 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 1, No. 1, Dec, 2003, pp. 9-14 HOW SHOULD DOCTORS BE PAID? LESSONS FROM THEORY AND PRACTICE Peter O. Ogwang. Policy Analysis Unit. Ministry of Health Code Number: hp03005 Introduction For long now, doctors in Uganda have been complaining that their terms of service, particularly remuneration, are not commensurate with the years that they spend training and the amount of work that they do. This issue has persistently been raised at several fora over the years but with no definite resolution. But how should doctors be paid? This paper attempts to answer this question. In the developed world, policy makers attempt to answer the question of cost containment. In Uganda, due to limited financial resources, the overriding question is where will the extra resources to adequately pay doctors be found? Two further questions should be considered:
The main problem here is that payers (private or third party) for health services can only imperfectly observe the true costs borne by health care providers. In an attempt to solve this problem, two alternate strategies for controlling healthcare costs can be suggested. Demand-side cost sharing. Insurance against health care expenditure, in whatever form, creates incentives for over consumption of health care services, while limitations on this insurance, whether in the form of deductibles1, co-payments2, or coverage limits, force the consumer/patient generally to bear a greater risk of illness and monetary loss. So demand-side cost sharing can be used in an attempt to reduce consumption of health services, but it also imposes additional financial risk on genuine consumers. The overall result is that demand side cost sharing may do most to discourage care among the lower income groups in society. Supply-side cost sharing. Under supply side cost sharing, the provider of health care services bears some of the costs of provision of health services and so this attempts to alter directly the incentives facing the providers. If equity of access is accorded high weight, then supply side cost sharing will be superior to demand side cost sharing as a tool for cost containment and also as a tool for encouraging the lower income groups in society to seek health care freely. Using this back ground, supply-side cost sharing will form the basis of this essay, on how doctors should be paid. The main mechanisms of paying healthcare providers are;
Retrospective payment systems
Under this system, providers of health services are paid fees on a per service basis (“fee-for-service”), which are often set to equal, or to exceed the costs of each service provided. As such health care providers have economic incentives to supply whatever consumption level is desired by their patients. Hicks (Hicks et. al. 1987) compared the impact of a random assignment of 18 paediatric residents to either fee-forservice payment or salary. Results showed that fee-forservice physicians had more visits per patient enrolled in them (+22%) than salaried doctors did. In terms of continuity of care, results from another study (Kristiansen and Mooney 1993) indicate that patients were more likely to be seen by their regular doctor if he was under fee-forservice. For home visits, fee-for-service GPs were twice as likely to undertake a home visit and four times more likely to follow up patients at home rather than in the surgery. Disadvantages of the fee-for-service payment also exist. The health care providers will inevitably tend to provide services and patient days in excess of maximum quality of treatment. As well as having a lack of incentive to control the quantity of care delivered, this system offers no incentive to control the price of such care. Such a payment system provides no incentive for health care providers to be cost conscious. So healthcare providers can induce demand if they so wish. Furthermore, there is the issue of fee creep. Since it is very difficult to control the adequacy between the fee claimed and the service performed by the physician/doctor, an inadequate use of the fee schedule may arise. Indeed, the client/negotiator for health is usually in a situation of imperfect information with respect to the true costs incurred by the providers of healthcare. Consequently, the negotiation process is likely to lead to a biased structure of fees, some procedures becoming more lucrative than others are. Keeler and Brodie provide a good example of price distortions between procedures in obstetric decisions (Keeler and Brodie 1993). They compared the use of vaginal delivery versus caesarean section and indicated that the greater physician fee for caesarean section (an additional $500) is likely to be a significant factor in the choice between both types of treatment. Lastly, doctors will less likely delegate to other care providers as readily as if they were salaried or under capitation and this can lead to unfortunate incidences like the one that embarrassed Mulago hospital 2 –3 months ago when a woman in labour was left unattended to by doctors simply because her personal doctor was not available. She later passed away and her husband is considering suing the hospital for mal-practice. This system has however been the most favoured by many doctors in Uganda and is commonly in use in private clinics/health units and also in private wings of Government hospitals/health units. Prospective payment systems This payment system first came to light in 1983 introduced by Medicare in the USA. Under this system, payment rates are fixed according to the Diagnosis Related Group (DRG)3 into which the patient is classified on discharge. The prospective payment system was based on the idea that hospital “output”can be proxied by the number of discharges in various categories, and that manipulating payment incentives to hospitals could reduce the level and the rate of growth of cost. Consider for example a patient hospitalized for a prostatectomy. Under the fee-for-service system, the hospital receives additional funding for each day of care, each diagnostic test, and each procedure conducted. However, under the prospective payment system, the provider/hospital is given a lump sum payment equal to the national average of all patients who undergo a prostatectomy (with some adjustments). If the patient is less expensive than the average, the hospital earns a profit on that patient. If the patient remains in hospital for a long time, or undergoes unusually expensive procedures while in the hospital, then it earns a loss on that patient. The prospective payment system is intended to alter incentives to hospitals/health units and improve efficiency. The physicians are given incentives to control expenditure and develop more cost effective styles of practice. In economic terms, it can be interpreted as a form of provider/supply-side cost sharing. Once a hospital accepts a patient and qualifies for a DRG-based prospective payment, costs of treatment are borne by the hospital itself; if treatment costs for the patient go up by $1, the hospital’s net revenue for that patient falls by exactly $1. Furthermore, supply-side cost sharing can be imposed to reduce utilization without shifting costs to the patient, i.e. changing supply-side cost sharing does not impose financial risk to patients. This system that uses DRGs is non existent in Uganda and therefore not applicable to this situation. However it can provide some food for thought, especially for the increasing number of private hospitals. However more applicable to Uganda under the PPS are salaries and capitation. Salary and capitation (payment for a responsibility) type of payments can be taken to generally fall under the prospective payment system in as much as total physician remuneration is known in advance and the incentives facing physicians are related. In Europe, Kristiansen et al studied the impact on the use of laboratory services of different payment systems and found that the total number of tests per encounter was slightly lower among salaried GPs than among fee-for-service GPs (Kristiansen and Mooney 1993). Fitzgerald et. al. 1987 compared two cohorts of patients hospitalized with newly diagnosed hip fractures before-andafter the introduction of Medicare PPS in the USA. They controlled for age, sex, ethnic group, marital status and home support. Results showed that length of stay fell post PPS from 16.6 to 10.3 days. Number of physical therapy sessions fell post PPS from 9.7 to 4.9. The proportion of patients in nursing homes after discharge rose post-PPS from 13% to 39%. A big disadvantage of prospective payment systems, however, is that they motivate providers to select out the sicker patients who will prove unprofitable (Ellis and McGuire 1990). GPs in the U.K. were found to lack motivation under a capitation system. Stearns (Stearns et al 1992) analyzed the change within a Health Maintenance Organization from a fee-for-service based system for primary care physicians to a capitation payment, with no parallel system change for specialists (albeit a significant reduction in the level of fees: 50%). Beyond a reduction in hospitalization rates, the authors found that the number of referrals to specialists within the group increased significantly as a result of the change. Safran (Safran et al 1994) argues that little evidence exists to show that the success of prepaid care in relatively healthy populations can be replicated among sicker patients. They developed a comprehensive analysis of the quality of primary care in FFS Vs prepaid systems and the study design was centered around chronic patients. The authors looked at five dimensions of care; (1) accessibility, either financial (1a) or organisational (1b). (2) Continuity (3) comprehensiveness (4) co-ordination and (5) accountability; either interpersonal (5a) or technical (5b). To assess the effect of payment systems on each primary care dimension, the authors performed seven multivariate regression analyses, each with one of the primary care dimensions as the dependent variable. Independent variables included patient, physician and system characteristics. Results indicated that:
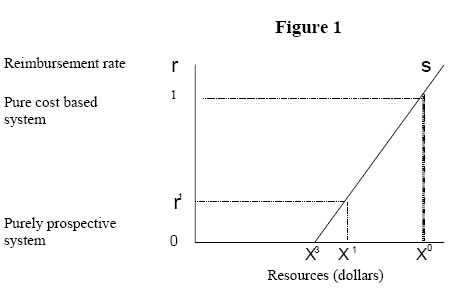
The results pointed to the difficulties of successfully incorporating each of seven elements of primary care into one payment system. In prepaid systems, we find increased financial access and improved co-ordination of care. However, these elements were countered by reduced patient-physician continuity and comprehensiveness of health care, in many cases, by diminished organizational access and interpersonal treatment that is less satisfactory to patients. This particular study is very relevant to the Uganda situation as the findings are what has been repeatedly found and reported by clients/patients. In Mulago hospital for instance, as an institution there is increased financial access and improved coordination of care but with reduced patient-physician continuity and interpersonal treatment is often less satisfactory for patients. Another difficulty with the PPS is that it may encourage providers to reduce the value of the treatment for which they receive a unit of payment by curtailing consultation time, leisure on the job, by excessive prescribing or by over-referral to hospitals. And yet consumers’choice of health care provider depends on the quality of care. This again is a common treatment outcome in Uganda whereby, again as for the case of Mulago hospital doctors don’t spend quality time with individual patients and also occasionally there is a lot of leisure on the job. Lastly, given the ability of healthcare providers to shape the amount of care provided, complete supply-side cost sharing may lead to some under provision of healthcare. On the relative merits of prospective Vs retrospective payment systems, neither system appears ideal. Mixed reimbursement We consider the two extremes of supply-side cost sharing as pure prospective payment (for the case of Uganda salaries and capitation) and pure cost based reimbursement (fee-for-service). Let; R = the lump sum payment under PPS (independent of costs) Then the total payment to the hospital per discharge; = R + rx When R>0, and r = 0, then s = 1. The system is then purely prospective. Mixed systems partly prospective and partly cost based are when R > 0, and 0 < s <1. An illustration of how supply-side cost sharing would perform in the market is depicted in figure 1 below; The supply curve above is an empirical relationship and indicates how the quantity of care supplied during a patient’s stay in hospital undergoing treatment responds to the degree of supply-side cost sharing. On the vertical axis is the reimbursement price r, and the horizontal axis measures the resources devoted to the patient’s care during the stay. This curve is drawn assuming there is no demand-side cost sharing. Resources labeled x0 refer to the amount of utilization with no supply-side cost sharing. A fully PPS with r = 0 and hence supply-side cost sharing equal to one would lead to x3. The desired quantity x1 could be implemented by a degree of supply-side cost sharing equal to r1. So basically what this figure shows is that the quantity of services supplied to an individual seeking treatment will tend to rise as the degree of supply-side cost sharing falls, and as the system moves away from prospective payment and toward cost-based reimbursement. So then for the case of Uganda, obviously the desired level of resource commitment to patients seeking health care would be x0, but this involves patients paying fees-forservices. But due to socioeconomic reasons, this is not possible. The best alternative would therefore be a compromise, like r1 and x1. A healthcare provider acting as an agent on behalf of an imperfectly informed patient, as long as the benefit to the patient has some weight in the objective function of the healthcare provider, then increasing the marginal reimbursement to providers will increase the desired level of services provided, since additional benefits to the patient (which also provides utility to the provider) can be purchased at lower cost. Krasnik et. al. 1990 investigated the effects on GP’s activities of a change in their remuneration from a capitation based system to a mixed FFS and capitation based system in Denmark. The study covered three periods; one period before a change in their remuneration system and two periods after, with a control group of GPs with a mixed fee per item and capitation based system throughout, in Copenhagen County. (The index group was in Copenhagen City.) The main outcome measures were the number of consultations (face to face and by telephone) and renewals of prescriptions, diagnostic and curative services, and specialist and hospital referrals per 1000 enlisted patients in one week (table 1 below). Table 1. Effects on GP’s activities of a change in their remuneration
The results showed that total contact rates per 1000 patients listed rose significantly compared with the rates before the change index in the city (100.0 before the change Vs 111.7) and over the same time in the control group (100.0 Vs 106.0), but within a year these rates fell to 104.2 and 104.0 respectively. There was an increase in consultation by telephone initially but not there after. Rates of examinations and treatments that attracted specific additional remuneration after the change rose significantly compared with those before. Referral rates to secondary care fell. They concluded that introducing a partial fee for service system seemed to stimulate the provision of services by GPs, resulting in reduced referral rates. Conclusion Since neither a purely cost-based nor a prospective payment system is likely to be ideal, the best alternative then seems to be an intermediate level of supply-side cost sharing in one form or another. A solution should logically be found in mixed prospective and retrospective systems of payments, which will attempt to bring in incentives for performance and cost control. Siegel et al. (1991) use an empirical Bayesian approach to demonstrate that given that hospital costs attributable to a given patient are only imperfectly observed, the fairest reimbursement system is one that uses a weighted average of the patient’s own cost, the cost of other patients in the hospital, and some average using other hospitals (such as a regional or national average). Several real-world reimbursement systems employ intermediate levels of supply-side cost sharing. Most Health Maintenance Organizations in the USA accept a fixed annual capitation payment for each enrollee, and are often responsible for all costs that enrollee may incur during the year. Many HMOs then compensate their physicians using a financial incentive system that include both a salary payment and a payment based on the volume of services provided. Danish physicians are paid using a formula under which 75% of their earnings are from fee-for-service and 25% from lump sum payments based on the total number of enrollees under their supervision (“capitation”payments). This new payment formula, together with their budgeted payments to hospitals, appears to have helped Denmark control its health costs (Abel-Smith, 1992). Typically, in Uganda, the Government health system pays doctors a fixed salary regardless of how many patients they see or the quality of care they provide and this gives doctors little motivation to improve performance. As a result, a majority of the doctors work in the public sector but at the same time moonlight in the private sector receiving both salary/capitation and fee-for-service/retrospective payments. However there are also some doctors who are exclusively in the public sector receiving salary/capitation, and also others exclusively in the private sector receiving fee-for-service and prospective payments. Clearly the retrospective payment system (fee-for-service) would suit most doctors best, since one of their biggest complaints is that they work hard and long and yet they are paid very little. This would also encourage them to see many more patients than they usually see. But the down side to this, especially if there is little supervision as already discussed above, is that doctors will end up providing services and in-patient days in excess of maximum quality of treatment. Price control and lack of delegation will also definitely be problems. However most worrying will be the issue of “fee-creep”, were some procedures will inevitably become more lucrative than others, e.g. there might be many more caesarean sections seen more than normal deliveries because of the better paying nature of the caesarean sections. The better approach would therefore probably be to strengthen the prospective payment system (salaries/capitation) that forms the biggest system for paying doctors in Uganda. However a pure PPS system, where suppliers of medical care are salaried employees causes lack of incentives to provide services as already mentioned above resulting in artificial shortages and queues on the demand side. More important, actors in such a system lose interest in innovation of any type. But better still, there are options that government can still take to officially introduce an appropriate system with a “blend”/”mix”of the different systems which will ensure that there is fairness to consumers and also better access; and also reduce on provider risk and increase fairness in payment to providers. This would involve supporting the salary and capitation systems and also accepting a supervised retrospective payment system, like occurs in the private wings of government hospitals. As shown in figure 1 above, this will also increase on the amount of resources dedicated to patients seeking health care. The private hospitals should also consider adopting the DRG system as a way of altering their incentives and improving efficiency. This would however, amongst other things, require a fairly good degree of knowledge about actual costs of production of different hospital services. These are sometimes very different from one hospital to another in relation to many factors. It would, in such circumstances, be difficult to have a standard DRG approach. Negotiations are still ongoing; we need to await the outcome. The key word here is incentives. In particular, it seems that the stronger the incentives are, the less payments are made on inputs (factor inputs, actual cost) and on activities (services provided), and the more the system depends on output quantities (treatment cases, patients to be treated). It is the task of the political decision-makers to devise such an appropriate payment system, which will seek to make doctors more responsive and accountable for the work they do by tying compensation directly to performance. Notes: 1 The amount of health care charges for which a beneficiary is responsible
before the insurer begins payment. References
Copyright 2003 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp03005f1.jpg] |
| |||||||||

{kind=link}