 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
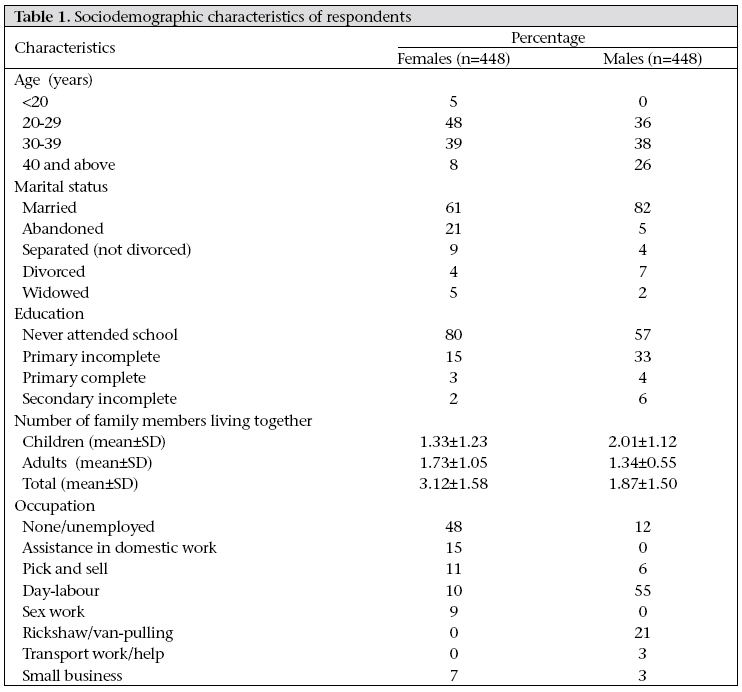
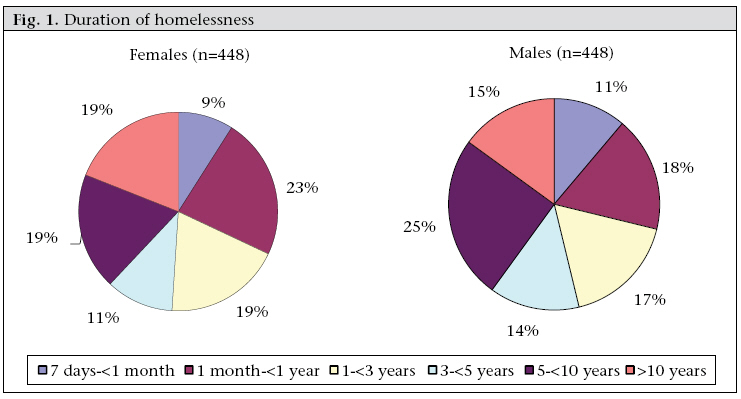
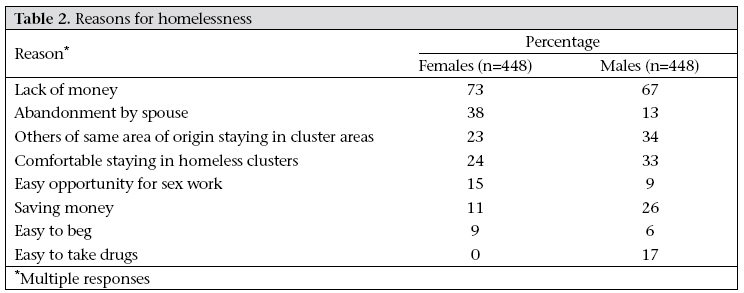
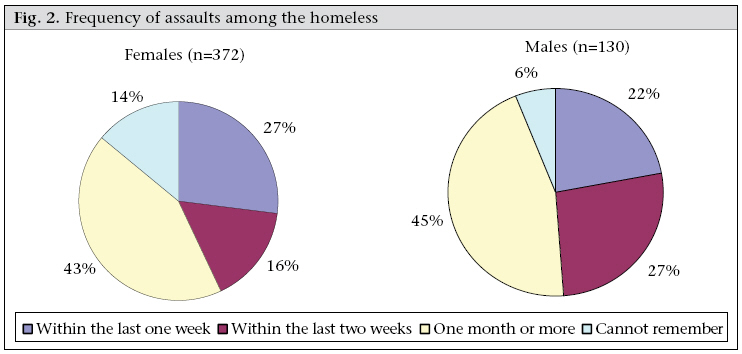
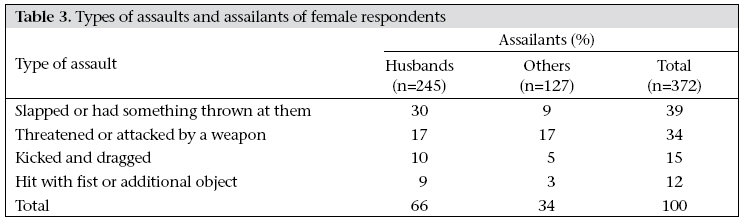
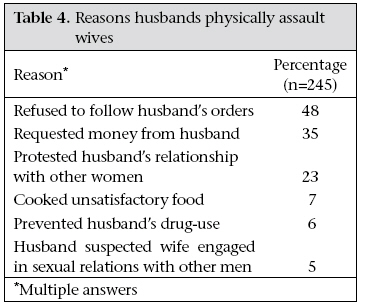
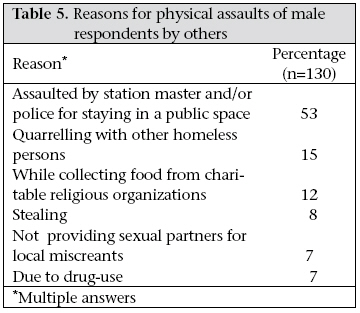
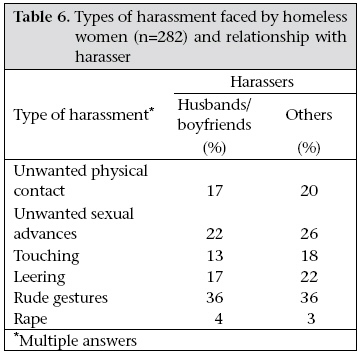
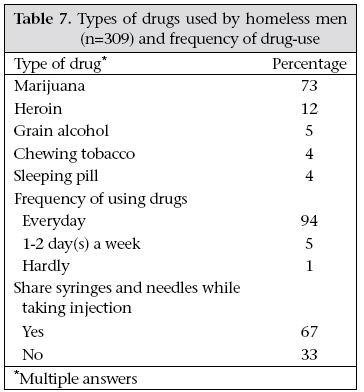
Journal of Health, Population and Nutrition, Vol. 27, No. 4, Aug, 2009, pp. 452-461 Homeless in Dhaka:Violence, Sexual Harassment, and Drug-abuse Tracey Pérez Koehlmoos, Md. Jasim Uddin, Ali Ashraf, and Mashida Rashid ICDDR,B, GPO Box 128, Dhaka 1000, Bangladesh Code Number: hn09045 ABSTRACT Bangladesh has experienced one of the highest urban population growth rates (around 7% per year) over the past three decades. Dhaka, the capital city, attracts approximately 320,000 migrants from rural areas every year. The city is unable to provide shelter, food, education, healthcare, and employment for its rapidly-expanding population. An estimated 3.4 million people live in the overcrowded slums of Dhaka, and many more live in public spaces lacking the most basic shelter. While a small but growing body of research describes the lives of people who live in urban informal settlements or slums, very little research describes the population with no housing at all. Anecdotally, the homeless population in Dhaka is known to face extortion, erratic unemployment, exposure to violence, and sexual harassment and to engage in high-risk behaviours. However, this has not been systematically documented. This cross-sectional, descriptive study was conducted to better understand the challenges in the lives of the homeless population in 11 areas of Dhaka during a 13-month period from June 2007 to June 2008. A modified cluster-sampling method was used for selecting 32 clusters of 14 female and male respondents, for a sample of 896. In addition to sociodemographic details, this paper focuses specifically on violence, drug-abuse, and sexual harassment. The findings showed that physical assaults among the homeless, particularly among women, were a regular phenomenon. Eighty-three percent of female respondents (n=372) were assaulted by their husbands, station masters, and male police officers. They were subjected to lewd gestures, unwelcome advances, and rape. Male respondents reported being physically assaulted while trying to collect food, fighting over space, or while stealing, by police officers, miscreants, or other homeless people. Sixty-nine percent of the male respondents (n=309) used locally-available drugs, such as marijuana and heroin, and two-thirds of injecting drug-users shared needles. The study determined that the homeless are not highly mobile but tend to congregate in clusters night after night. Income-generating activities, targeted education, gender-friendly community police programmes, shelters and crises centres, and greater community involvement are suggested as policy and programmatic interventions to raise the quality of life of this population. In addition, there is a need to reduce high rates of urban migration, a priority for Bangladesh. Key words: Cross-sectional studies; Descriptive studies; Developing country; Homelessness; Sexual harassment; Substance-abuse; Violence; Bangladesh BACKGROUND Globally, more people now live in urban areas than in rural areas. Over the past few decades, most lowincome countries have experienced a rapid population growth without adequate expansion of public services, and many cities in the developing world lack the infrastructure necessary to support high levels of urban population growth. As a result, globally, more than one billion people live in informal settlements or urban slums (1,2). Many others live where they can—at railway terminals and busstations, at ports, and in empty markets, parks, and stairways. In almost every major urban centre of Bangladesh, tens of thousands of people live in overcrowded slums or public spaces that lack basic facilities, such as safe water, sanitation, and health services (3). Bangladesh has experienced one of the highest urban population growth rates (around 7%) in the last three decades compared to a national population growth rate of about 1.5% per year (4). In Dhaka, an estimated 37% (n=9,136,182) of the total metropolitan population in 2007 lived in slums (5). Dhaka continues to grow as a mega-city, with approximately 320,000 migrants annually. More than three-quarters of migrants find shelter in urban slums or do not find shelter at all. Employment, shelter, and accessibility to basic services for the growing urban poor populations—those who live in informal settlements and those who are homeless—are critical issues yet to be fully addressed by policy-makers in Bangladesh (6). A study in Bangladesh in 1995 defined the homeless as people who sleep on streets, railway terminals and platforms, bus-stations, parks and open spaces, religious centres, construction sites, around graveyards, and in other public spaces with no roof (6). This population is sometimes referred to as ‘streetdwellers’. A government census in 1997 used the term ‘floating population’ to describe “the mobile and vagrant category of rootless people who have no permanent dwelling units” and may be found spending the nighttime hours in the rail-stations, piers (launch ghat), bus–stations, closed bazaars, stairways of public buildings, and open spaces. The terms ‘street-dweller’ and ‘floating population’ are rarely used outside Asia (7). The definition of the homeless population in this study is based on the above descriptions. The 1997 census count of the homeless population was 14,999 in Dhaka, with an additional 17,082 in other metropolitan areas of Bangladesh (7). A study in 2001 by the Marie Stopes Clinic Society (MSCS) estimated the number of homeless to be between 1,000 and 4,000 in each of seven major locations in Dhaka. The survey found that many homeless were living on their own: 26% were unmarried females and 15% unmarried males. However, 36% were living as married couples and families with an average family size of 3.6. The proportions of people in different age/sex-groups on the basis of rough estimates by homeless in seven locations were as follows: children–14%, adolescents–11%, women– 46%, and men–29% (8). The definition of homeless used in the present study reflects that many people live without permanent shelter in major towns and cities. The 1997 study by Islam et al. found that 47% of the homeless in Dhaka lived on footpaths, 23% in the city’s transport-stations, and 12% in front of major market centres. People are found in the above locations in all seasons, although their numbers vary throughout the year. Concentrations of people increase following natural disasters, such as flood, cyclone, and famine. During religious festivals, many rural poor from nearby districts migrate to the city and live temporarily as homeless to take advantage of increased seasonal charitable donations. However, the main reason for migration into the city is economic as many migrate permanently from rural areas to seek employment. Islam et al. found that nearly a quarter of the homeless came to Dhaka after losing their land and assets due to erosion of river-bank (6). Although a growing body of literature focuses on the conditions in the urban slums both globally and in Bangladesh, less is known about the conditions of the homeless population (2,3,6,8-10). This study presents a snapshot of the lives of the homeless population in Dhaka, particularly with respect to the violence, illegal drug-use, and sexual harassment that is a part of their daily lives. These findings are used for making recommendations for a future population policy that will anticipate the needs of the urban homeless, recognizing that the ultimate goal is to eliminate homelessness. MATERIALS AND METHODS This community-based, cross-sectional and descriptive study was conducted in 11 selected areas of Dhaka city over a 13-month period from June 2007 to June 2008. These selected areas included the five major entry-points for rural people moving into the city: Kamalapur, Saidabad, Sadarghat, Gabtoli, and Mohakhali, and also in other locations with major concentrations of homeless persons: High Court premises, Kawran Bazar, Mirpur Mazar, Stadium area, Cantonment Railway Station, and Gulshan market. Sampling Samples were drawn from adult men and women who slept in the last week within a two-kilometre radius of the five entry-point locations and from six other locations in Dhaka. To identify potential participants for inclusion in the study, enrollment was carried out at night while the homeless persons made preparation to sleep. A modified cluster-sampling method was used for selecting 32 clusters of 14 females and males (448 ever-married females or mothers aged 15-49 years and 448 ever-married males aged 15-49 years). Depending on the number of adults available for interview, sub-clusters of seven respondents were sometimes required. The interviewer went to the centre of the location being occupied by homeless persons and spun a bottle to randomly select a direction. Following this randomly-chosen direction, the interviewer then walked to the border of the location counting the number of adults of each sex. The interviewers used a table of random numbers for selecting a number (n) between one and the number of adults along the direction pointed by the bottle. Counting adults situated along that direction, the first interview was with the nth adult. Subsequent interviews were conducted with the nearest adult until the cluster was completed. Sample size For the survey questionnaire, a separate sample was required for ever-married females and ever-married males aged 15-49 years. The sample size required using simple random sampling was 224. However, allowing for an unknown cluster-sampling design effect (estimated at 2), the sample required for each of the adult age/sex-groups was 448. In total, we conducted 896 semi-structured interviews: 448 with men and 448 with women. Collection of data and research instrument Interviewers conducted a cross-sectional semistructured survey of homeless adults. Information was collected on violence, drug-abuse, and sexual harassment. The sets of questionnaire contained structured questions which were pre-coded and also contained several open-ended questions. Eight interviewers (four males and four females aged 2635 years) with 8-12 years of experience and having a master’s degree worked together in each site. Several measures were taken to ensure the safety of the interviewers. Before conducting interviews in a cluster area, we informed local law enforcement and police stations of the planned activities. Further, influential persons in the cluster areas were contacted before the start of interviews. Last, we mandated that interviewers travel and work in teams. Analysis of data Data were entered into visual BASICS/FoxPro and analyzed using the SPSS software (version 11.5). Responses to open-ended questions were quantitatively analyzed and categorized for coding according to similarity of response before being entered in the BASICS and SPSS. Both bivariate and multivariate analyses were carried out, with statistical significance based on 95% confidence interval and standard statistical tests. Multiple logistic regression analysis was conducted to identify factors that were associated with different dependent variables. Ethical consideration The Ethical Review Committee of ICDDR,B approved the study. Each potential research respondent completed a signed informed consent-sheet prior to participation in the survey. The consentsheet was written in Bangla and was read out in Bangla to the potential respondent. All respondents understood their rights not to participate in the survey and their rights to withdraw from survey participation anytime during the interview. RESULTS Sociodemographic information Table 1 shows that 48% of the female respondents were aged 20-29 years while 74% of the male respondents were evenly split between 20-29 years and 30-39 years of age. Sixty-one percent of the female respondents were currently married whereas the other one-third of the female respondents were abandoned, separated, divorced, or widowed. Eighty-two percent of the male respondents were currently married. Eighty percent of the female and 57% of the male respondents had never attended any school. The main occupations of the homeless women were assistance in domestic work, engaged in ‘pick and sell’ activities (collecting items from garbage depots and selling them), day-labour, and sex work. Nearly half of the female respondents were unemployed. More than half of the male respondents reported working as day-labourers, with rickshaw/van-pulling occupying an additional 21%. The gender differences were evident in the type of small businesses operated by the respondents. Women reported running small stands-selling tea, cigarettes, chocolates, or betel nuts, and men reported working as butchers. Information was also collected on other incomegenerating activities of the homeless men and women. Half of the female respondents were involved with begging either full-time or part-time while 11% and 5% of the male respondents were involved in begging full-time and part-time respectively. Seven percent and 5% of the male respondents were involved, respectively, with part-time blood-selling and stealing to earn money to provide necessities for wives and children. Figure 1 shows that the majority (68%) of the respondents had been homeless for more than a year. Approximately half of both females and males had been homeless for more than three years. Nineteen percent of the females and 15% of the males had been homeless for over 10 years. Using open-ended questions, the respondents were asked about reasons for living as homeless persons. Both male and female respondents mentioned lack of money/no income to rent a house as the primary reason. Other common reasons included: spouses abandoned them while homeless; people from their villages of origin were also living as homeless persons; feelings of comfort while living with so many other people (informal support networks within the clusters of homeless people); ease of sex work opportunities; beliefs of being able to save money; ease of begging; and easy access to and use of drugs (Table 2). Physical violence Data were collected and analyzed to ascertain the status of physical violence among the homeless. The respondents were asked if they were ever assaulted by their spouses or others while walking or lying in open areas or in public spaces. Eightythree percent of the female and 29% of the male respondents had ever been assaulted while living as a homeless person. Physical assaults among the homeless were a regular phenomenon. Of those who reported being assaulted, 27% of the females and 22% of the males were assaulted by others within the past week (Fig. 2). Another 16% of the female and 27% of the male respondents reported an assault in the two weeks prior to data collection while 43% of the female and 45% of the male respondents reported assaults one month or more prior to data collection. In a series of open-ended questions, the female respondents were asked about the types of assaults and assailants. Of the 372 female respondents who reported having ever been assaulted, 66% were assaulted by their husbands. Other assailants of the female respondents included boyfriends, strangers, law-enforcement officers, staff members of public utilities where they were living, and local miscreants. The female respondents were most often slapped or had something thrown at them (39%), or threatened and/or attacked by a weapon (34%). They were also kicked and dragged (15%) or hit with a fist or some other objects (12%) (Table 3) Table 4 shows the responses that women who reported being assaulted by their husbands gave to an open-ended question on the reasons their husbands assaulted them for. About half (48%) informed that their husbands assaulted them for refusing to follow orders, such as giving money to the husband, going outside without permission, or refusing to nurse step-children. More than onethird (35%) who had experienced assaults reported that it was due to asking their husbands for money to buy food or to meet the needs of children. Twenty-three percent were assaulted by their husbands due to protests over the husband’s relationship with another woman. Other reasons mentioned by the female respondents for being assaulted by their husbands included the husband’s disliking of food prepared by the wife, the wife having interfered with the husband’s drug-use, and the husband’s suspicion that his wife was engaged in sexual relations with other men. The reasons given by the female respondents for assaults by others revealed that 44% were assaulted by the station master and police while staying in public spaces, such as railway-stations, launch and bus-terminals. Twenty-six percent of the female respondents were assaulted while quarrelling with other homeless persons over sleeping space. Sixteen percent were assaulted because they did not agree with sexual propositions of police officers, and 12% were assaulted due to stealing. Information was also collected on types of assaults experienced by homeless men and the identity of their assailants. Of the 448 male respondents, 130 experienced assaults. The married men reported no incidence of assault by their wives. Forty-three percent of those who were assaulted said that they were hit with a fist or with something else while 26% were kicked and dragged. Twenty-two percent were slapped or having something thrown at them, and 9% were threatened or actually attacked with a weapon. Others who assaulted male respondents included law-enforcement officers, staff members of public utilities where the homeless were staying, and local miscreants. Of the 130 men who were assaulted, 53% of assaults were by authoritative figures, including station masters and police because they were staying in a public space. Other reasons for assaults included quarrelling with other homeless persons for sleeping space, fights while collecting food from charitable religious organizations, not agreeing to provide sexual partners for local miscreants, and being assaulted by police due to drug-use (Table 5). Sexual harassment among homeless women To assess the status of sexual harassment among homeless women, the female respondents (n=448) were asked if they were approached for unwanted physical contact or sexually propositioned while walking or lying in public spaces. More than twothirds (n=282) of the female respondents had experienced some form of unwanted physical contact or sexual proposition during their time as homeless women The victims were asked to describe the types of sexual harassment and their relationship with the harasser in their last incidence. They were harassed by boyfriends and others. Others included homeless men staying in close proximity to them, strangers, staff members of public utilities, local miscreants, and law-enforcing personnel (Table 6). The women were harassed through unwanted physical contact, unwanted sexual advances, touching, leering, rude gestures, and rape. In response to a question about how often the female respondents encountered harassment, threefourths of the victims (n=208) reported that it happened frequently. Categorical responses included that 8% experienced such encounters everyday, 43% reported two or three harassment episodes per week, and 23% experienced harassment two or three times per month. Drug-abuse The respondents were asked if they had used any drugs during the year prior to the survey. Less than one percent of the females reported drug-use. However, 69% of the males used some type of drug during the previous year. Table 7 shows that the male respondents were using various locally-available drugs, such as smoking marijuana, injecting heroin, drinking illegal locally-produced grain alcohol, chewing tobacco (gul), and taking sleeping pills. Ninety-four percent of the males used drugs every day. When asked, twothirds of drug-users who injected drugs reported sharing syringes and needles with others. DISCUSSION This study has shown that the homeless in Dhaka are extremely vulnerable in terms of their personal security and for men, their high-risk behaviours. Women especially suffer from physical violence at the hands of both their husbands and outsiders, such as law-enforcement officials, local miscreants, and boyfriends. They also suffer from all kinds of harassment, a majority of them two to three times per week, ranging from unwanted advances and rude gestures to rape. Males often get into violent fights over space for sleeping and food and get assaulted by police. The homeless men reported high levels of taking locally-available illegal substances, such as marijuana, grain alcohol, and heroin. That 55% (245 of 448) of the female respondents reported being assaulted by their husbands corroborates findings from an earlier multicountry study by the World Health Organization that included Bangladesh. The earlier study found that 53% of urban female respondents in Bangladesh had experienced physical and/or sexual abuse by an intimate partner (11). A recent World Bank paper reports that Bangladesh had the second highest incidence of violence against women in the world and that not only was violence against women widespread, it was also widely accepted: 50% of women interviewed thought that it was the husband’s rights to beat his wife; 85% felt that it was a right to hit wife if she was disobedient (12). Interventions to stop gender-based violence among the homeless can happen in both preventive and treatment/management levels. In Romania, the United Nations Population Fund has supported the Centers for Monitoring, Prevention and Management of gender-based violence in the capitals of districts. The centres provide integrated medical, emotional and juridical support to victims who are largely from urban areas but also from surrounding rural areas. They raise awareness about the consequences of violence but also train health personnel, local authorities, and police through regular coordination meetings with information, education, and communication activities (13). In Bangladesh, a small multisectoral initiative by the Ministry of Women and Children’s Affairs created two One-Stop Crisis Centres (OCCs), each one located within the emergency department of a major medical college hospital. During January-June 2008, the Dhaka-based OCC treated 284 cases (14). Such services should be placed within access of the homeless population and evaluated for expansion. The results of the present study showed that authoritative figures, like police officers and station masters, were responsible for a large number of assaults on both male and female respondents. Community-friendly policing is one innovative programme that can help prevent violence from escalating and change the relationship between those with power and those who are vulnerable. In Mumbai, police, with the help of community organizations, have started patrolling slum areas through community volunteers who are awarded responsibilities for their areas by the police department. These ‘panchayets’ bridge the gap between the community and the police and comprise mostly women to advocate gender-friendly policing. Conflicts, complaints, and disputes are settled by panchayets before they become violent, and the panchayets also address illegal drug and alcohol activities (15). This system reduces the risk of assault by police since members are elected by their own community. Bangladesh has similar initiatives, and the Ministry of Women and Children’s Affairs and the German Technical Cooperation (GTZ) are carrying out work for gender-friendly, community-based policing as part of a programme called Promotion of Legal and Social Empowerment of Women (16). These efforts might be implemented in the areas where the homeless regularly congregate. The findings of the present study showed that 31% of the male respondents were using drugs and sharing syringes. In addition to psychosocial counselling, other forms of treatment are necessary. One example is the current urban initiative between ICDDR,B and the United Nations Office on Drugs and Crime (UNODC) for a first-ever trial of methodone as a replacement therapy for injecting drugusers and additional interventions, such as needle distribution and behaviour-change communications for high-risk urban groups as part of the prevention of the spread of HIV/AIDS (17). Should this trial prove successful, its generalizability should be confirmed among this most vulnerable population before being scaled up. Further, establishing one-stop crises centres can be used for managing violence and drug-use. Aparajeyo Bangladesh and ChildHope UK are planning a five-year project which will provide health treatment, peer-to-peer counselling, and engage in raising awareness about drug-use, abuse, and the risk of STIs among streetchildren with 24-hour child-friendly centres (18). As additional preventive measures, it is useful to consider a range of policy options that seek to deal with, albeit indirectly, some conditions that give rise to alcohol and drug-use. These include: employment programmes targeted at sections of most at-risk population and integrated community services that can help build social capital and foster positive norms and support, especially for young people (19). This study demonstrates that the homeless are long-term residents of the same areas and that they routinely engage in high-risk behaviour and experience alarming rates of violence and sexual harassment. At the primary prevention level, it is important to create low-cost housing facilities, income-generating activities, credit extensions to start small businesses, and targeted education and awareness programmes. Working with residents’ associations, women’s savings and credit groups, Community Benefit Organizations, homeless communities, and NGOs is essential to identify the priorities, problems, and strengths of communities (12) and to stop the social exclusion that leads to conflict and drug abuse. The Government, through its Committee for Urban Local Governments, must lead the public-sec-tor ministries, the donor agencies, and civil society to address the levels of structural violence and urban poverty which work together to create the dismal living conditions of the homeless. Further, the Government needs to take the lead in addressing the larger issues of structural inequalities and the absence of human rights, such as rights to food, shelter, and education, which contribute to the social milieu of violence in the lives of the homeless. The present combination of social exclusion and continued rural to urban migration requires a multi-disciplinary coalition to work together to address the impact of urban growth, poverty, and the risky health experiences of vulnerable groups in the city, otherwise recommendations to improve this situation will not be effective. This study has several limitations. First, although we used random sampling, we are not sure the sample is representative of the entire homeless population in Dhaka. The limitation may be further amplified by our decision to include only ever-married men and women so that the experience of never-married homeless men and women is not captured in the study. We acknowledge that certain homeless people are more difficult to reach than others, and they were likely not captured here. Second, participation bias may have caused some homeless people to avoid being asked to participate. Third, as in any study that relies upon self-reporting, there may be recall bias on some issues and cultural biases in disclosure. Despite these limitations, this study has important implications for future programmes that work with urban homeless to increase their access to basic rights that should be guaranteed by society. ACKNOWLEDGEMENTS This research was funded by ICDDR,B and its donors which provide unrestricted support to the Centre for its operations and research. Current donors providing unrestricted support include: Australian Agency for International Development (AusAID), Government of the People’s Republic of Bangladesh, Canadian International Development Agency (CIDA), Embassy of the Kingdom of the Netherlands (EKN), Swedish International Development Cooperation Agency (Sida), Swiss Agency for Development and Cooperation (SDC), and Department for International Development (DFID), UK. The authors gratefully acknowledge these donors for their support and commitment to the Centre’s research efforts. The authors further express their heartfelt gratitude to Dr. Heidi Bart Johnston for her tireless support of the manuscript-revision process. REFERENCES
Copyright © International Centre for Diarrhoeal Disease Research, Bangladesh The following images related to this document are available:Photo images[hn09045t2.jpg] [hn09045t1.jpg] [hn09045t7.jpg] [hn09045t6.jpg] [hn09045f2.jpg] [hn09045t5.jpg] [hn09045t3.jpg] [hn09045t4.jpg] [hn09045f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}