 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
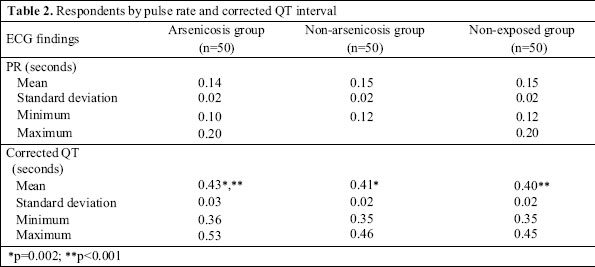
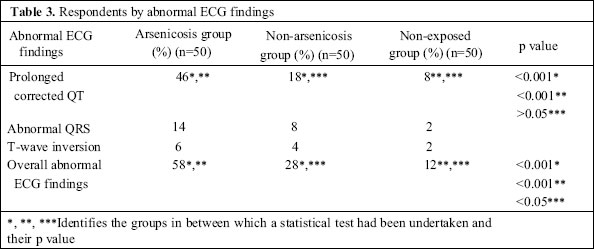
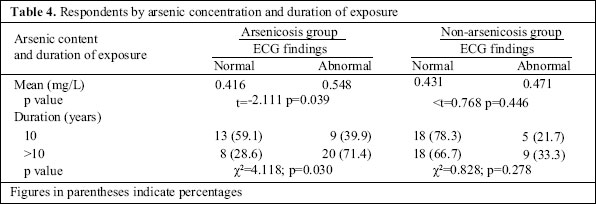
Journal of Health, Population and Nutrition, Vol. 24, No. 2, June, 2006, pp. 221-227 Electrocardiographic Abnormalities among Arsenic-exposed Persons through Groundwater in Bangladesh Sk. Akhtar Ahmad1, Fatema Khatun1, M.H. Salim Ullah Sayed1, Manzurul Haque Khan1, Md. Rashed Aziz2, Mohammed Zakir Hossain3, M.H. Faruquee4 1Department of Occupational and Environmental Health, National Institute of Preventive and Social Medicine, Mohakhali, Dhaka 1212, Bangladesh, 2Department of Cardiology, Dhaka Medical College Hospital, Dhaka 1000, 3Planning Unit, Directorate General of Health Services, Mohakhali, Dhaka 1212, and 4Asia Arsenic Network, Dhaka Correspondence and reprint requests should be addressed to: Prof. Sk. Akhtar Ahmad Professor and Head Department of Occupational and Environmental Health National Institute of Preventive and Social Medicine Mohakhali, Dhaka 1212 Bangladesh Email: anon@bdcom.com Code Number: hn06027 ABSTRACT This study was carried out among arsenic-exposed and non-exposed people of Bangladesh to assess and compare their cardiac status based on electrocardiographic (ECG) findings. For the purpose of the study, participants were included in three groups: arsenic-exposed persons with arsenicosis (arsenicosis group), arsenic-exposed persons without arsenicosis (non-arsenicosis group), and persons not exposed to arsenic (non-exposed group). Each group included 50 respondents. In this study, no significant difference in heart rate, rhythm, axis, and pulse rate interval was detected among the arsenicosis, non-arsenicosis and non-exposed groups. A significant difference in corrected QT interval between the arsenicosis and the non-exposed group (p<0.05) was observed. On the contrary, no statistically significant difference in corr-ected QT interval between the non-arsenicosis and the non-exposed group was found. Abnormal QRS complex was found among 14%, 8%, and 2% of the arsenicosis, non-arsenicosis, and non-exposed groups respectively. ECG findings, indicative of left ventricular hypertrophy, ischaemic heart disease, andright bundle branch block, were high among the arsenicosis group. Overall, abnormal ECG findings were high (58%) among the respondents of the arsenicosis group and were highly significant (p<0.001). The findings revealed that there was a significant association between ECG abnormalities and arsenic exposure. Key words: ECG; Corrected QT interval; QRS complex; Left ventricular hypertrophy; Ischaemic heart disease; Arsenicosis; Arsenic; Arsenic exposure; Cross-sectional studies; Bangladesh Introduction Tubewells have been used in Bangladesh since the 1940s. During the early days, the vast majority of rural people collected their drinking-water from surface-water sources, such as ponds and rivers. As the water from these sources was not bacteriologically safe, a large number of children and adults died each year from waterborne diseases. Consequently, with the aim of providing safe water to the vast population of Bangladesh, tubewells were installed. About 10 million tubewells (hand-pumps) had been sunk until recently in Bangladesh, which provided 97% of its population with access to safe water. Unfortunately, the identification of arsenic in tubewell water in 1993 gave rise to a new dilemma. Since the initial detection of arsenic contamination in groundwater in Bangladesh, it has rapidly emerged as a major public-health problem. Arsenic contamination in tubewell water has become evident in 61 of the 64 districts of the country. The Bangladesh Arsenic Mitigation and Water Supply Project (BAMWSP) has so far screened tubewells in 271 of 490 upazillas (sub-districts). Of 4,946,933 tubewells, located in 57,482 villages of these upazillas, 29.2% were arsenic-contaminated (>0.05 mg/L). And in 8,540 villages, more than 80% of the tubewells were arsenic-contaminated. Moreover, 38,118 patients with arsenicosis were detected in 255 upazillas. The situation so far uncovered is considered as the tip of the iceberg, and with the passage of time, the size of the population exposed, the number of patients detected, and the complications of arsenic exposure continue to evolve (1-4). Long-term arsenic exposure above the safe level of 50 µg/L (for Bangladesh) leads to the development of arsenicosis, which is characterized by the appearanceof characteristic skin manifestations (melanosis and or keratosis). Other manifestations often present include weakness, conjunctival congestion, chronic cough, chronic bronchitis, peripheral neuropathy (tingling, numbness, burning sensation, and pain), etc. In additionto complications, such as non-pitting oedema (pedal oedema), chronic ulcer of keratosis, peripheral vascular disease (gangrene), hepatopathy, nephropathy, Bowen`s disease, cancer, particularly squamous cell andbasal cell carcinoma, adverse pregnancy outcomes, dia-betes mellitus, and hypertension, may occur. Many of these effects and complications among arsenicosis patients in Bangladesh have already been reported (5-9). Cardiovascular effects of chronic arsenic exposure have been documented in some studies. A considerable increase in the prevalence of peripheral vascular disease and cardiovascular diseases among patients with chronic arsenic poisoning has been reported in Taiwan,Chile, Japan, Germany, and Sweden (10,11). An association between drinking arsenic-contaminated waterby mothers and congenital heart disease was also found in a study (12). In Bangladesh, an association between arsenic in drinking-water and occurrence of hypertension was reported rather recently (8). Various ECG abnormalities, such as QRS complex broadening, prolonged QT intervals, ST segment depressions, T-wave flattening, and even ventricular tachycardia, had been observed among cases of acute arsenic poisoning and in acute promyelocytic leukaemia patients treated with arsenic trioxide (13-17). This makes it likely that individuals exposed to excess arsenic through drinking-water could show some of these ECG abnormalities. However, in Bangladesh so far, no published reports referring to electrocardiographic (ECG) abnormalities in persons exposed to arsenic through drinking-water are available. This study was, thus, undertaken at the community level to explore if people who were chronically exposed to arsenic (>0.05 mg/L) through drinking tubewell water had ECG abnormalities in excess of those having little (<0.05 mg/L) or no arsenic exposure, and to assess whether such abnormalities were more common among those having clinical manifestations of arsenicosis than those having exposure but no arsenicosis. Materials and Methods Study design and area This was a cross-sectional study with comparison groups.The study was conducted in two selected arsenic-contaminated villages (Samta of Sharsa upazila and Marua of Chaugacha upazila under Jessore district) where levels of arsenic in tubewell water were above 0.05 mg/L (the Bangladesh standard). For the comparison group (i.e. non-exposed group), areas (Horiadi of Kapasia upazila and Kuriadi of Sreepur upazila under Gazipur district) were selected purposively where arse-nic content in tubewell water was 0.01 mg/L or less. Study population and sample size The study population comprised persons aged 25-60 years. Those diagnosed having cardiac ailments, hypertension, or taking any medications that could influence ECG findings were not included in the study. Parti-cipants were selected in three groups. The arsenicosis group and the non-arsenicosis group comprised persons who had been exposed to arsenic through drinking arse-nic-contaminated tubewell water (>0.05 mg/L) for at least two years, but the groups differed by the presence or absence of clinical manifestations of arsenicosis. The non-exposed group (reference group) comprised respondents who had been drinking arsenic-safe water (≤0.01 mg/L). In calculating the sample size, we used the formula, n=z2pq/d2, where z is the z-score and d (acceptable level of error) and p and q are anticipated population proportions of exposed and non-exposed groups. As available literature did not provide any estimate of anticipated prevalence rates, prevalence was taken as 0.5 for p and q to provide the largest sample. Using the above formula and modalities (z=1.96, p=q=0.5, and d=15%), the required sample size for each group was 43. The sample size was inflated by an arbitrary figure of 7 as a check against possible drop-outs; thus, the possible sample size for each group was 50. The total sample size was (50x3) 150. Data collection Researchers enlisted individuals fulfilling the criteria for inclusion in the study through house-to-house visits and selected the required number of respondents by simple random sampling. Subsequently, researchersused a pre-tested combined structured questionnaire and a checklist to interview selected respondents. At the beginning of interview, the purpose of the study was explained to each prospective respondent, and hisor her verbal consent to participate in the study was obtained. Two expert technicians performed ECG exa-minations after proper preparation of subjects. Two cardiologists independently interpreted ECG tracings and did not have any information of the group status of participants. The difference in opinion of the two cardio-logists in the interpretation of the ECG tracings was resolved by a third cardiologist. To determine the exposure to arsenic through tubewell water and duration of using particular tubewells, the recorded database in the Department of Occupational and Environmental Health of the National Institute of Preventive and Soc-ial Medicine (NIPSOM) was used. Cases of arsenicosis were diagnosed by having a history of prolonged ingestion of tubewell water with arsenic above the safe dose (0.05 mg/L) for at least six months and manifested by characteristic skin lesions of melanosis and/or keratosis with or without involvement of internal organs. Results Table 1 shows the mean age, monthly income, sex, and level of education of the respondents in the arsenicosis, non-arsenicosis and non-exposed groups. No statistically significant differences in sociodemographic characteristics, in terms of age, sex, and monthly income, were found among the groups (Table 1). The majority of the respondents in all the groups was farmers (35.3%) and housewives (36.7%). About 44.7% of the respondents had the habit of smoking, and no significant difference in smoking-habits was found among the respondents of the three groups. Concentration of arsenic in tubewell water consumed by the arsenicosis and non-arsenicosis groups varied from 0.10 mg/L to 0.80 mg/L. About 74.0% of the respondents in the exposed groups (arsenicosis and non-arsenicosis) had been drinking tubewell water containing arsenic >0.3 mg/L. The mean concentration of arsenic in tubewell water used by the respondents in the arsenicosis and non-exposed arsenicosis groups was 0.493±0.215 mg/L and 0.443±0.162 mg/L respectively, but the difference was not statistically significant (t=1.246; p=0.216). Moreover, 56% of the respondents in the arsenicosis group and 54% in the non-exposed arsenicosis group had been drinking arsenic-contaminated water for more than 10 years. Among the respondents in the arsenicosis, non-arsenicosis and non-exposed groups, the mean systolic pressure was 131.1±11.3, 123.8±12.3, and 120.0±13.3 mm of Hg respectively, while the mean diastolic pressure was 84.1±8.2, 80.3±8.1, and 75.7±7.8 mm of Hg respectively. The mean systolic and diastolic press-ures of the respondents in the arsenicosis group were statistically higher than those in the non-arsenicosis (p<0.05) and non-exposed groups (p<0.001). Between the respondents of the non-arsenicosis and the non-exposed group, only diastolic pressure was statistically different (p<0.05). The ECG tracings revealed that the mean heart rate of the respondents in the arsenicosis, non-arsenicosis, and non-exposed groups was 80.0±12.9, 80.6±17.0, and 82.9±14.4 per minute respectively, and the difference in the mean heart rate between the groups was not statistically significant (p>0.05). Most (99.3%) res-pondents in all the groups had regular heart rate andnormal P-wave. The PR interval and mean corrected QT interval for the respondents in the arsenicosis, non-arse-nicosis, and non-exposed groups are shown in Table 2. Prolonged corrected QT interval (normal interval 0.35-0.43 seconds) was found in 46% of the respondents in the arsenicosis group, and it was significantly higher compared to that of the respondents in the non-arsenicosis (p<0.01) and non-exposed groups (p<0.001). The difference in the proportions of having prolonged corr-ected QT intervals between the non-arsenicosis (14%) and the non-exposed group (8%) was not statistically significant (p=0.06) (Table 3). Abnormal QRS complex was a more common occurrence among the respondents in the arsenicosis groups (14%) than among the respondents in the non-arsenicosis (8%) and non-exposed (2%) groups (Table 3). In the arsenicosis group, among those (n=7) having abnormal QRS complex, about 71% (5) had changes, indicative of left ventricular hypertrophy (LVH). Moreover, QRS complex changes, indicative of RBBB (28.6%), was also found. Of four (8%) respondents in the non-arsenicosis group having abnormal QRS complex, two had LVH, and two had RBBB. Only one (2%) had LVH in the non-exposed group. T-wave inversion, indicative of ischaemic heart disease, was found among 6% (3), 4% (2), and 2% (1) of the respondents in the three groups respectively (Table 3). The ST segment was elevated in 4% (2) of the respondents in the arsenicosis group, depressed in 2% (1) in the non-arsenicosis group. However, no ST segment abnormality was found among the respondents in the non-exposed group. Axis deviation was observed in two (4%) cases in the arsenicosis group (one had left axis and the other one had right axis deviation). In the non-arsenicosis group, none had axis deviation, whereas in the non-exposed group, only one had left axis deviation. There was a significant association among overall abnormal ECG findings (prolonged corrected QT, abnormal QRS complex, T inversion, axis deviation, etc.) in the arsenicosis, non-arsenicosis, and non-exposed groups(χ2=24.79; p<0.001). Overall, abnormal ECG findings were observed in the arsenicosis group in higher percentage (58.0%). In the non-arsenicosis group, the abnormal ECG finding was found in 28.0% of the respondents, while in the non-exposed group, it was 12.0%. The differences in the proportion having abnormal ECG findings between the arsenicosis and the non-arsenicosis group, and between the arsenicosis and the non-exposed groups were highly significant (p<0.001), but it was just significant (p<0.05) between the non-arsenicosis and the non-exposed groups (Table 3). The mean concentration of arsenic in tubewell water used by those having normal ECG findings was 0.426 (±0.191) mg/L, and in contrast, the mean concentration of arsenic for those having abnormal ECG findings was 0.523 (±0.180) mg/L, and the diffe- rence was statistically significant (t=-2.597; p=0.011). Among the respondents in the arsenicosis group, the mean arsenic concentration in tubewell water used by those having abnormal ECG findings was higher than that used by those having normal ECG findings, and the difference was statistically significant (t=-2.111; p=0.039). In the non-arsenicosis group, no such diffe-rence was observed (t=0.768, p=0.446). A significant association between duration of exposure (>10 years) and abnormal ECG finding was observed in the arsenicosis group (χ2=4.118; p=0.030), but no such association was found in the non-arsenicosis group (χ2=0.828; p=0.278) (Table 4). In relation to smoking-habit, no significant relationship of ECG findings was observed between and within the groups. On further analysis using sequential binary logistic regression to examine the relationship between the ECG status and the arsenicosis and non-arsenicosis groups, the association was significant (χ2=19.929; p=<0.001; odds ratio=3.432, 95% confidence limit 1.416-8.32) after removing the effect of duration of exposure and arsenic concentration. Moreover, the arsenicosis andnon-arsenicosis groups could significantly predict 72.0% of the overall ECG findings with 65.1% of the abnormal and 77.2% of the normal ECG status. During examining the relationship between concentration of arsenic in tubewell water and the ECG status after adjustment for the effect of arsenicosis and non-arsenicosis groups and the duration of exposure, it was observed that the mean difference of arsenic concentration between normal and abnormal ECG status remained significant (p=0.021) and, on average, respondents with an abnormal ECG status had 0.097 mg/L higher concentration of arsenic than respondents with a normal ECG status. Discussion In this cross-sectional study, we compared ECG findings among arsenic-exposed persons with signs of arse-nicosis (arsenicosis group), arsenic-exposed persons without sign of arsenicosis (non-arsenicosis group), and persons not exposed to arsenic (non-exposed group). The groups were comparable in terms of age, sex, income, and level of education, as these variables did not differ statistically. The mean PR intervals for the different groups were almost similar. Among the respondents in thearsenicosis group, the PR interval varied from 0.10 to 0.20 second, and in the non-arsenicosis and non-exposed groups, it was the same (0.12 to 0.20 second). Among the arsenicosis group, PR was significantly higher (0.43 second) than that found among the respondents in the non-arsenicosis (p<0.01) and non-exposed groups (p<0.001). Among the respondents in the non-arsenicosis and non-exposed groups, the mean corrected QT intervals were 0.41 and 0.40 second respectively. In the current study, a higher prevalence of ECG abnormalities among individuals having exposure to arsenic (≥0.1 mg/L) through their drinking-water (tubewell water) was detected. A significantly high prevalence of prolonged corrected QT interval and abnormal QRS complex was found among respondents having arsenicosis compared to those of the non-arsenicosis and arse-nic non-exposed groups (Table 3). ECG evidence of ischaemic heart disease, left ventricular hypertrophy, and RBBB was more common among the arsenic-exposed groups than among the reference group. Ischaemic heart disease was far more common in the arsenicosis group than in other groups. The relationship between mortality due to ischaemic heart disease and long-term arsenic exposure was previously reported from Taiwan (18). Various signs or symptoms of cardiovascular diseases were observed by Hotta in a study (11) carried out in a small population of Toroku (Japan) having environmental and occupational exposure to arsenic. Of them, 53.6% had abnormal ECG findings. ECG abnormalities, such as QRS prolongation, ST depression, T-wave flattening, QT prolongation, etc., had been observed among patients with acute arsenic poisoning and in those treated with arsenic trioxide (13-17). Prolonged corrected QT interval was found among 50-68% of patients who were treated by arsenic trioxide for acute promyelocytic leukaemia (14,17). The findings of this study indicate that arsenic exposure through drinking-water in Bangladesh could give rise to cardiac toxicity and pathology evident through ECG abnormalities. Moreover, those having arsenicosis were more vulnerable, and the higher thelevel of arsenic and duration of exposure, the more likely it is to find ECG abnormalities. Acknowledgements The authors wish to express their gratitude to all the respondents of the four villages for their kind cooperation and responses. They also express gratitude to Dr. Sanjoy Sarker, Register, Cardiology Department of Dhaka Medical College Hospital and Dr. Jayonta Kumar Poddar, Consultant, Cardiology, Sadar Hospital Jessore, for their active participation of ECG interpretation. References
© 2006 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn06027t4.jpg] [hn06027t3.jpg] [hn06027t2.jpg] [hn06027t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}