 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
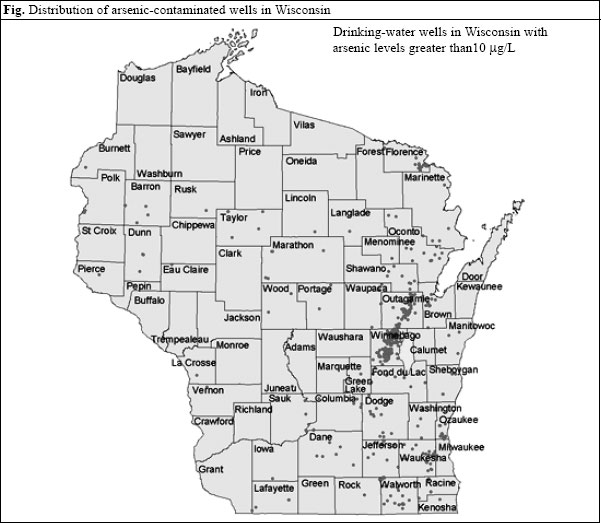
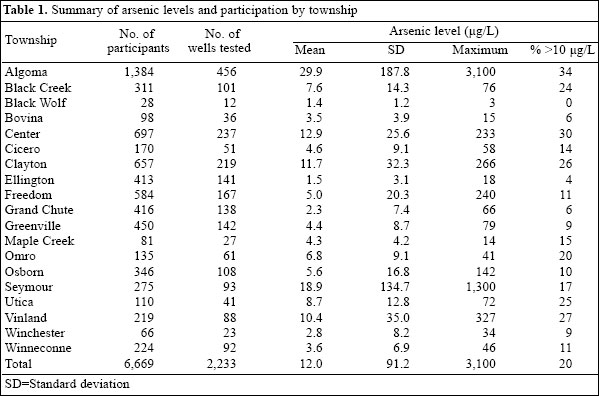
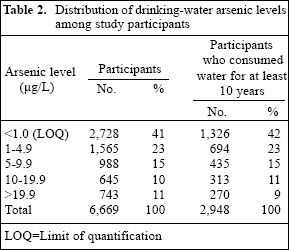
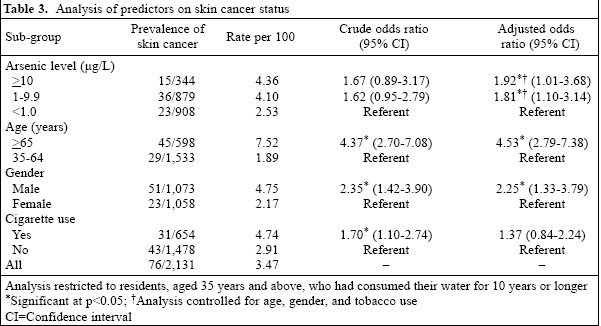
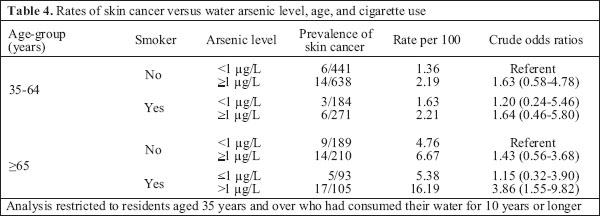
Journal of Health, Population and Nutrition, Vol. 24, No. 2, June, 2006, pp.206-213 Association of Arsenic-contaminated Drinking-water with Prevalence of Skin Cancer in Wisconsin's Fox River Valley Lynda M. Knobeloch1, Kristina M. Zierold2, Henry A. Anderson1 1Wisconsin Department of Health and Family Services, Bureau of Environmental Health, Madison, WI 53702, USA and 2Department of Environmental Health Sciences, Arnold School of Public Health, University of South Carolina, Columbia, SC, USA Correspondence and reprint requests should be addressed to: Dr. Lynda Knobeloch Wisconsin Department of Health and Family Services 1W Wilson St., Room 150 Madison, WI 53702 USA Email: knobelm@dhfs.state.wi.us Fax: (608) 267-4853 Code Number: hn06025 Abstract During July 2000-January 2002, the Wisconsin Division of Public Health conducted a study in 19 rural townships. A high percentage of private drinking-water wells in these townships contained traces of arsenic. Residents were asked to collect well-water samples and complete a questionnaire regarding residential history, consumption of drinking-water, and family health. In total, 2,233 household wells were tested, and 6,669 residents, aged less than one year to 100 years, provided information on water consumption and health. The well-water arsenic levels ranged from less than 1.0 to 3,100 µg/L. The median arsenic level was 2.0 µg/L. The arsenic levels were below the federal drinking-water standard of 10 µg/L in 80% of the wells, while 11% had an arsenic level of above 20 µg/L. Of residents aged over 35 years, those who had consumed arsenic-contaminated water for at least 10 years were significantly more likely to report a history of skin cancer than others. Tobacco use was also associated with higher rates of skin cancer and appeared to synergize the effect of arsenic on the development of skin cancer. Key words: Arsenic; Skin neoplasms; Tobacco; Cross-sectional studies; United States Introduction Since the 1990s, concern over the health effects resulting from arsenic exposure has increased worldwide. Inorga-nic arsenic, frequently found in groundwater supplies in the United States, is a well-known human poison clas-sified as a human carcinogen by the World Health Orga-nization (1) and the United States Environmental Protec-tion Agency (EPA) (2). Long-term ingestion of conta-minated drinking-water increases the risk of basal and squamous cell cancers of the skin and has been linked to tumors of the bladder, kidney, liver, and lung (3-6). Additionally, exposure to inorganic arsenic may cause thickening and discolouration of the skin (7-9), nausea and diarrhoea (10), decreased production of blood cells (11,12), abnormal heart rhythm (13), blood-vessel damage (14), and numbness in the hands and feet (15,16). More recently, arsenic exposure has been associated with the development of diabetes mellitus (17,18). While many of these studies have shown positive associations between exposure and disease, most have focused on arsenic levels of above 20 µg/L. Prior to 2001, the maximum contaminant level (MCL) for arsenic in drinking-water was 50 µg/L. However, the EPA recently lowered this standard to 10 µg/L and has required all public water supplies to comply with this standard by 2006. In 1987, a groundwater study, conducted by the Wis-consin Department of Natural Resources (DNR), identi-fied a large vein of arsenic-rich sulphide minerals in a bedrock layer found at the interface of the St. Peter Sandstone and Sinnippee Dolomite. This formation stretches from southern Brown county into Outagamie and Winnebago counties and lies beneath more than 20,000 private water-supply wells (Fig.). Water sam-ples collected from 1,943 private wells during 1992-1993 contained arsenic concentrations ranging from less than 2 µg/L to 15,000 µg/L. Nearly 20% of these water sup-plies contained concentrations that exceeded the new federal drinking-water standard of 10 µg/L (19). A 1992-1993 study found that residents whose water intake pro-vided an estimated arsenic dose of >50 µg/day were significantly more likely to report a diagnosis of skin cancer than others (20). Recent water-quality testing indicates that arsenic levels in this aquifer are increasing. This trend appears to correlate with withdrawal of regional groundwater and may involve the introduction of oxygen and chlorine disinfectants into the aquifer (21,22). Some experts have expressed concern that this trend could create a regional shortage of potable water. One of the greatest challenges facing public-health officials is convincing families to monitor arsenic levels in their private wells and to follow water-use advisories. Families whose drinking-water contains arsenic con-centrations of above 10 µg/L are advised to seek an alternative supply of water for drinking and cooking. The principal objective of this research was to evaluate the prevalence of skin cancer, cardiovascular diseases, and other illnesses in families that use water from pri-vate wells located within the advisory area. The correla-tion between arsenic exposure and the prevalence of chronic diseases among these families has been pub-lished previously (23). Materials and Methods Measurements of arsenic During July 2000-January 2002, 19 townships in Winne-bago and Outagamie counties sponsored well-water testing programmes. Home-owners were encouraged to submit a well-water sample to the local town hall for analysis. For a small fee ranging from 15 to 20 dollars, the well-water samples were analyzed for arsenic. In total, 2,849 families representing 10-35% of the house-holds in each township submitted water samples. All samples were acidified prior to analysis and were un-filtered due to concerns that iron-bound arsenic would be removed by filtration. A certified laboratory conducted arsenic analyses according to the method 3113B (SM). Total arsenic was determined using graphite furnace atomic absorption. The limit of detection and limit of quantifation were 1 µg/L and 3 µg/L respectively. Approximately, one month after turning in their well-water samples, home-owners were invited to an infor-mational meeting at the local town hall. During this meeting, they received the results of their well-water tests and were given the opportunity to discuss their test results with state experts on water quality. Questionnaire The Wisconsin Division of Public Health, Bureau of Environmental Health, USA, developed a questionnaire that was used for examining residential history, consumption of drinking-water, use of a water-treatment system, and family health. The questionnaire was distributed with the water-sample kits. Families were instructed to sign a consent form, complete the questionnaire, and return it to the town hall along with their water samples. Thus, the questionnaires were returned before the home-owners received the results of water-arsenic analyses. Within the 19 participating Wisconsin townships, 2,233 families comprising 6,669 individuals completed the questionnaire. This represented 78% of the 2,849 families that participated in the well-water testing programme. Water arsenic levels were similar among participants in the health survey and others. Of the study participants, 20% had a well-water arsenic level of ≥10 µg/L. This percentage was essentially the same at 20.7% among the 2,849 water-test results. Measures Cancer status: To determine the cancer status, partici-pants were asked whether they had ever been diagnosed with cancer (Y/N) and were asked whether they had been diagnosed with cancer since they moved into their current home (Y/N). Those who answered 'yes' to either question were asked to provide information regarding the type of cancer, the year of diagnosis, and their age at diagnosis. Arsenic exposure: For the analysis, the exposure variable was divided into three exposure categories: arsenic levels of <1.0 µg/L, 1.0-9.9 µg/L, and >10 µg/L. Predictor variables: Other variables analyzed as possible factors associated with cancer included gender (M/F), age (35-64 vs >64), and smoking status (Y/N). Statistical analysis Data from the surveys were analyzed using SAS (ver-sion 8.2); (Cary, NC). Only those persons who were ex-posed to their well-water for 10 or more years were in-cluded in the analysis. To examine the individual effects of the independent predictor variables, simple logistic regression, modelling each independent variable on can-cer status, was used for calculating crude prevalence odds ratios (ORs) and 95% confidence intervals (CIs). To evaluate the effects of several predictor variables on cancer status, multivariate logistic regression was used for calculating adjusted odds ratios (AOR) and CIs. Results Of the 6,669 individuals, 51% were male and 49% were female. Their age ranged from less than one year to 100 years (mean=37 years; standard deviation [SD]=21.8). Of those who were aged 18 years and above, men were more likely to report a history of past or current cigarette use than women (33% vs 22%). The residents reported drinking water from their wells from less than one year to 83 years (mean=11.5 years; SD=11). Although informa-tion on race and ethnicity was not collected, most par-ticipants were non-Hispanic Caucasians. According to the 2000 U.S. Census, approximately 94% of residents living in the Outagamie and Winnebago counties re-ported their race/ethnicity as non-Hispanic white. Arsenic findings In total, 2,849 wells were tested in the 19 townships, and 2,233 families returned the family-health question-naire with their water samples. Table 1 summarizes the arsenic levels in the water samples provided by the families that returned health questionnaires. The total number of participants, the mean, standard deviation, and maximum of arsenic concentrations, the number of wells tested, and the percentage of wells that had an arsenic concentration greater than 10 µg/L are shown for each township. Overall, 920 (41%) of the wells that were sampled contained no detectable arsenic, and 866 (39%) wells contained an arsenic concentration between 1 µg/L and 9.9 µg/L. Twenty percent (n=447) of the water samples contained an arsenic concentration equal to or greater than the current EPA standard of 10 µg/L (Table 2). Arsenic exposure and skin cancer For the purpose of evaluating the effect of arsenic expo-sure on the prevalence of skin cancer, our analysis was restricted to 2,131 people who were aged 35 years or over and consumed water from the tested wells for at least 10 years. None of these families treated water to remove arsenic. Thirty-one percent of these individuals reported a history of tobacco use. The majority (57%) had a detectable level of arsenic in their well-water, and 34% had an arsenic level of >5 µg/L. One hundred eighteen people reported a diagnosis of skin cancer. These included three people aged less than 35 years and members of 111 different families. The youngest persons to report a history of skin cancer were a 30-year old man and two women aged 30 and 34 years. These individuals were unrelated and lived in homes with low arsenic levels at the time of their par-ticipation in our survey. The overall rate of skin cancer among people aged over 34 years was 3.0% (115/3,828). This rate was essentially the same among people whose current drinking-water supplies had arsenic levels below 1.0 µg/L (2.6%), between 1 and 9.9 µg/L (3.4%), and above 9.9 µg/L (3.1%). Because skin cancer is a disease found primarily in middle-aged and older adults, people aged less than 35 years were eliminated from our analysis. In addition, since chemically-induced cancers normally appear after several years of exposure, our analysis was limited to adults who had consumed water from their tested wells for at least 10 years and did not have a water-treatment system in their homes. These restrictions, which were planned during the design of the survey, were intended to increase our ability to evaluate the effect of long-term exposure to arsenic-contaminated water by reducing the chances of exposure misclassification. We reasoned that, to see an effect of chronic exposure to arsenic on the prevalence of cancer, it was essential to limit our cohort by removing people whose primary drinking-water sources over the previous 10 years had not been tested for arsenic content. The rate of skin cancer was 3.47% among 2,131 peo-ple, aged 35 years and above, who had consumed their water for at least 10 years (Table 3). This rate varied with age, gender, history of cigarette use, and arsenic level of drinking-water. Residents whose water samples contained a detectable level (≥1 µg/L) of arsenic were more likely to report a diagnosis of skin cancer than others. The results of multivariate logistic regression controlling for smoking status, age, and gender indicate that adults whose well-water samples contained arsenic concentrations ranging from 1.0 to 9.9 µg/L were nearly twice as likely to report a diagnosis of skin cancer than adults whose well-water samples contained less than 1.0 µg of arse-nic per litre (AOR=1.81, 95% CI 1.10-3.14). Adults whose well-water samples contained an arsenic concentration of . ≥10 µg/L reported the highest rate of skin cancer. These residents were significantly more likely to report skin cancer than those whose water-arsenic levels were <1.0 µg/L (AOR=1.92, 95% CI 1.01-3.68). As shown in Table 4, arsenic exposure seemed to en-hance the effect of smoking on skin cancer risk. Among adults aged over 64 years, the rate of skin cancer was lowest among non-smokers whose well-water contained no detectable arsenic (4.76 per 100). Among non-smo-kers whose well-water arsenic levels exceeded 1 µg/L, the rate of skin cancer increased by 40% to 6.67 per 100. Among smokers, the rates of skin cancer increased three folds from 5.38 to 16.19 per 100 as the arsenic level in their drinking-water increased from <1.0 to ≥1.0 µg/L. Discussion This study is the largest epidemiological study relating to contaminated drinking-water that has ever been con-ducted in Wisconsin. It was initiated to evaluate arsenic exposure and prevalence of cancer among residents of several townships in Wisconsin's Fox River Valley. These townships overlie a bedrock aquifer that is known to be affected by arsenic-bearing sulphide minerals. Our finding of higher skin cancer rates among people who had long-term exposure to arsenic-contaminated water is consistent with the 1999 Report of the National Re-search Council on Arsenic in Drinking Water (24) which summarized skin-cancer mortality studies conducted by Chen et al. (25), Chen and Wang (6), and Wu et al. (5). None of these studies assessed the incidence of non-fatal skin cancers, however. We are unaware of any other US studies that have evaluated incidence of skin cancer in populations exposed to low levels of arsenic in water. Since skin cancer is not a reportable illness and rarely results in death in the US, it cannot be tracked using state or national databases. Assessment of incidence of skin cancer requires a population survey or a review of patient-records that are not readily available to re-searchers. Wisconsin recently began to collect diagonstic and treatment data from outpatient departments. It is hoped that this new electronic database will facilitate tracking of skin cancer and other chronic illnesses. Our finding that the effect of arsenic on incidence of skin cancer was more pronounced among current and past cigarette-smokers is novel and merits additional in-vestigation. The use of tobacco products has been shown to increase the risk of squamous cell carcinoma. In a recent study conducted by the Leiden University Medical Centre, the relative risk of squamous cell carcinoma was 2.0 among smokers vs non-smokers after adjustment for age, sex, and sun exposure (26). Tobacco use was not associated with a higher risk of basal cell carcinoma, however. The cross-sectional design used in this study had im-portant weaknesses and unique strengths. Diagnoses of skin cancer were self-reported and were not confirmed by reviewing medical records. Skin cancer is not a re-portable diagnosis in Wisconsin, so there are no registries that can be reviewed to confirm self-reported diagnoses. It seems likely that most people would remember a pre-vious diagnosis of skin cancer. However, few people in our study were able to provide specific information on the type of skin cancer, i.e. squamous vs basal cell cancer. The health-related questionnaire was returned by 78% of the families that provided water samples for testing. Since completion of the questionnaire was voluntary, it is likely that some families may have participated in the health study because they were concerned about arse-nic exposure or existing health problems. This bias is un-avoidable in studies that rely on voluntary participation, but is unlikely to have affected our findings since the study participants were unaware of their water test results at the time they completed their health-related question-naire and could not have anticipated the interaction we observed between history of smoking and arsenic expo-sure. In addition, because skin cancer is easily treated, it may be less likely to motivate participation in an environmental health study than a more serious health problem. The questionnaire used in this study did not request information on occupation or sun exposure, so we were unable to control for this well-known risk factor. Sun exposure may partially explain the higher rates of skin cancer we observed among men since men are more likely to work outdoors than women. While it is unlikely that sun exposure would be differentially associated with individual well-water arsenic levels, controlling for sun exposure might have improved our ability to evaluate the effects of arsenic exposure. It is plausible that expo-sure to ultraviolet radiation which damages DNA might have increased the risk of skin cancer posed by arsenic, which is thought to promote tumour growth by inhibit-ing DNA repair (27). Research that evaluates the com-bined effects of arsenic, sun exposure, and cigarette use on the incidence of skin cancer would be very interesting. Despite these weaknesses, our study was able to see an effect of arsenic on human skin cancer. Our success is likely due to a relatively large sample size, collection and review of water-consumption and tobacco-use his-tories for each individual, and arsenic analysis of well-water from each household. By limiting our analysis to people who had consumed water from the tested well for at least 10 years, we were able to refine our exposure assessment and ensure that the exposures were long-term. Collection of information on tobacco use is standard in most studies of human cancer, but we did not antici-pate an interaction between tobacco use and arsenic ex-posure in the occurrence of skin cancer. If we had not collected information on water-consumption times and tobacco use from each individual in our study, our find-ings could have been negative. The inability to control for exposure time and tobacco use in ecological studies makes them less useful for assessing the health impacts of exposure to water that contains traces of arsenic. Findings of this investigation support the need to reduce long-term exposure to arsenic-contaminated drinking-water. All private well-owners in Wisconsin are advised to test their water for arsenic. In some areas, periodic testing may be advisable, since arsenic levels can change over time. Arsenic levels have been found to increase gradually following installation of a new well. This effect is thought to be the result of oxidation of sul-phide minerals due to aeration of the aquifer. Ground-water data of Wisconsin Department of Natural Resources contain many wells that show an increasing arsenic con-centration over time. Dramatic changes in the arsenic level in two wells were observed following repeated chlorination to control iron bacteria. In one of these cases, the arsenic level increased from <5 µg/L to 1,200 µg/L over a period of a few weeks. The release of arsenic following oxidation is accompanied with a drop in pH and release of other metals, such as zinc, lead, and nickel. In regions where arsenic-bearing bedrock exists, special well-construction codes may be needed to reduce the risk of contamination of drinking-water. Our observation of higher rates of skin cancer among consumers of water that contained arsenic levels below the new federal standard of 10 µg/L supports the need for additional health studies. Research that focuses on aging populations that have had continuous, long-term exposure to water that contained arsenic levels ranging from 1 to 20 µg/L would be especially helpful in establishing a safe level of exposure to this common groundwater contaminant. Acknowledgements This work was supported by a grant from the Wisconsin Groundwater Coordinating Council. References
© 2006 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn06025f1.jpg] [hn06025t1.jpg] [hn06025t4.jpg] [hn06025t3.jpg] [hn06025t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}