathies, and the smaller sample size might lead to wider 95% confidence intervals, further investigations and larger samples are necessary to elucidate the different clinical presentations and mechanisms of chronic arsenic peripheral neuropathy. Acknowledgements The study was supported by grants [no. NSC89-2314-B-038-060; no. NSC90-2320-B-038-044; and no. NSC92-2321-B-038-011] from the National Science Council, Executive Yuan, Republic of China. References
© 2006 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn06023t3.jpg] [hn06023t4.jpg] [hn06023t1.jpg] [hn06023f1.jpg] [hn06023t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}