 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
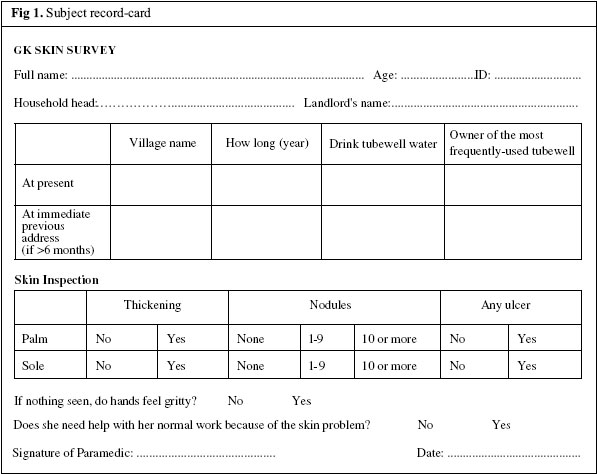
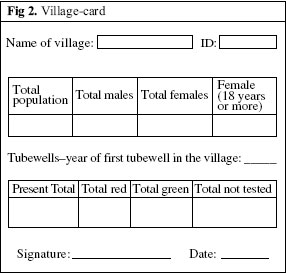
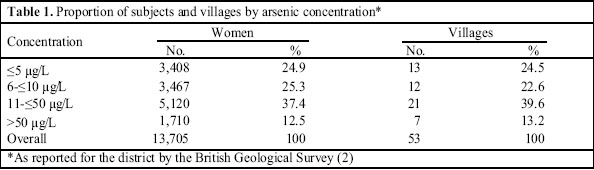
Prevalence of Arsenic-related Skin Lesions in 53 Widely-scattered Villages of Bangladesh: An Ecological Survey Corbett McDonald1, Rezaul Hoque2, Nazmul Huda3, Nicola Cherry4 1Department of Occupational and Environmental Medicine, National Heart and Lung Institute, Imperial College, London, UK,2 Gonoshasthaya Kendra, Nayarhat, Savar, Dhaka, Bangladesh, 3Institute of Child and Mother Health, Matuail, Dhaka, and 4Department of Public Health Sciences, University of Alberta, Edmonton,Canada Correspondence and reprint requests should be addressed to: Prof. N. Cherry Department of Public Health Sciences Faculty of Medicine and Dentistry University of Alberta 13-103 Clinical Sciences Building Edmonton, Alberta T6G 2G3 Canada Email: ncherry@ualberta.ca Fax: (780) 492-967 Code Number: hn06028 ABSTRACT A survey was carried out to provide a representative assessment of prevalence and risk of arsenic-related skin lesions in relation to geographical distribution of arsenic in wells of rural Bangladesh as a necessary background for research into effects in pregnancy and cancer risks. A systematic random sample of 53 villages in four divisions of Bangladesh served by Gonoshasthaya Kendra was selected, and all women aged 18 years or more (n=16,740) were listed. Trained paramedics recorded the presence of skin thickening and nodules on the palms and soles, together with information on tubewell use. The prevalence was related to the mean concentration of arsenic for the district as indicated by data from the British Geological Survey and to the date the first well in the village was installed. Overall, the observed prevalence was 176 cases (1.3%) in 13,705 women examined, varying from 0% in 26 villages to 23% in one; lesions were observed more frequently on hands than on feet. The estimate doubled with concentrations of arsenic from 11 to ≤50 μg/L and increased more than 20 times at >50 μg/L. In the absence of further information, priority for control measures should be directed at areas where the average concentrations of arsenic are above 50 μg/L, especially in villages where skin lesions have been identified. Key words: Skin lesions; Arsenic; Arsenic exposure; Prevalence; Bangladesh Introduction Inhaled or ingested arsenic is a human carcinogen and skin pathogen (1). The guideline for arsenic in drinking water specified by the World Health Organization (WHO) is 10 μg/L, and the permissible level by the Government of Bangladesh is 50 μg/L. Extensive studies by the British Geological Survey (BGS) (2), over a three-year period, 1998-2000, reported that levels of arsenic far in excess of 50 μg/L were commonly found in water from tubewells in the southern half of the country and in some areas of the north. The source of arsenic and, indeed, of several other potentially-toxic metallic elements, such as boron and manganese, is natural sedimentation into the Ganges Delta by water pouring down over millennia from the Himalayas. The use of tubewell water in southern Asia began some decades ago as it was virtually free from pathogenic organisms. Tubewells are now used as a source of drinking-water by most households in the innumerable villages of rural Bangladesh, with perhaps half the population of the country exposed to a potentially grave hazard from arsenic. The full extent of effects on health of arsenic in drinking-water is, however, quite unknown. Limited epidemiological studies have been reported in recent years mainly from West Bengal where much the same environmentalsituation prevails and a few studies also from Bangladesh (3-7). Typical arsenical skin lesions (keratosis, thickening) on the hands and feet, with resulting disability and some evidence of malignant change, have been reported from villages known to have high arsenic exposure, but no data from Bangladesh are yet available on potentially more serious risks, such as lung and bladder cancers, and effects on the foetus. Major difficulties for epidemiological research lie in the quantification of exposure intensity and in the enormous geographical variation in concentrations of arsenic in well-water, even within the same village (2). For skin lesions, and more certainly for cancer, many years of exposure are required (7). The number of tubewells has steadily increased, from relatively few in the 1960s to an estimated 10 millions or more today (2). Although the geographical boundaries of average concentrations obtained by the BGS are reasonably well-defined, in three villages studied in detail by the BGS, the highest levels in each were three orders of magnitude greater than the lowest. To record reliably from which wells, and for how long, any individual has taken drinking-water is close to impossible, with little evidence of how concentrations may have changed over time, even from the same well. It is not surprising, therefore, that the recently-published study of Haque et al. from West Bengal, India, the first reported study from this region designed specifically to assess exposure-response, was limited by several acknowledged assumptions (7). Nothing similar has yet been reported from Bangladesh. For a country with limited resources, the magnitude of this ecological disaster would be daunting even if an economically feasible method of control were known. Research plan and objectives In the past 35 years, Gonoshasthaya Kendra (GK) (8), a non-governmental organization, has provided comprehensive primary healthcare to the entire population of nearly a million residents in over 600 villages scattered throughout four of six divisions of Bangladesh. Basic demographic data are recorded and are periodically updated for all residents by paramedics who have ready access and visit frequently. Information routinely recorded includes all pregnancies with outcome and all known deaths, with suspected causes. In common with other official health providers, GK needs to know the level of risk from arsenic in the villages for which they are responsible. GK is perhaps the largest NGO providing healthcare, covered for the most part by pre-paid universal insurance and by grants from international donors such as DANIDA. Their paramedics, mostly young women, are well-trained and highly regarded by other NGOs and official services, for both of which they provide staff. GK is, thus, uniquely well-placed to investigate toxicity of arsenic over a diverse geographical area with a wide range of arsenic concentrations in well-water, putting in context published reports from selected areas often chosen for their elevated arsenic levels. Because of the great difficulty in determining levels and duration of arsenic exposure in rural Bangladesh, a programme of epidemiological research was planned, in collaboration with GK, to proceed step by step. The first phase, a wide prevalence survey of keratotic skin lesions on the hands and feet, was needed to determine whether or not these changes were significantly related to exposure as provided by published data from the BGS (2). This phase has two parts: the first, reported below, is based on a large population of adult women in widely-scattered villages. Women rather than men were selected because they were believed to have a simpler pattern of well-use than men, who often work away from home. In addition, a detailed study of prevalence among the male and female population of all ages in two large villages, where skin lesions were said to be common, has been completed and is awaiting analysis. Finally, a detailed case-control study is in progress, based on cases identified in the prevalence studies, with current concentrations of arsenic measured in wells normally used. In all these surveys, the question of diagnosis of arsenic-caused disease was deliberately avoided, with preference instead given to defined lesions as illustrated in standard photographs. This may eventually allow us to describe the range of clinical characteristics, particularly of early lesions as related to level of arsenic exposure. Depending on findings from these surveys, studies of pregnancy outcome will be analyzed retrospectively and prospectively in these same villages. Later, we hope to study deaths thought to be due to lung and bladder cancers throughout the GK network, using a validated system of verbal autopsy. Materials and MethodsStudy sites and subjects Fifty-six villages were selected by systematic random sampling from all listed in each of four administrative divisions (Barisal, Chittagong, Dhaka, and Rajshahi) of Bangladesh stratified roughly in relation to population. In the remaining two divisions (Khulna and Sylhet), GK has no villages under its network. In each of the selected villages, women aged 18 years or above were identified in January 2004 from the GK lists of all residents. In February, the paramedics normally responsible for each village were brought together in Savar for a two-day training course on completion of record-cards and practical demonstration of skin lesions and on how they should be classified. The workload for the study was assessed for each village, and in some where the number of subjects exceeded 500 for one paramedic, a ‘para’, or defined portion of the village, was chosen randomly for investigation. The field survey was conducted during April-October 2004. Field work To carry out the survey, the paramedic visited the home of each woman on the administrative list created by GK for that village. After explaining the purpose of the visit, and with her permission, the paramedic examined the palms and soles (washed, if indicated) of each woman and recorded the presence and number of characteristic nodules, of thickening, ulcers and, where no other lesion was detected, a feeling of ‘grittiness’ on the margin of the palms. These were recorded on a standard card (Fig. 1) in Bangla, together with age and details of tubewell-use in the present and immediately previous residence (if any). Where a woman was temporarily away from home, the paramedic made repeated visits to carry out the examination. If a woman listed in the administrative records had died, moved away (for marriage or work), proved to be aged under 18 years, or otherwise ineligible,this was recorded and the subject excluded. The paramedic also completed a ‘village card’ (Fig. 2) giving the village population (from GK records) and information about the history of tubewells within the village (from the best available source), together with the total number of wells and the numbers marked red (concentration ≥50 μg/L), green (<50 μg/L), or unmarked. The survey was carried out under the supervision of two physicians (RH, NH) who visited each village frequently during the study and checked on the quality of work; problems were resolved by discussion with NC or CMcD. Completed cards were collected and checked, and data entered electronically for later analysis. Any cards containing errors or omissions were referred back at once to the village paramedic for correction and further checking. Case and exposure definitions Cases were defined as women with one or more nodule(s)or with characteristic thickening on either palm or sole. For analysis of prevalence reported here, no account was taken of ulcers, ‘grittiness’, or reported lesions elsewhere on the body. Our paramedics investigated the number of marked wells but were otherwise uninformed about the level of arsenic in water of their villages. Certainly, neither they nor the authors were aware of the BGS’ classification of the villages until after the field survey had been completed, and the observations of the paramedics were recorded. Arsenic exposure was taken as the mean concentration reported by the BGS for the administrative district in which the village was located [Fig. 4, volume 1, of the BGS report (2)]. Dates of the first well and numbers and marking of wells were those recorded by the paramedic using the village-card.
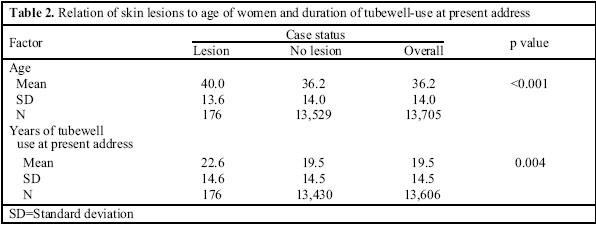
Statistical analysis The approach adopted considered, first, the village as the unit of analysis (using the Poisson regression model) with number of cases as the outcome variable and, second, each subject (in a logistic model) with case status as the outcome variable. In the analysis of villages, the initial multivariate model included concentrations of arsenic, the number of women examined, the year the first tubewell was installed in the village, and the proportion of tubewells marked red. In the analysis of subjects, the initial model included the subject’s age and duration of drinking tubewell water by the village people at the current address. Only variables significant (p<0.05) in univariate or multivariate analyses were included in the final models.
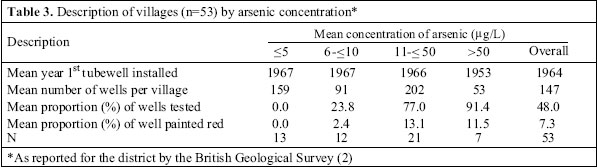
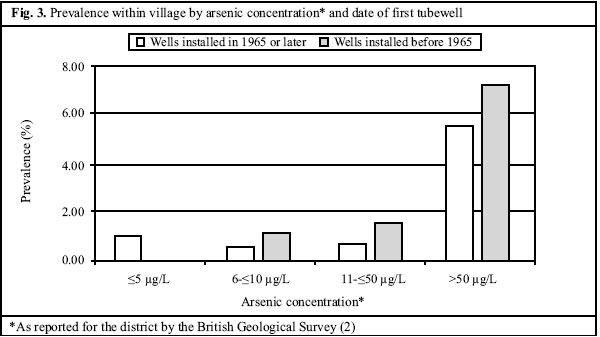
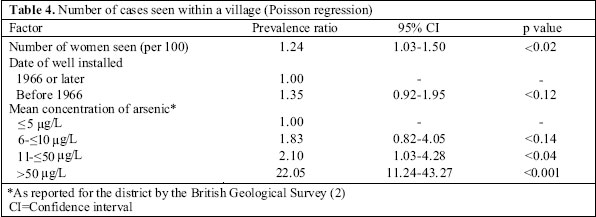
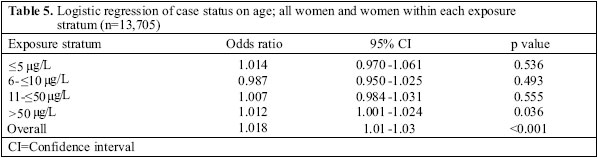
Ethics The study protocol was formally reviewed by the GK Executive Committee. It was also reviewed by the Royal Brompton Hospital, London Ethics Committee. Results Fifty-six villages were identified for inclusion in the study. Of these, three were excluded, where the paramedic who had attended the training course was unable to complete the task, and no trained substitute could be found. In the 53 villages, 16,740 women aged 18 years or over were identified from the administrative lists. Of these, complete examinations were carried out and findings were recorded for 13,705 women; 2,992 women listed had either died, moved from the village, or could not be located during the survey. Another 43 women were located but parts of the skin examination critical to the case definition were not recorded. A village-card was completed for all 53 villages. The women surveyed were distributed fairly evenly among villages in districts with a range of arsenic concentrations reported by the BGS (Table 1). Their mean age was 36.2 years (Table 2). All but 281 women were still drinking tubewell water at the time of the survey, with a mean of 19.5 years of drinking this water at their present address.Nearly three quarters (72.9%) had drunk tubewell water at their previous address, for a mean duration of 10.8 years. The first date at which a tubewell had been installed in the village (Table 3) varied markedly with an unexpectedly early median of 1965. The proportion of wells tested varied from 0% to 100% with the proportion of wells labelled red ranging from 0% to 79%. The skin lesions recorded were more commonly nodules (114 women) than thickening (82 women) and were found more often on the palms (103 women) than on the soles (87 women) with profusion ranging from a single nodule to multiple nodules and thickening on both hands and feet. Overall, 176 (1.3%) of 13,705 women were recorded to have nodules or thickening. The prevalence within the villages ranged from 0% (no cases) in 26 villages to 23.0% (48 of 209) in one village in Feni (Chittagong). The median was 0.22% with only 13 villages having a prevalence of 1.0% or greater. The prevalence of cases was related to the mean concentration of arsenic reported by the BGS. Women in villages with a mean concentration of arsenic of ≤5 μg/L had a prevalence of 0.4% (10 cases), 6-≤10 μg/L 0.4% (16 cases), 11-≤50 μg/L 0.7% (33 cases), and those having greater than 50 μg/L 6.9% (117 cases). The prevalence was also related to the date at which the first well was installed in the village (Fig. 3). No relationship was found between the prevalence of cases and the number or proportion of wells in a village that were labelled red, either when this factor was considered unilaterally or in a multivariate analysis. In an analysis of the number of cases reported in each village, the only factors of importance were the number of women examined in that village and the mean concetration of arsenic in tubewell water (Table 4). Villages in districts with mean concentrations below or equal to 50 μg/L showed a small increase in risk when ≤5 μg/L was used as a reference, but the prevalence increased very substantially (to a rate ratio of 22) for villages in districts with mean concentrations of arsenic above 50 μg/L in tubewell water. With women (rather than village) as the unit of analysis, both duration of tubewell-use at the present address and age were related to lesions (Table 2). However, in a logistic regression analysis including both these factors, only age was related to case status. When an analysis was carried out stratified by concentrations of arsenic, age was related to the detection of lesions only for those living in areas with high concentrations of arsenic (Table 5). Discussion The purpose of the survey was to provide a balanced picture of the prevalence of arsenic-related skin lesions in Bangladesh to complement the broad geographical distribution of arsenic in tubewell water from the extensive information published by the BGS. It is, thus, essentially an ecological study, since lifetime exposures to arsenic on an individual basis were not, and indeed may never be, available. Despite the obvious limitations of the ecological approach, public-health measures are also essentially ecological; so, for this purpose, it provides a more robust base than detailed data based on individual estimates of arsenic intake over time, complicated by uncertain human behavioural variables. Our second objective was to test the feasibility of using this source of information for epidemiological studies of cancer and pregnancy-related risks. Both these objectives appear to have been met reasonably well, and we are now encouraged to believe that it may be possible to undertake further epidemiological studies within the resources of the GK network. It is also reassuring that evidence of excess risk of skin lesions was seldom found in villages in districts where average concentrations of arsenicin tubewell waterwere reported by the BGS as 50 μg/L or less. The latter conclusion must be regarded cautiously, however, especially as arsenic is a cumulative poison, and cases seen to date may only be the first of an approaching epidemic caused by the use of well-water at lower concentrations over many years. Also, while the presence of skin lesions in a community may prove to be a good marker of that community’s risk of arsenic-related malignant disease, this has not been established in Bangladesh or West Bengal, and continued efforts to determine the full cost to health of arsenic in well-water are clearly needed. The high prevalence (6.9%) of skin lesions reported from villages of a high-arsenic district is lower than that reported in previous studies (4,6). This may reflect both levels of arsenic concentration, which may have been up to 500 μg/L in some villages chosen for previous studies and the restricted case definition used in the present study. Guha Mazumder et al. reported a range in prevalence of keratosis by exposure levels in West Bengal (3) that is consistent with the results reported here. The more comprehensive study of Haque et al. in West Bengal found high concentrations in drinking water of both cases (325 μg/L) and controls (180 μg/L) (7), suggesting a setting not comparable with the lower concentrations reported for the large majority of villages in the present study. This study has shown the value of simple, but large-scale epidemiological surveys, conducted by an experienced primary-care network, which are essential if the results of more detailed local research are to be put in proper context. The females, aged 18 years or over, were selected for the present survey because women, less frequently away from home than men, are likely to use fewer wells, although they may move from one village to another when they marry. Paramedics tend to have more contact with women than with men and, in this study, their enquiries and examinations were readily accepted. Other strengths of the survey were large-sized, systematic random sampling by administrative division, well-defined populations of female residents, and well-trained field workers familiar with the women being studied. On the other hand, 53 villages are a minute proportion of the country’s many thousand villages, and none was from Khulna or Sylhet—the first of these being an important deficiency. Also, we tried to supervise and check the quality of the paramedics’work, but we may not always have succeeded. Some indication of this will be obtained from the nested case-control study where all cases and controls were re-examined by one of us (NH), and all lesions photographed for a later panel review. Further analysis combining village and subject data may then better evaluate the true risk of arsenic-related skin lesions. There remains the fundamental question as to the validity of using the extensive but relatively crude average test results of the BGS for the assessment of exposure. Within any village, levels of arsenic are known to vary widely, and individual intake of arsenic may vary to the same extent. It would require estimates of arsenic concentration of all wells used during a lifetime for a sufficient number of residents of scattered villages to improve on the ecological approach. However, group-based assessment of exposure, as in this analysis, has been shown to produce essentially-unbiased estimates of risk (9). Further insight into this question will be obtained from the nested case-control study, in which measurements have been made of water in wells currently in use by each subject. Our results so far suggest that, in the absence of other information, immediate priority should be given to areas of the country where the average concentration of arsenic is above 50 μg/L. Acknowledgements This survey was supported in part by research funds from the Royal Brompton Hospital and was made possible by the hard work of some 60 GK paramedics. The data were coded and entered for analysis by Shafiqul Islam and Kamal Uddin. References
© 2006 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn06028f2.jpg] [hn06028t3.jpg] [hn06028f3.jpg] [hn06028t4.jpg] [hn06028t2.jpg] [hn06028t5.jpg] [hn06028t1.jpg] [hn06028f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}