 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
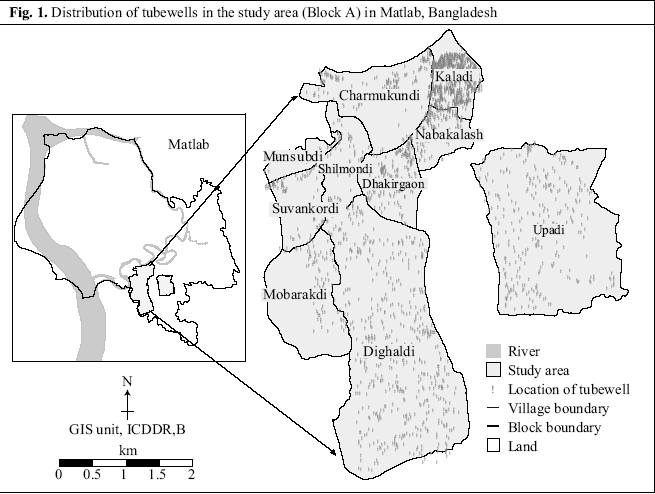
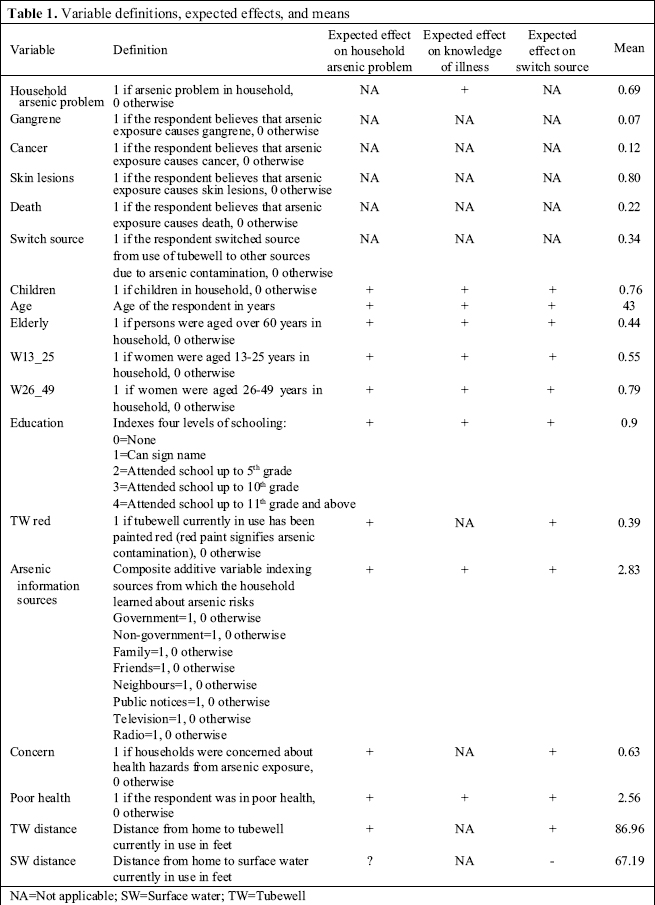
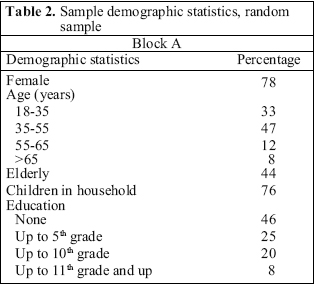
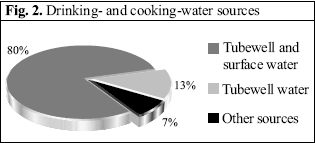
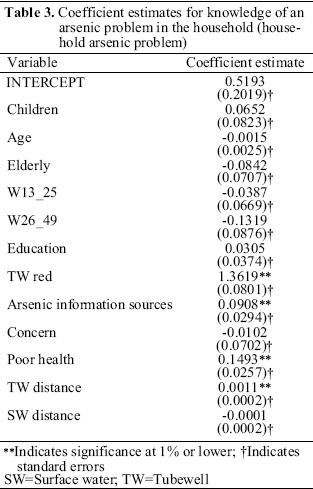
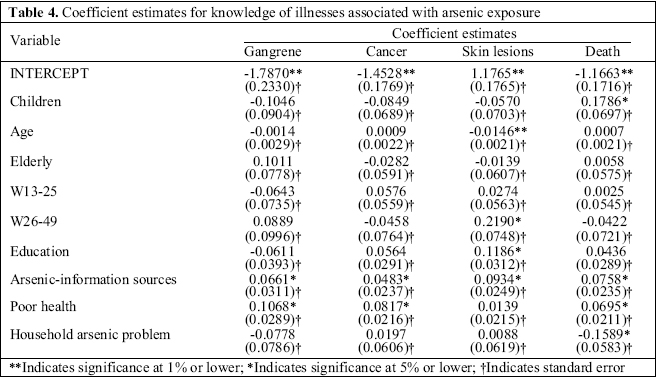
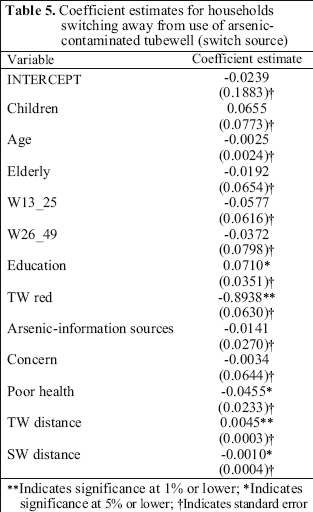
Journal of Health, Population and Nutrition, Vol. 24, No. 3, Sept, 2006, pp. 327-335 Knowledge of Arsenic in Drinking-water: Risks and Avoidance in Matlab, Bangladesh Sonia N. Aziz, Kevin J. Boyle, Mahfuzar Rahman Virginia Tech, 208-A Hutcheson Hall, Blacksburg, VA 24061, USA andICDDR,B, GPO Box 128, Dhaka 1000, Bangladesh Code Number: hn06041 ABSTRACT Widespread contamination of arsenic in Bangladesh has been jeopardizing the health of millions of people. Residents of Matlab, Bangladesh, are among the millions at risk. Using bivariate models in the analysis of survey data, knowledge of health risks and avoidance of arsenic exposure in response to widespread contamination of arsenic for residents of Matlab were estimated. The models examined individuals’ knowledge of an arsenic problem in the household and knowledge of specific illnesses caused by arsenic exposure. The likelihood of avoiding exposure to arsenic contamination was further examined. Results of the estimation showed that individual’s knowledge of arsenic problems in the household was gathered through awareness campaigns and by word of mouth and that knowledge of illnesses was predicated on education, health, presence of children, elderly and young women. Adoption of avoidance measures was not affected by exposure to arsenic-information sources, but level of education had a statistically significant positive effect on the decision to avoid arsenic exposure. Lack of convenience of safe drinking-water practices lead people to persist in drinking arsenic-contaminated water. Key words: Arsenic; Water pollution; Water supply; Drinking-water; Risk factors; Arsenic exposure; Awareness; Bangladesh Introduction The demand for environmental quality in developing countries is generally considered to be relatively low due to poverty. The demand for safe drinking-water, for example, may be overwhelmed by other competing needs for survival. It has been conjectured that lack of awareness about the adverse effects of degraded environmental quality, combined with poverty, keeps the demand for resources such as safe drinking-water relatively low (1). However, if the health risks associated with contaminated water are properly understood, the need for survival may dictate a higher demand for safe drinking-water. Contaminated drinking-water is a major health hazard in developing countries where infectious diseases caused by pathogens and parasites make up the most common and widespread health risk. The effects of diseases from pathogenic bacteria are immediate and debilitating, even affecting the taste and appearance of drinking-water (2). Despite these obvious ill effects and inexpensive water-purification methods, adoption of safe drinking-water practices is not prevalent. Gadgil showed that many people were unaware of the link between contamination of water and diarrhoea—indicating that awareness of the link between water and disease risk is an important condition for people in developing countries to demand safe drinking-water (3). Naturally-occurring arsenic in groundwater of South and South-East Asia has also been jeopardizing the health of millions of people who have been drinking contaminated water for years. In areas with natural geological contamination, such as Bangladesh, drinking-water from wells containing high levels of inorganic arsenic can cause serious health consequences, such as skin lesions, cancer, and death (4). Unlike contamination of drinking-water by pathogens, arsenic does not affect the taste or appearance of drinking-water and, moreover, the health effects from ingesting arsenic-contaminated water appear very slowly. For example, the average latency for appearance of skin lesions may be 23 years from the first exposure (5). Use of arsenic-contaminated water may be predicated on lack of awareness of the dangers posed by such action. With taste and appearance not being an issue and with health risks being an abstract notion, it is essential for public-health officials to increase public awareness of risks of arsenic to change the behaviour of people who use this water. Previous studies attempting to explain and predict health-related behaviours have identified that perceived negative consequence of taking a health action is the most influential variable for predicting actions taken to avoid health risks (6). Other studies have shown that the perceived effectiveness of actions taken to avoid exposure and events that motivate people to take such action (such as public-awareness campaigns) leads to change in behaviour. Results from these studies showed that more knowledge of risks improved the perceived effectiveness of actions taken to avoid exposure. Further, it has been shown that perceived risk may decrease with increase in knowledge (7). Water sources free of arsenic may be few and far between, taking a practical toll on a person’s time available for work. Such perceived negative consequences stemming from the lack of arsenic-free groundwater are complicated by the trade-off of health risks from consuming pathogen-contaminated surface water. Loss of convenience may outweigh the long-term costs associated with obtaining safe drinking-water. This ambivalence or reduced concern may be mitigated by individual household characteristics, such as the presence of children in the household—it is more likely for a child to contract diseases from arsenic exposure within their lifetime that it is for the contraction of such diseases within a parents’ lifetime (5). By disseminating knowledge on health risks associated with arsenic exposure, a successful public-awareness campaign could change health behaviours. Accordingly, the demand for safe drinking-water may reflect mitigating factors, such as the presence of children in the household. To assess people’s awareness of arsenic-related health risks, Ahmad et al. investigated the extent to which households in Bangladesh are aware of the consequences of consuming arsenic-contaminated water from tubewells (8). Most (87%) respondents were aware of the problem, but few were aware of the serious health risks associated with drinking arsenic-contaminated water. The study also found that radio, television, government and non-governmental agencies were important sources of information of arsenic, followed by members of the family and other residents of the village. Ahmad et al. also found that 69% of households in the study area changed their drinking-water source due to contamination with arsenic. While the 2003 study done by Ahmad et al. looks at the household’s awareness of the arsenic problem and related concerns, no statistical analysis was undertaken to explain households’ awareness and households’ knowledge of arsenic risks. The research presented in this paper focuses on a statistical analysis to identify the factors that significantly explain knowledge of arsenic contamination in Matlab, Bangladesh. The specific objectives of this study were to: (i) investigate factors affecting the individuals’ knowledge of arsenic contamination in tubewell water in the household, (ii) investigate factors affecting public knowledge of illnesses associated with arsenic exposure in drinking-water, and (iii) investigate household avoidance of exposure to arsenic contamination in drinking-water. A survey was conducted to collect data to address these objectives. Information from the analyses of these objectives will assist policy-makers in considering the effectiveness of current education efforts and in crafting future public-awareness campaigns of arsenic risks. While results from the study relate to Matlab, Bangladesh, the general findings are of pertinence to other rural areas in the developing world. Materials and Methods In-person interviews were conducted in Matlab, Bangladesh, during March-June 2004, under the auspices of International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR,B). Matlab has seven sub-divisions—A through G—for major ongoing research activities. This study is an addendum to an ongoing project titled “Arsenic in tubewell water and health consequences,” which is a joint effort of ICDDR,B and other collaborating institutions. The study was performed on a stratified random sample of the population in Block A (Fig. 1). The total target sample size for the study was 3,000 households. Enumerators interviewed 2,800 households. The first section of the survey was designed to collect sociodemographic data. The second section included questions about individuals’ awareness of various arsenic-related issues. Section three was designed to reveal household sources of drinking- and cooking-water, including questions on avoidance of exposure to arsenic-contaminated drinking-water. The survey was pre-tested by administering the instrument to 40 people outside the sample area. Responses from the selected survey items were used for defining binary variables representing individuals’ knowledge of arsenic contamination in the household (Objective i), knowledge of arsenic diseases (Objective ii), and avoidance of arsenic exposure (Objective iii). Addressing the first objective involved a variable representing knowledge of an arsenic problem in the household (household arsenic problem). The variable—household arsenic problem—was based on answers to the question of whether the respondent currently or has ever had an arsenic problem in their households. Addressing the second objective involved a set of variables representing households’ knowledge of health consequences of arsenic exposure. The specific health consequences represented by the dependent variables here are knowledge of gangrene (gangrene), knowledge of cancer (cancer), knowledge of skin lesions (skin lesions), and knowledge of death (death) due to long-term arsenic exposure. The answers revealed a wide variation in knowledge of health consequences of arsenic exposure allowing us to examine the link between the knowledge of health consequences of arsenic and the decision to avoid arsenic exposure. Implementing the third objective involved a variable representing the decision of households to avoid exposure to arsenic-contaminated drinking-water (switch source); this is an indicator for avoidance measures. This dependent variable is based on answers to the question of whether the respondent has ever switched away from using red tubewells that identify elevated arsenic levels. The investigation of the effects of respondent characteristics on the variables described above was done using a probit model. A probit model is a statistical model in which the dependent variable yi is either one or zero: Pr(yi=1)=-F(xi ß) Here Pr(yi=1) denotes the probability that the dependent variable is 1 (e.g. have an arsenic problem), F is a normally-distributed cumulative distribution function, xi is a vector of household characteristics, and ß is a vector of parameters to be estimated that explains how household characteristics affect each of the six dependent variables (household arsenic problem, gangrene, cancer, skin lesions, death, and switch source). One equation is estimated for each of the six dependent variables defined above. The independent variables (xi)—household characteristics that were used for explaining each of the dependent variables—are defined in Table 1. Knowledge of an arsenic problem in the household (household arsenic problem) is specified as a function of children, age, elderly, W13_25, W26_49, education, TW (tubewell) red, arsenic-information sources, concern, poor health, TW distance, and SW (surface water) distance. We conjectured that children, age, presence of young women, presence of elderly, education, arsenic-information sources, concern, and poor health would have a positive effect on knowledge of an arsenic problem in the household (9,10). The status of tubewell (TW red) was also conjectured to have a posi-tive effect on knowledge of an arsenic problem—the purpose of painting the tubewell red is to raise awareness of arsenic in drinking-water (11). Distance to surface water (SW distance) may have a positive or negative effect on knowledge of a problem. Proximity to surface water may mean that individuals have a lower chance of being exposed to arsenic problems. On the other hand, proximity to surface water may increase the chances of contamination by pathogens, which may prompt the respondent to seek knowledge on water-contamination problems, including contamination with arsenic. Knowledge of each illness caused by arsenicexposure was estimated as a separate model. Each of the knowledge of illness variables indicates whether the respondent believed that arsenic causes gangrene, cancer, skin lesions, or death. Each of these variables was specified as a function of household arsenic problem, children, age, elderly, W13_25, W26_49, education, arsenic-information sources, and poor health. Concern about potential health hazards (concern) was not included as an explanatory variable because the focus was on awareness of specific health concerns. Distance to water sources was not conjectured to have an effect on perceived arsenic risks. Avoidance of exposure (switch source) was not conjectured to explain knowledge of illnesses. It may be the case that avoidance is explained by knowledge of illnesses, but knowledge of illnesses is not predicated on people’s avoidance of arsenic exposure. Avoidance of arsenic exposure (switch source) is a variable that indicates a household’s decision to switch away from use of red tubewells. Switching of households from use of tubewell (switch source) was specified as a function of children, age, elderly, W13_25, W26_49, education, TW red, arsenic-information sources, concern, poor health, TW distance, and SW distance. We conjectured that sociodemographic characteristics, such as presence of children, age, presence of women, knowledge, and level of education, increased the propensity to avoid arsenic exposure. We also conjectured that concern about potential health hazards (concern) would have a positive affect on the tendency to avoid arsenic exposure. Perceived convenience, such as distance travelled to avoid arsenic exposure, of avoidance measures was also considered to have a positive affect on the tendency to avoid arsenic exposure. Prior empirical work on the avoidance of exposure to contamination showed that the presence of children, age, education, information on exposure and its consequences, subjective consideration of risk, and perceived convenience of averting activities seemed to increase the propensity to avoid exposure (10,12-17). All equations and analyses were done using SAS. Results The demographic statistics of the sample are presented in Table 2. Most respondents interviewed were female (78%), whereas the proportion of females in the overall population was 49% (18). The target respondent was the household member most knowledgeable about sources of drinking-water and water-use patterns. Since this was usually the female head of the household, the sample population had a higher proportion of women than that of the overall population of Bangladesh. The average age of the respondents was 43 years. A relatively few respondents were aged above 65 years. In contrast, only 3.4% of the overall population included persons aged over 60 years. Almost half of the respondents were illiterate, while about one-fourth of the population had been educated only up to the fifth grade. This is roughly comparable to a literacy rate of 43.1% in the overall population. Eighty percent of the respondents used a combination of tubewell water and surface water for drinking and cooking (Fig. 2). Thirteen percent relied solely on tubewell water. The remaining 7% used other sources for drinking- and cooking-water. The results of the survey revealed that approximately 70% of the respondents had exposure to arsenic problems in their households. Although this is lower than the finding of Ahmad et al. that 87% of respondents were aware of the arsenic problem; it is important to note that the questions asked in the two surveys were not exactly the same. Ahmad asked for awareness of arsenic (8), and here the question was whether households knew that they had an arsenic problem in their drinking-water. The survey results also showed that 64% of the respondents had switched away from use of tubewells, and 60% of these respondents had switched away from use of tubewells due to contamination with arsenic. This is also lower than the finding of Ahmad et al. that 69% of households in their sample area changed their drinking-water sources due to arsenic contamination (8). Results from the first probit model indicated that the status of tubewell, arsenic-information sources, poor health, and tubewell distance were important determinants in knowledge of an arsenic problem in the household (household arsenic problem), while sociodemographic characteristics were not significant (Table 3). If the tubewell was painted red, this increased the individuals’ knowledge of an arsenic problem in the household. The greater the number of sources from which the household learned about arsenic risks, the higher the individuals’ knowledge of an arsenic problem in the household. People with poor health had a higher likelihood of knowing about an arsenic problem in the household. People who were using tubewells farther away also had a higher likelihood of having knowledge of an arsenic problem in the household, which might reflect the fact that people were travelling to a tubewell that was farther away to avoid exposure to arsenic in their household’s water. None of the sociodemographic characteristics affected the households’ knowledge of an arsenic problem. Results from the second probit model explaining the knowledge of illnesses of arsenic exposure (gangrene, cancer, death, and skin lesions) are presented in Table 4. Arsenic-information sources had a significant and positive effect on knowledge of all four health consequences from arsenic exposure (gangrene, cancer, skin lesions, and death). Poor health had a significant and positive effect on knowledge of gangrene, cancer, and death. Age, presence of women aged 26-49 years, education, and arsenic-information sources—all had a significant effect on knowledge of skin lesions as a consequence of arsenic exposure. Older people tended to believe less in the probability of contracting skin lesions from arsenic exposure. Given the long latency period before skin lesions from arsenic exposure developed, an older person might perceive less risk of contracting skin lesions from arsenic exposure. The presence of women aged 26-49 years in the household increased the probability of perceiving skin lesions as a potential health hazard from arsenic exposure. Respondents with higher education and with exposure to more sources of knowledge regarding arsenic risks had a higher probability of believing that skin lesions are caused by arsenic exposure. Given that skin lesions are the most visible among the health consequences of arsenic exposure, the strength of results for knowledge of skin lesions was not surprising. The presence of children in the household had a significant and positive effect on the probability of perceiving death as a serious health hazard from arsenic exposure. Knowledge of a household arsenic problem, however, had a significant and unexpected effect on death. It decreased the probability of perceiving death as a serious health hazard from arsenic exposure. | Results from the third probit model (switch source) showed that the probability of avoiding arsenic exposure was influenced by education, status of tubewell, poor health, distance to tubewell, and distance to surface water (Table 5). Higher educational levels increased the probability of avoiding arsenic exposure. People who still used a red-painted tubewell were less likely to switch to an alternative source. Poor health status also decreased the probability of avoidance—it might be the case that persons with poor health were unable to walk a long distance to collect cleaner water. Distance to tubewell currently in use had a positive effect—this means that travelling a long distance to gather clean tubewell water does not deter an individual’s propensity to avoid exposure. The farther away the surface water, the lower the probability of avoiding arsenic exposure. If the surface water was too far away, people likely consider switching away from using their current tubewells to be inconvenient. This may be due to the time and opportunity costs associated with the treatment of surface water and the long distance that must be traversed to get to surface water. |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}