 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Journal of Health Population and Nutrition, Vol. 28, No. 6, December, 2010, pp. 595-601 Duration of Breastfeeding and Its Correlates in Bangladesh Shamima Akter and Md. Mizanur Rahman Department of Population Science and Human Resource Development, University of Rajshahi, Rajshahi 6205, Bangladesh Correspondence and reprint requests should be addressed to: Md. Mizanur Rahman Assistant Professor Department of Population Science and Human Resource Development University of Rajshahi Rajshahi 6205 Bangladesh Email: mizanur_rub@yahoo.com Code Number: hn10077 ABSTRACT The purpose of this study was to assess the duration of breastfeeding and the sociodemographic factors affecting it. Data for the study were drawn from the Bangladesh Demographic and Health Survey 2004. In total 5,364 mothers were included in the study. The life table and Cox’s proportional hazards model were employed for the analysis of breastfeeding-related data, which showed that the average duration of breastfeeding was 31.9 months. Cox regression analysis revealed that the duration of breastfeeding was positively associated with maternal age, contraceptive-use, work status, and religion and was negatively associated with age at marriage, parity, delivery status, region, and maternal education. Younger mothers, having higher education, higher maternal parity, caesarean-section birth, being a Muslim, and mothers who have not used any contraceptive were associated with lower duration of breastfeeding. The findings suggest that health institutions can play a significant role in promoting breastfeeding in Bangladesh. Educational campaigns that stress the benefits of lactation are important strategies for encouraging mothers to breastfeed longer. Key words: Breastfeeding; Parity; Sociodemographic factors; Bangladesh INTRODUCTION Breastfeeding plays a vital and influential role on the duration of amenorrhoea, child survival, and fertility, offering protection to an infant against early morbidity and mortality. Short-term risks of not breastfeeding include an increased risk of post- partum haemorrhage while long-term effects may include a higher risk of osteoporosis and breast and ovarian cancers (1). Breastmilk contains all types of nutrients required for an infant in right proportion and composition (2). Longer and more frequent breastfeeding and ma-ternal survival status ensure the survival of chil- dren (3-4). Results of studies on cessation of breast-feeding of children suggest that mothers who have lower education stop breastfeeding earlier than those with higher education (5-7). Other factors that also relate to the duration of breastfeeding are present age of mothers and socioeconomic status (7-12). Younger mothers are most likely to termi- nate breastfeeding early compared to older counterparts (13-15). The importance of breastfeeding in regulating in-dividual and social fertility has been a matter of general interest for many years because it tends to increase the average birth interval and, therefore, to reduce women’s fertility over their life span, es- pecially in societies where the use of contraceptive methods is not widespread. Recent reviews and meta-analyses conclude that breastfeeding consti- tutes a small but consistent protective effect against obesity or higher values of body mass index (BMI) in children (16-19). The propensity to breastfeed is not only of importance with regard to the beneficial effects on individuals but is also of concern as an indicator of health behaviour relating to social conditions. A large body of research supports an association between the socioeconomic status and the health and development of children (20-24) but this concept has rarely been studied in relation to the duration of breastfeeding in the context of Bangladesh. The aim of this paper was to estimate the duration of breastfeeding and also to explore the sociodemographic determinants of the duration of breastfeeding in Bangladesh. MATERIALS AND METHODS
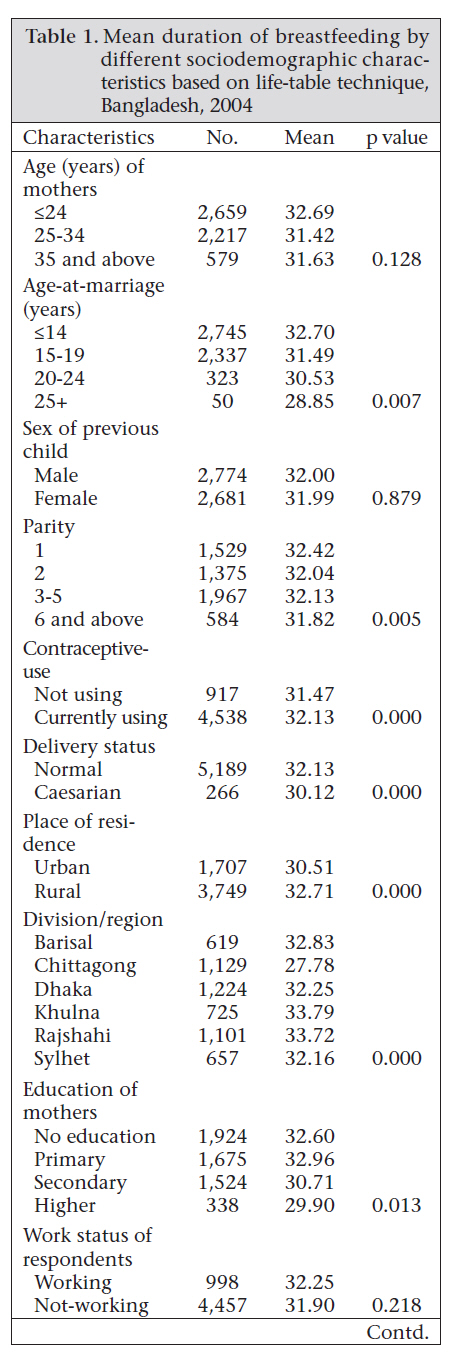
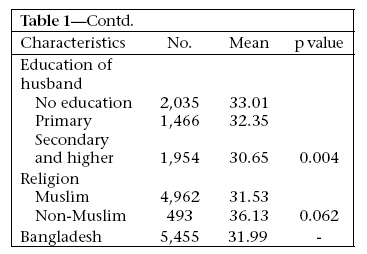
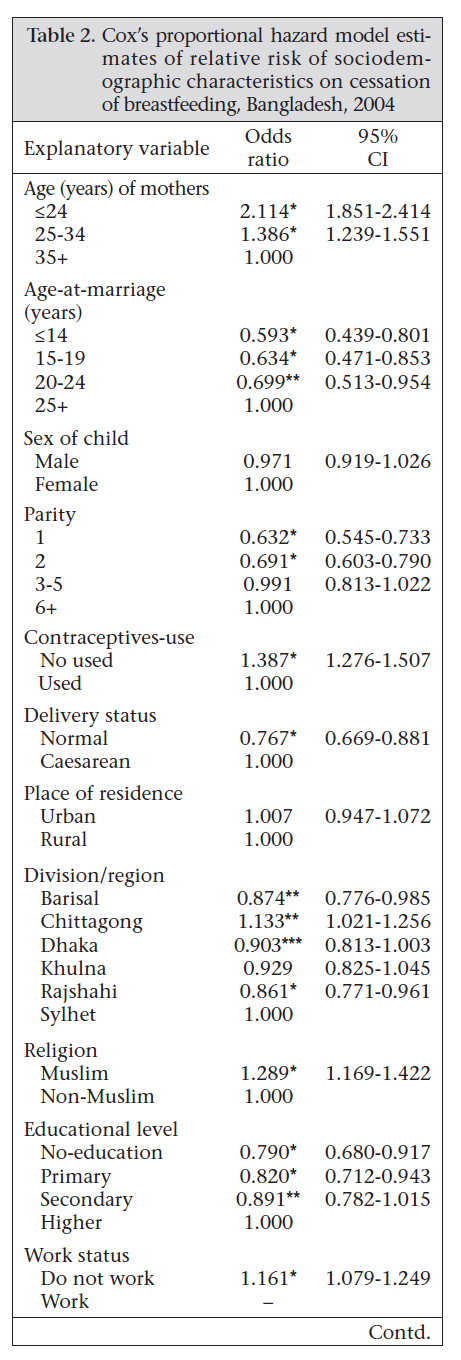
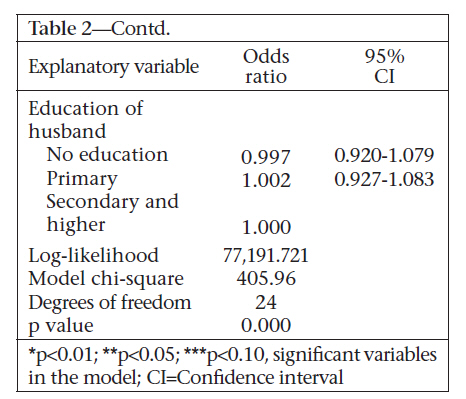
Data for the study were drawn from the Bangladesh Demographic and Health Survey (BDHS) 2004. Information was collected on education, age, reproductive behaviour, availability of family-planning supplies and services, breastfeeding, child health, and maternal status. The survey considered ever-married women of reproductive age as eligible for interview. A sample of 10,500 households was selected from which 11,444 women were interviewed. In total, 5,364 mothers provided information on the duration of breastfeeding for their last-born child at the time of interview. The maximum number of months of breastfeeding recorded in the survey was 60 but our study included the duration of breastfeeding up to 48 months and ignored the remaining months as outlier. Measurement of variables Dependent variable The duration of breastfeeding the last child of the respondent was the dependent variable which was calculated as the number of months that the mother reports having breastfed the child. Independent variables The demographic variables included age of mother, age-at-marriage, sex of child, parity, contraceptive-use, and delivery status. For analysis of data, the age of the respondent was categorized into three broad groups:≤ 24 years, 2534 years, and 35 years and over. The age-at-marriage was classified into four categories:≤ 14 years, 15-19 years, 20-24 years, and 25 years and over. The parity of mother in the sample was divided into four major groups: 1, 2, 3-5, and≥ 6. The category relating to contraceptive-use was dichotomous: not used and used. The delivery status was assessed as either normal or by caesarean section. The socioeconomic variables included place of residence, region of residence/administrative division, the highest level of education of the respondent and the husband, and occupation of the respondent. Education of the respondent is the highest level of schooling attained, measured as no education, primary, secondary, and higher; education of her spouse was also measured as no education, primary, secondary, and higher. Occupation of the respondent was also measured as a categorical variable: not working and professional/administrative, clerical/sales, skilled/unskilled manual, domestic, and others. Statistical analysis Bivariate and multivariate statistical techniques were used for studying the predictor variable— duration of breastfeeding—in relation to the explanatory variables. The variable—duration of breastfeeding—was coded as 0-12 months, 12-24 months, 24-36 months, and 36-48 months. The association of the duration of breastfeeding with all the independent variables in the study was first checked by the chi-square statistic. Life-table analysis provides a good understanding of breastfeeding behaviour over time. The factors affecting the duration of breastfeeding were investigated in a regression using Cox’s proportional hazard model (25). This model was used for determining the covariates that were significantly associated with the duration of breastfeeding. The data obtained were analyzed using the SPSS software (version 10.0 (26), Statistica 5.0, and Excel. Life-table technique A life-table can be constructed by pooling completed and censored cases of breastfeeding (27-28). The completed observations were those in which breastfeeding was stopped, and the exact duration of breastfeeding was known. Censored observations were those in which the child was still being breastfed at the time of survey. The mean duration of breastfeeding was used as the summary measures. Cox’s proportional hazard model Survival analysis technique was used in analyzing breastfeeding-related data. The survival analysis technique adjusts for truncation bias by incorporating both complete and incomplete segments of histories in the analysis of breastfeeding-related data (some mothers might be continuing to breast-feed at the time of the survey). The Cox’s proportional hazards (PH) model may be viewed as a multivariate life-table but unlike other regression techniques, this method uses censored data and, thus, controls for truncation bias (29). Descriptive statistics and the individual effects of Cox regression analysis for each variable are given to provide a general overview of the covariates in the analysis (30). The hazard function at time-point t (stopping or termination of breastfeeding), denoted λ (t,z), by is expressed as: λ (t,z) = λ0(t).exp ∑ Xiβi, where λ(t,z) is the hazard rate at time t, λ0(t) is the baseline hazard function of t, ßiis a vector of coefficients, and Xi is a vector of covariates. It is assumed in this model that: (a) there is a hazard or risk of occurrence of the event of interest (in this case, the termination of breastfeeding) at each time t, and this is applicable to all members of the population; (b) at each time t, the respondents at one level of a given subgroup experience a hazard proportional to the reference category; the models are a function of time and regressor variables; and (c) there will only be one set of coefficients. The hazard ratio (odds ratio) for breastfeeding and its 95% confidence interval (CI) were calculated for the sociodemographic factors associated with breastfeeding. RESULTS The figure shows the overall pattern of breastfeeding in Bangladesh. The survival curve represents the probability of mothers who continued to breast-feed at any given time. During the first month of life, the maximum (87%) probability of continuing breastfeeding was observed, which decreased dramatically after two years of age. The life-table analysis and its related measure (mean) for the duration of breastfeeding by various covariates of mother and child are shown in Table 1a & b. Bivariate analysis revealed significant differences in the duration of breastfeeding relating to place of residence, administrative division,deliverystatus, contraceptive-use, education of mother, education of husband, parity, and religion. The mean duration of breastfeeding in Bangladesh for surviving children is 31.9 months. It is comparatively higher among younger mothers (<25 years) than older mothers (=35 years). In this study, the mean duration of breastfeeding was 32.67 months for mothers of younger age-group, 31.4 months for middle-aged mothers, and 31.6 months for older mothers. Mothers who were married at an early age had a longer duration of breastfeeding than those who were married in older age. Mothers of single parity breastfed their children, on average, for 32.4 months; mothers of 2 parity breastfed for 32.0 months; and those with 3-5 parity breastfed for 32.1 months. This decreased to 31.8 months for those who had six and more children. The average duration of breastfeeding was 31.4 months for mothers who were not using any contraception compared to 32.1 months for those who were using contraception. The mean duration of breastfeeding was comparatively lower among mothers who gave birth by caesarean section (30.1 months) compared to mothers giving birth vaginally (32.1 months). The urban mothers breastfed their children for a relatively-shorter duration than did the rural mothers. Among the six administrative divisions of Bangladesh, the duration of breastfeeding was the lowest in Chittagong division (27.78 months). The non-Muslim mothers breastfed for a longer duration (36.13 months) than the Muslim mothers (31.53 months). Table 2a & b presents the results of the proportionality hazards model for the duration of breastfeeding. Age of mother, age-at-marriage, parity, contraceptive-use, delivery status, region, religion, education and occupation of mother were statistically significant. The odds of stopping breastfeeding for older mothers were lower than their younger counterparts. Women who married at an early age (=14 years) had a lower risk of stopping breastfeeding compared to women who married at an older age (25 years and over). Increased parity was associated with increase in the risk of cessation of breastfeeding. Normal delivery was associated with a 23% less likelihood of terminating breastfeeding compared to birth by caesarean section. Similarly, the use of contraceptives had a lower risk of stopping breast-feeding. The mothers of Chittagong and Sylhet divisions were more likely to terminate breastfeeding early compared to the mothers in other divisions. The Muslim mothers had 1.3 times higher risk of stopping breastfeeding than their non-Muslim peers. The risk of cessation of breastfeeding increased with increasing maternal education. Moth-ers not working were 1.16 times more likely to stop breastfeeding than working mothers. DISCUSSION The study examined the socioeconomic and demographic determinants of breastfeeding in Bangladesh. Breastfeeding is virtually universal (98.3%) and prolonged in Bangladesh. Past studies in Bangladesh found the mean duration of breastfeeding to be 26.4-28.9 months (30-33). It seems that the duration of breastfeeding in Bangladesh is gradually increasing. Increasing maternal age and parity can lead to breastfeeding of a shorter duration. Higher parity leads to shorter birth intervals and, hence, shorter time available for breastfeeding. It is also well-established that parity is closely related to maternal age (31). An older woman is more likely to have a greater number of children; hence, the demand on her time is considerable which may lead to early termination of breastfeeding. Poor nutritional status, particularly among older women, can diminish the capacity and the fat and vitamin content of breastmilk. The result is that not enough breast-milk will be provided to the infant, thus, hastening early termination of breastfeeding. In this study, mothers with 1, 2, and 3-5 parity were 37%, 31%, and 1% less likely to terminate breastfeeding than mothers with =6 parity, suggesting that an increase in parity is associated with a decrease in probability of terminating breastfeeding. Giving births to too many children might have caused physical complications and weakness to these mothers who were unable to breastfeed their children. Women aged =14 years, 15-19 years, and 20-24 years were less likely to terminate breastfeeding than women who were married at =25 years. The higher risk of terminating breastfeeding in mothers with first-born babies might result from two reasons. First, they belonged to younger age-group, and second, they neither had breastfeeding experience nor they feel comfortable in breastfeeding their children. The use of contraceptives plays a role in lengthening inter-pregnancy interval, and thus, mothers have time to breastfeed their children, consequently reducing the risk of termination. Region of residence of the respondents had a significant effect on the risk of termination of breast-feeding, for example, mothers from Chittagong were more likely to terminate breastfeeding than those from Sylhet. This is in agreement with the results of previous studies (10-11,30). One of the key determinants of the decline in breastfeeding in Bangladesh is the increasing level of education of mothers, a factor which plays a role in the adoption of modern ideas and which usually leads to the abandonment of traditional practices regarding childcare. A similar trend that higher education is associated with shorter duration of breastfeeding was also observed in some earlier studies in Bangladesh (10-11) and in other developing countries (34), although the scenario in industrialized countries, such as Denmark, appears to be the opposite (35). Results of a study suggest that education is a proxy for socioeconomic status, which could be related to exposure to advertisements and the capability to buy infant formula (36). The probability of terminating breastfeeding by Muslim mothers was higher compared to non-Muslim mothers (Hindu, Christian, and Buddhist). Working women breast-fed for a slightly longer duration compared to the non-working women, which is consistent with the findings of other studies (30,32). Women in Bangladesh are involved in traditional or informal work (agricultural activities, domestic work, jobs in cottage industries, and small-scale marketing, or as labourer), especially in the rural areas, and have more flexible schedules, and this allows them to nurse their infants more often, thus maintaining longer periods of lactation. The results of the present study indicate that the breastfeeding-promotion programme in Bangladesh should address mothers with higher education, those who have higher parity, give birth by caesarean section, and those living in urban areas and Chittagong since these mothers tend to breast-feed their children for a relatively-shorter period of time. ACKNOWLEDGEMENTS The authors thank the anonymous reviewers of this journal for providing insightful comments and suggestions for revision. REFERENCES
Copyright 2010 - Journal of Health Population and Nutrition The following images related to this document are available:Photo images[hn10077t2a.jpg] [hn10077t1b.jpg] [hn10077f1.jpg] [hn10077t2b.jpg] [hn10077t1a.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}