 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
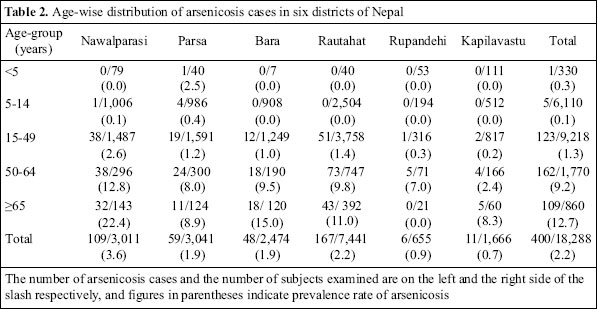
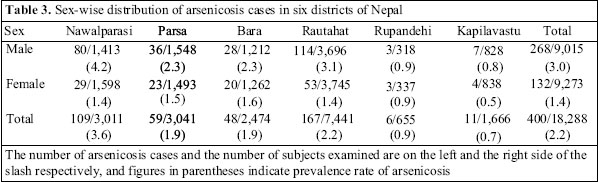
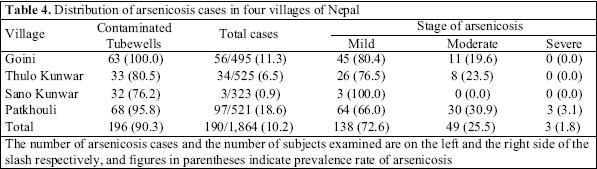
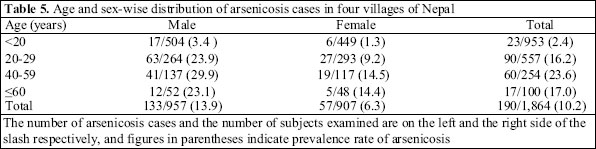
Journal of Health, Population and Nutrition, Vol. 24, No. 2, June, 2006, pp. 246-252 Prevalence of Arsenicosis in Terai, Nepal Makhan Maharjan1, Roshan R. Shrestha1, Sk. Akhtar Ahmad2, Chiho Watanabe3, Ryutaro Ohtsuka4 1Environment and Public Health Organization, New Baneshwor, PO Box 4102, Kathmandu, Nepal,2Department of Occupational and Environmental Health, National Institute of Preventive and Social Medicine, Mohakhali, Dhaka 1212, Bangladesh, 3Department of Human Ecology, School of International Health, Graduate School of Medicine, University of Tokyo, Hongo 7-3-1, Bunkyo-ku, Tokyo 113-0033, Japan, and 4National Institute for Environmental Studies, Tsukuba, Ibaraki Correspondence and reprint requests should be addressed to: Dr. Makhan Maharjan Environment and Public Health Organization (ENPHO) New Baneshwor PO Box 4102, Kathmandu Nepal Email:maharjanmakhan@yahoo.com Fax: 00977-1-4491376 Code Number: hn06030 ABSTRACT This paper summarizes the findings of surveys on arsenicosis cases conducted during 2001-2004 in terai, Nepal, by governmental and non-governmental organizations in their respective project areas and by some national and international institutes. Studies were conducted in six arsenic-contaminated districts of terai, namely Nawalparasi, Bara, Parsa, Rautahat, Rupandehi, and Kapilvastu. In these districts, arsenic contamination in tubewells varied from 2.1% to 25.7%. The prevalence of arsenicosis was, on average, 2.2% and varied from 0.7% in Kapilavastu district to 3.6% in Nawalparasi district. In the community-based study, the highest prevalence (18.6%) of arsenicosis was found in Patkhouli village of Nawalparasi, where 95.8% of tubewells were contaminated with arsenic. The prevalence of arsenicosis was higher in older age-groups (>50 years) of both the sexes. Males suffered more from arsenicosis than females (odds ratio: 2.50, 95% confidence interval 1.80-3.47). Skin manifestations, such as melanosis and keratosis, were the common symptoms of arsenicosis. Most patients were identified in the early or mild stage of the disease. They are expected to recover if further exposure to arsenic could be avoided by providing arsenic-safe drinking-water through intervention measures. Key words: Arsenic; Arsenic contamination; Skin lesions; Melanosis; Keratosis; Arsenicosis; Water supply; Prevalence; Nepal Introduction Nepal, a small land-locked South Asian country, lies between latitude 26º 22’ N to 30º 27’ N and longitude 80º 4’ E to 88º 12’ E. Elevation ranges from 60 to 8,848 metres, including the highest peak in the world—the Mount Everest. It is bounded on the north by Tibet (China), on the east by Sikkim and West Bengal, on the south by Bihar and Uttar Pradesh, and on the west by Uttar Pradesh of India (Fig.). It has roughly a rectangular shape encompassing an area of 147,181 sq km with an average length of 885 km east to west and an average breadth of 193 km north to south. Topographical diversity provides a wide range of climates, differing according to variations in altitude and location. Likewise, annual rainfall differs with seasonal variations depending on the monsoon cycle. Nepal’s landscape is broadly defined by three contrasting physiographic bands, which run in more or less parallel, east to west: lowland terai region in the south; Hill region in the centre and Mountain region in the north (Fig.). The terai region, also called the ‘grainary’ of Nepal, is a low-lying tropical and sub-tropical belt of flat alluvialdeposits stretching along the Nepal-India border that comprises 20 districts with an average width of 29 km. It is the northern extension of the Gangetic Plain and has an altitude ranging from 60 to 310 metre above the mean sea-level. Three major rivers—the Kosi, the Narayani (Gandak River), and the Karnali—feed the region. The terai makes up only 23% of the total land area but accommodates 50% of the total population of the country (1,2). Arsenic contamination in groundwater in Nepal is a new public-health issue. With the identification of massive arsenic toxicity caused by consumption of arsenic-contaminated tubewell water in Bangladesh and in West Bengal, India, arsenic contamination was appre-hended in Nepal, particularly in the terai region having similar alluvial and fertile plain characteristics to those encountered Bangladesh and West Bengal. The Department of Water Supply and Sanitation conducted the first study on arsenic contamination in the eastern terai region of Nepal in 1999, results of which indicated the possibility for arsenic contamination in groundwater of terai (3). Findings of another preliminary study on arsenic contamination in tubewell water in eight terai districts conducted jointly by the Nepal Red Cross Society (NRCS) and the Environment and Public Health Organization (ENPHO) in 2000 revealed the need for a comprehensive study on arsenic contamination in tubewell water to find out the extent of arsenic distribution in southern Nepal. Since then, governmental and non-governmental organizations and some researchers have tested several thousand samples of tubewell water to identify levels of arsenic contamination and have found that 7.4% of tubewells had arsenic concentrations more than the maximum permissible limit (50 µg/L) for Nepal (4). Elevated levels of arsenic in drinking-water and its health effects have been a public-health concern in many Asian countries, including Nepal. Based on the evidence of carcinogenicity from human studies, arse-nic has been recognized as a human carcinogen (5). Chronic exposure to inorganic arsenic causes characteristic skin manifestations due to chronic arsenic toxicity. Cancers of the skin, bladder, kidney, lung, and other organs also occur due to chronic arsenic toxicity (6). The non-carcinogenic effects of chronic arsenic toxicity on the reproductive, neurological, cardiovascular, respiratory, hepatological, nephrological, haematological problems, diabetics, etc. are also reported in various studies (7). Skin manifestations, characterized by pigmentary change and keratosis, have long been considered to be the hallmark, of chronic arsenic toxicity. Several earlier epidemiological studies in Bangladesh (8-9) and India (10) reported manifestations in skin, these were the most common features in populations exposed to arsenic through drinking tubewell water for a long time. Similar findings were also reported from Inner Mongolia, China, and several other countries (11). Although arsenic contents of hundreds of thousands of tubewells in Nepal were reported, so far only a little published information is available which could sufficiently explore the magnitude of health effects due to chronic exposure to arsenic through tubewell water. In this paper, the extent and status of arsenicosis in arsenic-contaminated areas of the terai region, along with findings of some previous studies carried out by several authorities on different occasions, are summarized and presented. Materials and Methods Of the 20 districts in the terai region where 18,635 tube-wells were examined and, on average, arsenic contamination was detected in 7.4% of the tubewells as reported previously (4), comparatively six higher arsenic-contaminated districts were included in this study. The districts are: Nawalparasi, Bara, Parsa, Rautahat, Rupandehi, and Kapilvastu. Investigation of health effects due to chronic toxici-ty of arsenic was also carried out at village level on a total coverage basis in purposively-selected four vill-ages, namely Goini, Thulo Kunwar, Sano Kunwar, and Patkhouli of Nawalparasi district, where water contamination was higher. Water samples from all 217 tubewells of all four study villages with a total population of 2,339, living in 358 households, were examined for arsenic contamination. Arsenicosis cases were identified by observing skin manifestations on the body and by organizing medical camps in different places of the studied villages. The day before organizing each medical camp, all the households of that particular area of the village were informed, and volunteers requested them to visit the camp the next day for clinical examinations. All the villagers visiting the medical camps were examined for asenicosis, and there was no refusal. One of the authors carried out clinical examinations and diagnosis of arsenicosis. Of the total population (n=2,339), 1,864 (79.7%) were included in the study. The villagers who were not exposed to arsenic-contaminated water and those who were not available at the time of the study period were not included in the study. Following the measurement of arsenic contamination level in tubewell water, targeted subjects were clinically examined to identify arsenicosis cases. Nece-ssary information relating to arsenicosis was also coll-ected. Any person showing pigmentary changes, such as hyperpigmentation (melanosis) or hypopigmentation (leucomelanosis) and/or hyperkeratinization (keratosis), with or without other manifestations of chronic arsenic toxicity and having a history of arsenic exposure through water for more than six months, was diagnosed as an ‘arsenicosis’ case. The patients were categorized into three different stages based on clinical manifestations (9) observed on the body, which were as follows: First stage (mild stage): Melanosis, keratosis (mild), conjunctivitis (conjunctival congestion), and bronchitis. Second stage (moderate stage): Depigmentation (leucomelanosis), keratosis (moderate to severe), oedema (non-pitting), peripheral neuropathy, hepatopathy, and nephropathy (early stage). Third stage (severe stage): Hepatopathy and nephropathy (late stage), gangrene of the limbs, pre-cancerous skin lesions, and cancer. Arsenic concentrations in water samples were measured by atomic absorption spectrophotometer (AAS) equipped with a continuous hydride generator in the research laboratory of the Environment and Public Health Organization (ENPHO), Kathmandu, Nepal. Level of arsenic in water samples was determined, foll-owing pre-reduction with 5% (w/v) potassium iodide (KI) and 5% (w/v) ascorbic acid in 10% (v/v) HCl. The accuracy of determination of arsenic in water was ensured by measuring standard reference material (SRM), NIST SRM 1640 with arsenic of 26.67±0.41 µg/kg. The detection limit (DL) of the HG-AAS was 3 µg/L for arsenic in water. The variables, which were common, included geographical distribution, demographic characteristics, types of skin lesion, and stages of arsenicosis cases. Data of these common variables were summarized and analyzed to find out the prevalence of arsenicosis in relation to different demographic characteristics. Surveys for the determination of arsenic contamination in the study areas were organized by the Nepal Red Cross Society (NRCS), Department of Water Supply and Sanitation (DWSS), and Rural Water Supply and Sanitation Support Program (RWSSSP) during 2001-2004. The community-based health surveys were, however, carried out by the Department of Human Ecology, School of International Health of Tokyo University, Japan, Department of Dermatology of University of Miyazaki, Japan, and Department of Occupational and Environmental Health of National Institute of Preventive and Social Medicine (NIPSOM), Bangladesh, in collaboration and coordination with ENPHO and other local institutions during 2002-2004. Results The rate of prevalence of arsenic contamination (>50 ppb) in Nawalparasi, Parsa, Bara, Rautahat, Rupandehi, and Kapilavastu districts of the terai region was 25.7%, 2.3%, 2.4%, 9.7%, 2.1%, and 3.9% respectively (Table 1). Of the total studied population (n=18,288) of the six districts, 9,015, (49.3%) were male and 9,273 (50.7%) were female. Of them, 400 were identified as cases of arsenicosis. The prevalence of arsenicosis in these districts, on average, was 2.2%, but ranged from 0.7% to 3.6% (Table 2). The highest prevalence of arsenicosis was found in Nawalparasi district (3.6%), which was also reported to be a highly arsenic-contaminated district. The prevalence of arsenicosis was lower in Rupandehi (0.9%) and Kapilavastu (0.7%) districts. The prevalence of arsenicosis was higher among people who were aged 50 years and above. In the age-group of 5-14 years, five (0.1%) cases of arsenicosis were repor-ted, and in the age-group of below five years, only one (0.3%) person had arsenicosis. Of the total arsenicosis patients identified in the six districts, 268 (67.0%) were male, and 132 (33.0%) were female. A higher prevalence of arsenicosis was also found among males in all other studied districts, except Rupandehi. A significant association between the prevalence of arsenicosis and sex was recorded (odds ratio [OR]=2.12, 95% confidence interval 1.719-2.619). The prevalence of arsenicosis among males was 3.0%, and it was 1.4% among females. The highest prevalence of arsenicosis was found among males in Nawalparasi district (4.2%) and the lowest prevalence was found in Kapilavastu district (0.8%). The highest prevalence of arsenicosis was found among females in Bara district (1.6%), and the lowest prevalence of arsenicosis was found among females in Kapilavastu district (0.5%) (Table 3). In the community-based studies in four villages (Goini, Thulo Kunwar, Sano Kunwar, and Patkhouli), 1,864 (79.7%) of the total population were examined for skin manifestations. Of the examined subjects, 957 (51.3%) were male, and 907 (48.7%) were female. Of these, 190 were diagnosed as arsenicosis cases with a prevalence rate of 10.2%. The arsenic test results of the water samples revealed that most (90.3%) tubewells of these four villages were highly arsenic-contaminated. The mean arsenic contamination of these tubewells was 604±432 µg/L. The prevalence of arsenicosis was highest (18.6%) in Patkhouli village where 95.8% of tubewells were arsenic-contaminated (>50 µg/L), while none of the tubewells in Goini village was arsenic-safe, and the prevalence of arsenicosis was 11.3%. In Thulo Kunwar village, 80.5% of tubewells were arsenic-contaminated, and the prevalence of arsenicosis was also comparatively less (6.5%). In Sano Kunwar village, the prevalence of arsenicosis was lowest (0.9%), where only three mild arsenicosis cases were found, but 76.2% of tubewells were arsenic-contaminated. The large majority (72.6%) of the identified arsenicosis cases were at the mild stage, 25.5% at the moderate stage, and 1.8% were at the severe stage. The severe cases were found only in Patkhouli village (Table 4). The number of arsenicosis cases was higher among males (13.9%) than among females (6.3%) in the studied villages. The difference was highly significant (OR=2.50, 95% CI 1.80-3.47). Among the different age-groups, the prevalence of arsenicosis was higher (23.6%) in the age-group of 40-59 years, while it was lower (2.4%) in the age-group of <20 years. The highest (29.9%) prevalence was found among males in the age-group of 40-59 years (Table 5). Arsenicosis cases were identified by observing skin manifestations on their body. Among the cases, the most common manifestation was melanosis (95.7%), followed by leukomelanosis (57.0%) and keratosis (55.9%). In the majority of the cases, these manifestations were found in combination. Leukomelanosis and keratosis were more commonly found in moderate and severe arsenicosis cases than among mild cases. Melanosis was commonly found on the chest, abdomen, and back, and keratosis on the palm and soles. Leukomelanosis was mostly found on the thighs. Discussion Arsenic contamination in tubewell water was found in Nepal on the alluvial plains along the southern border with India; these plains are called the ‘Terai’. About 90% of the terai people usually depend on 600,000-800,000 tubewells as the source of their drinking-water. It was reported that, of 18,635 tubewells located in 20 districts of terai examined for arsenic concentration, 7.4% had arsenic contamination (>50 µg/L), and the large majority (76.3%) had below the guideline value of the World Health Organization (<10 µg/L) (4). Arsenic contamination in tubewells in the examined districts varied from 0.0% to 25.7%. According to that report, of 20 districts in the terai region, the higher percentages of arsenic-contaminated tubewells were found in Nawalparasi, Parsa, Bara, Rautahat, Rupandehi, and Kapilavastu districts (4). Arsenic contamination was high in Nawalparasi, and in this study, the prevalence of arsenicosis was also highest (3.6%). Next to Nawalparasi, the prevalence of arsenicosis was found to be high (2.2%) in Rautahat. The overall prevalence of arsenicosis in six districts was 2.2%, while the prevalence of arsenicosis in four villages was 10.2%. Among these villages, the highest prevalence (18.6%) of arsenicosis cases was found in Patkhouli village, where most (95.8%) tubewells were contaminated with arsenic. In both the studies, i.e. studies in six districts and in community-based studies, the prevalence of arsenicosis was significantly higher among males. In West Bengal and Bangladesh, different studies also showed the higher prevalence of arsenicosis among males than among females (9,10,13). However, in relation to age, the prevalence of arsenicosis was high in the older age-group (50 years and above), while, in West Bengal, the prevalence of arsenicosis was high both in the middle age- and older age-groups, and, in Bangladesh, the proportion of arsenicosis was high in early and middle age-groups (8-10). As in many preceding studies in West Bengal (10) and Bangladesh (9), the current study revealed that manifestations in skin, such as melanosis and keratosis, were common among the arsenicosis patients. Melanosis was commonly present on the chest or trunk, while keratosis on the palms and soles and leukomelanosis on the thighs. Regarding the extent of severity of arsenicosis, most cases were found at the mild and mode-rate stages (12), while, in Bangladesh, severe arsenicosis was slightly higher compared to that in Nepal. In Bangladesh, complications, such as non-pitting pedal oedema, gangrene, and cancer, have been reported in different studies (9,14) but, in Nepal, no such complications have yet been reported. It is important to mention that, as the studies were carried out in some programme areas and tubewells installed by villagers or by others were not included, there might have some selection bias. However, the findings of these studies will contribute to providing precise information in knowing the existence of arsenicosis patients in larger populations in the terai region of Nepal. Results of the studies showed the existence of arseni-cosis patients resulting from the consumption of arsenic-contaminated tubewell water in the terai region in Nepal. With the spatial and unequal distribution of arsenic in groundwater and other unknown factors yet to be explored, there was individual or sex variation in toxicity of arsenic despite living in the same environment. Since most identified arsenicosis patients were at the mild and moderate stages, they are expected to recover if further exposure is avoided and proper case management provided, otherwise they are likely to develop severe irreversible symptoms of diseases, including cancer. Based on the findings of the studies, the following measures are suggested for further actions: (a) regular screening and monitoring of tubewells and other sources of water for arsenic contamination; (b) awareness-building and motivational programmes should be organized in arsenic-affected villages so that people stop using arse-nic-contaminated water and accept and use the arsenic-safe water options; (c) health professionals in the local health posts or hospitals or paramedical persons should be trained on diagnosing arsenic-related health implications and its management which will greatly help undertake preventive measures; (d) necessary steps should be taken to develop and equip the existing research laboratories for analysis of biological samples (hair, nail, urine) for arsenic; and there is still a scope for conducting a systematic and comprehensive health survey on arsenicosis and, thus, further efforts should be made in this context. References
© 2006 ICDDR,B: Centre for Health and Population Research The following images related to this document are available:Photo images[hn06030f1.jpg] [hn06030t1.jpg] [hn06030t5.jpg] [hn06030t2.jpg] [hn06030t4.jpg] [hn06030t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}