 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health, Population and Nutrition, Vol. 24, No. 2, June, 2006, pp.214-220 Levels of Arsenic in Drinking-water and Cutaneous Lesions in Inner Mongolia Xiaojuan Guo1,2, Zhiyao Liu3, Chenping Huang1, Lingui You4 1Department of Preventive Medicine, School of Public Health, Wenzhou Medical College, Wenzhou City, Zhejiang 325035, China, 2Department of Clinical Epidemiology, Institute of Industrial Ecological Sciences, University of Occupational and Environmental Health, Kitakyushu City, Japan, 3Inner Mongolia Medical College, Hohhot city, China, and 4Inner Mongolia Center for Endemic Disease Control and Research, Hohhot City, China Correspondence and reprint requests should be addressed to: Dr. Xiaojuan Guo Professor, Department of Preventive Medicine School of Public Health Wenzhou Medical College, China Chashan High Education Area Wenzhou City Zhejiang Province 325035 China Email: juan@med.uoeh-u.ac.jp Fax: +86-577-8668-9122 Code Number: hn06026 ABSTRACT The most common health effects from drinking-water containing dissolved arsenic are skin abnormalities and lesions that are typically diagnosed as keratosis and pigment disorder. It was previously reported that the prevalence of cutaneous lesions was about 44% in arsenic-affected villages. However, there has been little research on the relationship between levels of arsenic in drinking-water and cutaneous lesions in Inner Mongolia. One study examined the association between the prevalence of keratosis and levels of arsenic exposure and the relationship between pigment disorder and levels of arsenic exposure among villagers aged 18 years or older in the arsenic-affected village of Hetao Plain in Inner Mongolia, PR China. The study included 227 participants who were affected by cutaneous lesions and 221 participants who were not affected by cutaneous lesions diagnosed in 1996 and 1998. Well-water drunk by the participants was collected to analyze arsenic content. Adjusting for age, sex, and smoking, logistic regression was applied to calculate the risks that arsenic in drinking-water will lead to cutaneous lesions. The results from the logistic regression showed that, with the increase of arsenic concentration in water, the risk of pigment disorder also increased (odds ratio [OR]=5.25, 95% confidence interval [CI] 1.32-83.24 for 50-199 µg/L; OR=10.97, 95% CI 1.50-79.95 for 200-499 µg/L; OR=10.00, 95% CI 1.39-71.77 for ≥500 µg/L (p=0.000), but the association between risk of keratosis and levels of arsenic was not significant (p=0.346). The findings suggest that keratosis is an early feature of arsenic poisoning, and the development of pigment disorder depends on higher doses of arsenic intake rather than keratosis. Further studies are needed to confirm that cutaneous lesions and other adverse health effects occur at low levels of arsenic exposure. Key words: Arsenic; Drinking-water; Cutaneous lesions; Inner Mongolia; China Introduction Arsenic is an ubiquitous element in nature. Contamination of water can occur naturally when arsenic-rich ores leach into ground and surface water (1). Chronic ingestion of water with high concentrations of arsenic cause adverse health effects to human beings. Keratosis, hyperpigmentation, and depigmentation are the most common cutaneous lesions and play important roles in the diagnosis of arsenic poisoning (2-5). Furthermore, cutaneous lesions are often viewed as useful precursors of severe diseases such as skin cancer (6). Some epidemiological studies have estimated the relationship between levels of arsenic and cutaneous lesions (7,8). Tondel reported that, among people in Bangladesh with cutaneous lesions, the mean concentration of arsenic in drinking-water was 640 µg/L, while for those without any cutaneous lesions the mean concentration of arsenic was only 21 µg/L (range 0-740 µg/L) (9). In addition, Valentine et al. surveyed groups of 20-57 residents in six cities of the United States where concentrations of arsenic in drinking-water ranged from 0.5 to 395 µg/L. No significant differences in the prevalence of dermal or neurological symptoms were detected among any groups studied (10). Since 1990, there have been some wells with high levels of arsenic in some areas in Inner Mongolia, China. One of our surveys in 1996 indicated that up to 26% of wells or other water sources in the Hetao plain area of Inner Mongolia had arsenic concentrations that were equal to or higher than 50 µg/L with the highest arsenic level being 1,354 µg/L. More-over, the prevalence of cutaneous lesions was 44% (11). Some patients had the symptoms of keratosis, while others had both keratosis and pigment disorder (hyperpigmentation and depigmentation). However, there have not been sufficient epidemiological studies clarifying the relationship between the level of arsenic exposure in drinking-water and cutaneous lesions in the area. The main objective of the present study was to determine whether the prevalence of various cutaneous lesions was associated with levels of arsenic exposure. Materials and Methods Study population
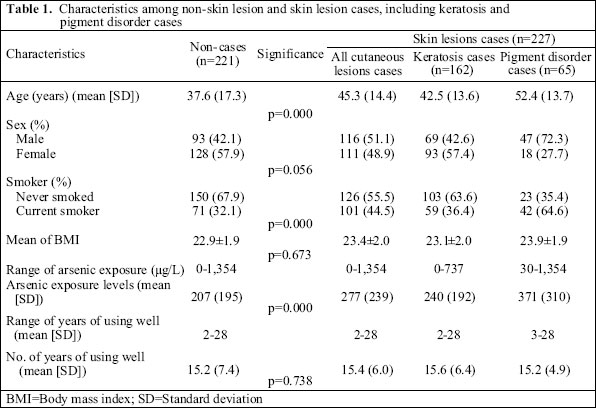
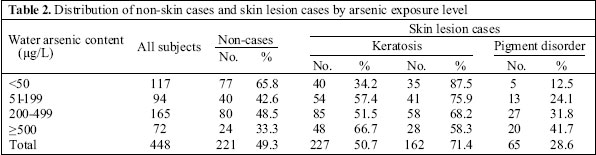
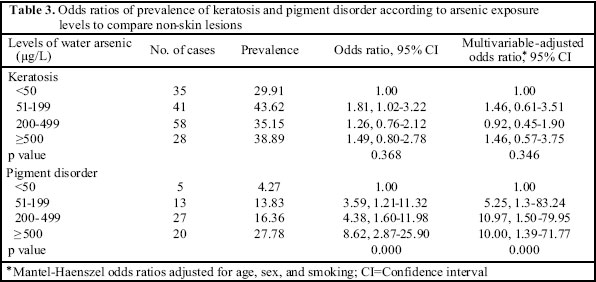
As part of the Asia Arsenic Network’s (AAN) Investigation and Strategy of Inner Mongolia Arsenic-contaminated Program 1996-2000, a preliminary survey was conducted between 1996 and 1998 in Wuyuan county of Inner Mongolia. In this survey, 66 of the 679 villages were found to be affected by arsenic (levels of arsenic in drinking-water >50 µg/L), while the permitted standard of arsenic in drinking-water is 50 µg/L in China. One of the 66 arsenic-affected villages was selected as the study area due to cooperation from the local government and the heterogeneity in exposure, enabling the investigators to collect exposure-response data. The village’s main source of income comes from agricultural employment, and there are no other industries or mining activities around the village. Until the 1970s, four public open-shallow wells (depth approximately 3-5 m) were used for drinking-water. From the 1980s onwards, the villagers turned to private tubule-type wells (depth approximately 15-30 m) due to reasons relating to hygiene. The concentrations of arsenic in water in the village ranged from non-detectable doses to a dose of 1,354 µg/L. According to the registered records of the local government office of Wuyuan county, the total number of inhabitants in the village was 662,589 (89%) of the total number of residents who were in the arsenic-affected village at the time they participated in our study. Most of them were engaged in agricultural work. After the officials from the local government explained the purpose of the study, residents were asked to participate. All subjects signed an informed consent form before being interviewed. Interviews and cutaneous examination All participants were given standardized sets of questionnaire during face-to-face interviews in their homes. The questionnaire included finding out information about the participants’ residential history, sociodemographic conditions, sources of water at each residence, duration of using tubewell, amount of water consumed daily, occupation, working conditions, and health-related lifestyle habits, such as smoking and alcohol consumption. After the interviews, subjects were also invited to undergo a skin examination by a dermatologist from Inner Mongolia Medical College. The dermatologist made a diagnosis of skin lesions for every subject. At the time of skin examination, the dermatologist did not know any information about the participants. To reduce observation bias, the same dermatologist and the same interviewer examined all the subjects. According to diagnostic criteria in China (12), there were two kinds of skin symptoms that appeared in the subjects of this study. These were keratosis lesions and keratosis with pigment disorder lesions which included hyperpigmentation and depigmentation. Patients who only had hyperpigmentation or depigmentation and patients who had skin cancer were not discovered. Many villagers have remained asymptomatic despite drinking water contaminated by arsenic for many years. Of 589 participants available for the study, 448 were selected on the basis that they were aged ≥18 years. One hundred forty-one individuals were excluded because they were children who ate and drank mostly at school, except during the weekend. Analyses of arsenic levels in well-water At the time of investigation, the geological team collected samples from all wells in the village. In total, 106 samples were collected from households using drinking-water wells. Water samples were stored in a cool container with an ice block and transported to the laboratory at the Institute for Water Research in Bayanaoer League, Inner Mongolia. The samples were analyzed to assess the total concentration of arsenic using Ag-DDC analysis. Each sample was assayed three times, and the mean value was used. Statistical analysis To evaluate the relationship between various cutaneous lesions and levels of arsenic in water, the prevalence of keratosis and pigment disorder was calculated separately. According to the endemic arsenic region criterion of 1994 in China, arsenic-contamination levels in water were classified into four categories (13): secure level (<50 µg/L), low level (50-199 µg/L), middle level (200-499 µg/L), and high level (≥500 µg/L). According to this criterion, levels of arsenic in water in this study were categorized as follows: <50, 50-199, 200-499, and ≥500 µg/L . Logistic regression analyses were performed to estimate odds ratios and their 95% confidence intervals for each level of arsenic detected among the subjects. Factors, such as sex, age, and cigarette-smoking were adjusted as the confounding factors because they varied among participants. Hence, the score test for a trend test of odds of calculations was performed using a Mantel-Haenszel odds ratio adjusted for age, sex, and smoking by the StataSE 8 for Windows. Results Table 1 shows descriptive characteristics of the 448 subjects surveyed in the arsenic-affected village. Compared to subjects without skin lesions, subjects with cutaneous lesions were older and were more likely to be male. The average age for subjects without skin lesions was 37.6 years; for subjects with keratosis, the average age was 42.5 years; for subjects with pigment disorder (p=0.000), the average age was 52.4 years. The proportion of males without skin lesions was 42.1% , while the proportion of males in the cutaneous lesions group was 51.1% (42.6% for keratosis and 72.3% for pigment disorder). The proportion of current smoking in subjects without skin lesions and those with cutaneous lesions was 32.1% and 44.5% respectively (p=0.000). The body mass indices were similar (22.9, 23.1, and 23.9 kg/m²) in three groups. Levels of concentration of arsenic in water ranged from undetectable to 1,354 µg/L in the village. An increase in average values of arsenic exposure was indicated (p=0.000) from 207 µg/L (among subjects without skin lesions), 240 µg/L (among subjects with keratosis) to 371 µg/L (among subjects with pigment disorder). Subjects without skin lesions and subjects with cutaneous lesions were similar in regard to the mean number of years that they had been using the wells (15.2 years for subjects without skin lesions, 15.6 years for subjects with keratosis, and 15.2 years for subjects with pigment disorders) (p=0.738). Table 2 presents the distribution of subjects without cutaneous lesions and subjects with cutaneous lesions by arsenic exposure level. The ratios of cutaneous lesions increase from 34.2% for arsenic levels less than 50 µg/L to 66.7% for arsenic concentrations of ≥500 µg/L. There were 35 subjects with keratosis and five subjects with pigment disorder among 117 villagers whose water supply had an arsenic concentration of <50 µg/L. Among villagers who drank water containing more than 50 µg/L of arsenic, the results showed that there were: 41 subjects with keratosis and 13 subjects with pigment disorders for arsenic levels of 50-199 µg/L; 58 subjects with keratosis and 27 subjects with pigment disorder for arsenic levels of 200-499 µg/L; and 28 subjects with keratosis and 20 subjects with pigment disorder for arsenic levels of ≥500 µg/L. These results indicated that higher doses of arsenic was associated with a higher prevalence of skin lesions, especially pigment disorder. A significant relationship was not noted between arsenic content and the risk of keratosis (Table 3). The odds ratios of keratosis were 1.81 (95% CI 1.02-3.22) for arsenic levels of 50-199 µg/L, 1.26 (95% CI 0.76-2.12) for arsenic levels of 200-499 µg/L, and 1.49 (95% CI 0.80-2.78) for arsenic levels of ≥500 µg/L compared to levels of arsenic less than 50µg/L. After adjusting for sex, age, and smoking, the odds ratio was 1.46 (95% CI 0.61-3.51), 0.92 (95% CI 0.45-1.90), and 1.46 (95% CI 0.57-3.75) respectively. The levels of arsenic in well water were significantly associated with the prevalence ratios of pigment disorder (Table 3). Compared to arsenic levels of less than 50 µg/L, the odds ratios of pigment disorder were 3.59 (95% CI 1.21-11.32) for arsenic levels of 50-199 µg/L, 4.38 (95% CI 1.60-11.98) for arsenic levels of 200-499 µg/L, and 8.62 (95% CI 2.87-25.90) for arsenic levels of ≥500 µg/L. The sex-, age- and smoking-adjusted odds ratios were 5.25 (95% CI 1.32-83.24), 10.97 (95% CI 1.50-79.95) and 10.00 (95% CI 1.39-71.77) (p=0.000) respectively. Discussion
The most common health effects from drinking-water containing dissolved arsenic are cutaneous abnormalities and lesions.Typically, these cutaneous abnormalities and lesions are diagnosed as keratosis and pigment disorder, including hyperpigmentation and depigmentation. The objective of this study was to determine the dose-response relationship between arsenic in drinking-water and cutaneous lesions and whether there was difference between arsenic concentration in subjects with keratosis and subjects with pigment disorder. Our study in the arsenic-affected village found that 162 subjects had keratosis, and 65 subjects had both pigment disorder and keratosis, while there were no subjects with only hyperpigmentation or depigmentation. The results are consistent with a previous medical investigation exploring other arsenic-affected villages in Inner Mongolia (14). Previously, we examined 260 people in an arsenic-affected village and discovered that 100 participants had keratosis, and 64 participants had pigment disorders and keratosis lesions, while no participants had only pigment disorders. It was, therefore, suspected at the time that keratosis might be an early feature of arsenic poisoning. Similar reports are scarce, except for a study by Centeno who emphasized that arsenical keratosis is a common characteristic of arseniasis in a study of pathology relating to chronic arsenic exposure (15). Studies conducted in other countries have also investigated the prevalence of cutaneous lesions and arsenic concentration in regions where drinking-water has elevated arsenic levels. Foy reported that keratosis was recognized in children whose exposure to arsenic was 200 µg/L in Thailand (16). The study of Chakraborty revealed that high amounts of arsenic in well-water were associated with keratosis and hyperpigmentation in five arsenic-affected regions of India. Of 784 exposed individuals, 25% had keratosis or hyperpigmentation. The mean drinking-water arsenic concentration among those with cutaneous lesions was 640 µg/L (range 200-2,000 µg/L) (17). In the present study, the range was 0-1,354 µg/L. Thus, the mean arsenic concentration in cutaneous lesions group (277 µg/L) was lower than that found in the study in India. Nevertheless, arsenic concentration in water drunk by most subjects with keratosis ranged from 50 µg/L to 499 µg/L, and arsenic concentration in water drunk by most participants with pigment disorder ranged from 200 µg/L to 500 µg/L or over. Previous studies concerning the dose-response relationship between arsenic and cutaneous lesions have been reported (5,18). However, the analysis of the relationship between keratosis and arsenic levels and between pigment disorder and arsenic levels has rarely been conducted separately. Yu et al. reported that depigmentation occurs in advanced stages of arsenic poisoning, and keratosis is a later feature of arsenical dermatosis (19). The results of our study showed that the prevalence of pigment disorder indicated statistically significant dose-response relationship, and the association was not apparent in keratosis lesion. In terms of potential confounding factors, nutritional status and smoking have been reported to increase susceptibility to arsenic poisoning (20,21). In the present study, body mass index as a crude indicator of nutritional status was calculated, and no difference was found in normal subjects, subjects with keratosis, and subjects with pigment disorders. Furthermore, the difference between the rich and the poor was very small in the area. Despite the lack of information on potential confounders other than age, sex, and smoking, the strong association supported the relativity: the adjusted prevalence ratio was 10.0 (95% CI 1.39-71.77).Thus, it is likely that the arsenic exposure level in an individual with pigment disorder is higher than in an individual with keratosis, and keratosis is an early and common feature of arsenism. The mechanism for arsenic-related hyperpigmentation and depigmentation remains elusive. One reason why pigment disorder is different may be that the effects of arsenic on pigment disorder risk might be modified by genetic or constitutional and geographical factors, such as cutaneous colour and sun-sensitivity. On the other hand, different diagnostic criteria have been used in each country and area, leading to the variance of case detection for keratosis and pigmentation. For instance, while keratosis is characterized by a bilateral thickening of the people’s palms and soles in Bangladesh (19), the character of keratosis is raised on the palms and soles of people in Inner Mongolia (14). We also found 35 subjects with keratosis and five subjects with pigment disorder who drank water containing arsenic of <50 µg/L. In India, four patients with keratosis and seven patients with hyperpigmentation whose main source of drinking-water contained <50 µg/L of arsenic were also identified (22). Recently, the question of whether low level of arsenic concentrations is associated with any health effects has become an important focus on arsenic exposure. Further epidemiological studies are needed to focus on the adverse health effects on people who have been exposed to low levels of arsenic. There are some limitations to this study. First, we only used concentration of arsenic in water to evaluate exposure levels. However, it is difficult to procure and calculate accurately the data of water consumption for each individual. Second, the duration of exposure to arsenic might be a confounding factor. Kosnettemphasized three perspectives: clinical perspective, public-health perspective, and sub-clinical perspective. The development of hyper-pigmentation depends on the dose of arsenic intake. If a person ingests more than 0.04 mg/kg body-weight/day for six months to three years, there is a chance to develop hyper-pigmentation (23). Most participants in our study started using tubule-type wells as a water source in the 1980s, and usually their drinking-water sources had not changed over a long period. Thus, apart from children and a few newcomers to the village, the villagers have been using the well consistently over a long period of time. In conclusion, this study found that the prevalence of keratosis was higher than pigment disorder. A clear exposure-response relationship between the prevalence of pigment lesions and the levels of arsenic was shown. However, there was no significant association between the risk of keratosis and the levels of arsenic (p-trend=0.346). The findings suggest that keratosis is an early feature of arsenism and that the development of pigment disorder depends on a high intake of arsenic. Although the level of arsenic exposure is low in the wells of some subjects, we also found that some of these subjects had cutaneous lesions. Further studies are needed to confirm the adverse health effects among populations with low levels of arsenic exposure. Acknowledgements This study was supported by the globe environment fund of Japan and Asian Arsenic Network. The authors thank the Wuyuan County Government for supporting the field survey. The authors also thank the staff members of the Station for Hygiene Prevention from Wuyuan county in Inner Mongolia, Department of Clinical Epidemiology, Institute of Industrial Ecological Sciences, University of Occupational and Environmental Health, and the Japan Inner Mongolia Arsenic pollution study group for their assistance. References
© 2006 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn06026t1.jpg] [hn06026t3.jpg] [hn06026t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}