 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 2, No. 1, April, 2004, pp. UGANDA’S MINIMUM HEALTH CARE PACKAGE: RATIONING WITHIN THE MINIMUM? Freddie Ssengooba, Lecturer, Institute of Public Health, Makerere University Medical School, Uganda. Code Number: hp04005 Abstract Essential/minimum health care packages (MHCP) have appeared on the primary health care scene as a means of setting priorities for national health budgets. A technical approach of cost-effectiveness was sought to guide the political and group bargaining approaches. In Uganda, the application of the cost-effectiveness techniques seem not to have had an effect on the priority setting. A package of minimum services that is written into the sector plan has turnout to be more then the resources available in the medium term. At the operational level, the delivery of the minimum package has been rendered ineffective and inefficient, by trying to attain universal access with $ 8 per capita instead of $28. System capacity constraints for effective and equitable delivery of the MCHP are traced at the infrastructure-based planning and in explicit and implicit re-prioritization and rationing within the minimum package. Introduction
The overriding aim in setting an essential or minimum health care package (MHCP) is for the state to guarantee free access of its population to a set of health services it can afford. In essence, the minimum health package represents a health insurance that the state provides its population (WHO 2000). The purpose of developing and using the minimum package approach was to assist in resource allocation in the health sector especially in the face of a huge and growing health burden that has to be addressed with small public budgets, that characterize developing countries like Uganda. Due to demographic changes, lifestyles like obesity and smoking, and new technology and information, the health care needs are increasing at a pace that is not matched by the growth of the national budgets. The MHCPs is an explicit rationing of health services by the state. Services that fall outside the boundaries are not guaranteed to the population and therefore additional financing (e.g. private insurance or out-of-pocket payments) are needed (World Bank 1993). The flip side of this is that the state, by defining a minimum package, commits itself to make this package available and effective to all those in position to benefit from it. The aim of establishing MHCP is also to achieve the best possible value for available resources by allocating them to interventions that have the most benefits in improving population’s health. This "costeffectiveness" approach, it is argued, is preferable to alternative approaches to setting priorities in the health sector (World Bank 1993; Mahapatra 2002). Priority setting in health sector
Sometimes decisions regarding allocation of resources are ad hoc, based on professional opinions or on strong lobby groups, political expediency or outright public hysteria. For example, the most important single determinant of the annual health budget and its composition, for most districts in Uganda, is the previous year's expenditure pattern with some marginal additions to compensate for inflation and budget growth. This basis of allocation creates a financial inertia that perpetuates the deficiencies and inefficiencies in the system. Governments of developing countries are also usually sensitive to international initiatives and fashions as to what deserves priority in the health sector at any given time. External assistance through the earmarking of loans and grants influences country priority setting. For example, Global Fund to Fight HIV, TB and Malaria and other grants for HIV/AIDS have raised the priority of these conditions even when the ordering of needs at the population level may have been different. Provision of ARVs now tops the list of health system concerns and MOH has pronounced its commitment to provide universal free access to ARV to all persons living with HIV despite statements to the contrary in its Health Sector Strategic Plan (MOH 2000). The commitment in rolling out ARVs in the Ugandan health system although carries tremendous public health benefits, is an example of international priorities confronting national systems starved of resources to address their own set of needs. Unfortunately, health priorities stemming from international agencies with resources may not always be derived from studies of cost-effectiveness, but often from implicit judgments such as the threat of contagion that "global village" imposes on the international community as reflected below: "Recognizing that, in an age of worldwide travel by people from all over the world, disease can move rapidly from country to country and continent to continent, so that the health of Americans is intricately interwoven with health measures taken elsewhere, …..applaud President Bush's initiative proposing $15 billion over the next five years for prevention and treatment programs for HIV/AIDS and other serious infectious diseases in fourteen countries" (UNA-USA 2003) Other considerations that may influence the definition of health priorities are: the perceived interest of the politicians, medical profession and other groups in society. All these stakeholders have own interests in the priority setting process ranging from having access to complex medical technology for doctors and medical workers, ideological standpoints of the government lobby groups and political capital for politicians. Others may champion issues of equity, patients and provider’s rights and freedoms. Resource allocations based on such consensus decision processes have in the past been a source of inefficient budget allocation. For example, inappropriate large share of resources at tertiary hospitals around the world reflect the strong lobby of the powerful medical professionals who seek to adopt more technology and professional status accruing from extensive technical capacity of the hospitals even when needy clients cannot afford such hospitals (Cooper 1990). Despite the aforementioned influences on the health priority-setting context, over the past 10 years, major progress has been made in evaluating the health needs at the population level and developing the appropriate interventions for addressing them. The World Bank and WHO set out a process for establishing a rational and globally applicable method of guiding priority setting by using objective and technical criteria. This process has variously developed measures of effectiveness from health interventions which includes quality adjusted life years (QALY), disability adjusted Life years (DALY) and most recently, the health adjusted life expectance (HALE) (Mahapatra 2002). However, the measures have been in a state of flux indicating the difficulty of having very technical tools that can be applied across different countries, health, culture and value systems (Reidpath 2001). Economic evaluation of interventions and programs, mainly through cost-effectiveness analysis, has been introduced and applied more widely. More importantly, the rationale of economic evaluation is slowly permeating the process of decision making in the Ugandan health sector (MOH 2003). The socio-political dimensions of priority setting
Resource allocation is essentially a socio-political process although technical inputs such as cost effectiveness are important for evidence-based policy making (Walt 1994). Political expedience tends to drive the package beyond the available resources due to the distasteful concept of rationing in the political debates especially due to strong lobby groups such as women and human rights activists (Tengs 1996, Maynard 1998). Universal access to all possible care is commonly implied although the way the health system is planned, financed and its overall capacity grossly reduces this scope by adjusting both service quality and availability. As a product of the cost-effectiveness approach to priority setting in health care, a list interventions are identified that provide the best value for money in achieving the most reduction in the disease burden. The overall principal in constituting the minimum package is to match the package of interventions with the available resources (financial human and technology). The process of matching the interventions with resources is a technical process whose tools are limited to mostly to two dimensions: 1.) what the costs of interventions are, and 2.) how effective are the interventions in improving health status. Most of these are derived from ideal contexts that do not pertain in Uganda. On the political side, however other dimensions are needed. For example, is access to services equitable? To the individuals using the services, the convenience of access, the out-of-pocket expenditures and the utility/benefits derived from using the interventions are major consideration. In this paper an attempt is made to illustrate how the priorities set using the technical measures above (ie costs and effectiveness) may not have been usefully applied in Ugandan context. Data from national surveys is abstracted as indicative of the problems and promise in the minimum package approach. The paper tries to illuminate the problems, both in the technical processes of evaluating costs and effectiveness of interventions as well as in the process of planning and delivery of actual services that make the approach of fail to deliver better health. The paper argues that MHCP approach as used in Uganda’s health sector strategic plan far outstrip the available resources in the short and medium term, and can not be guaranteed by the state. The paper also illustrates the access problems that arise due to explicit and implicit rationing that takes place as attempts at policy and provider levels are made to provide a minimum package estimated at $28 per capita with only $8 par capita currently available (MOH 2002). System financing and the minimum health care packages
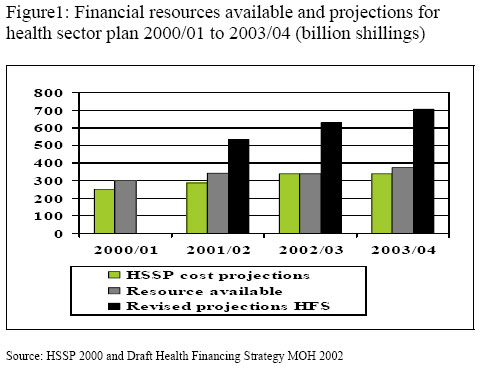
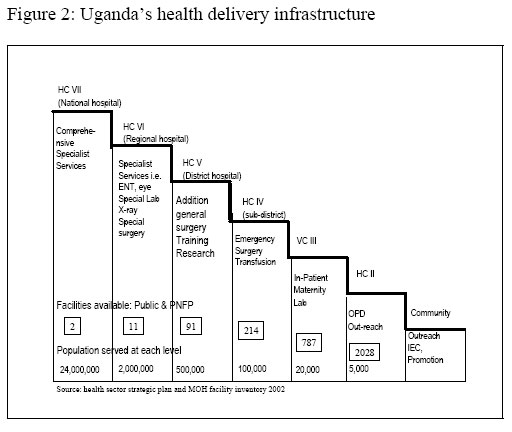
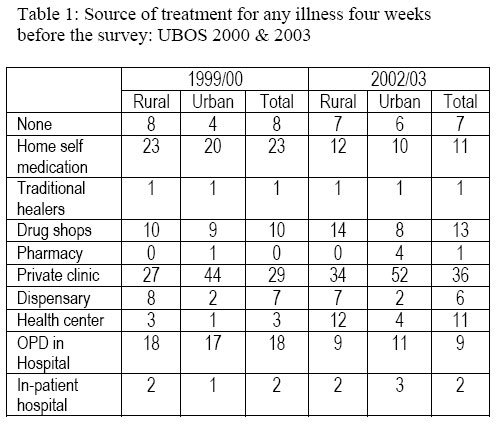
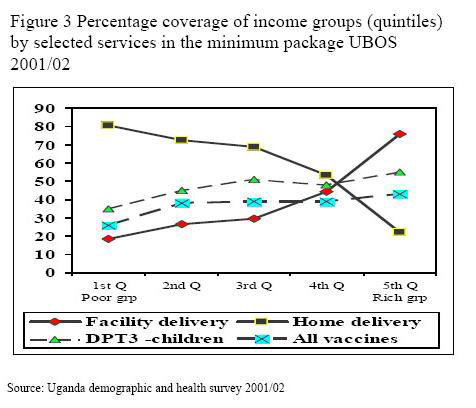
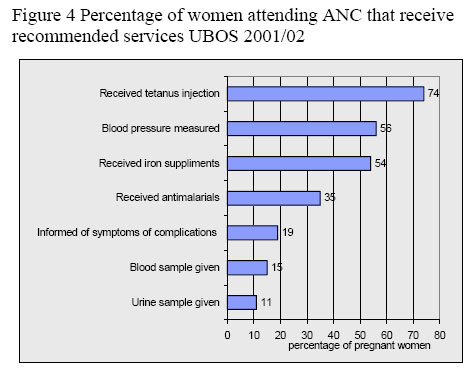
The MHCP services typically include preventive services such as childhood immunization, health promotion and education as well as treatment and control of common and infectious disease such as malaria, HIV/AIDS and TB. The use of MHCP presupposes three main issues: 1) that government has a good estimate of the resources that are going to be available for health service delivery, 2) that the delivery system has the capacity to deliver the package of services, and 3) that the costs of the services to be delivered and their benefits to the population are available. Mostly due to lack of reliable cost data about interventions effectiveness in Ugandan context, the selected interventions are of unknown effectiveness in the local circumstances and have turned out to be beyond the reach of available resources as reflected in figure 1. The process of costing the minimum health care package (MHCP) seem to have been understood as equating health budgets to projected resources for Health Sector Strategic Plan (HSSP) without duly costing out the interventions as envisaged in the HSSP. This seems to be the best explanation for the near perfect match between cost projections in HSSP and the resources that have been allocated overtime. But as shown in figure 1, efforts in 2001/02 to cost out the needs of HSSP in the health financing strategy (HFS) indicate a technical flaw in identifying the minimum package, i.e. that the minimum package is set before its costs (and presumably its effectiveness) are fully understood. Should the government commit itself to provide a minimum it can not afford? Rationing within the package Given the inadequacy of the resources to shoulder the MHCP as designed in the HSSP, there is a re-prioritization with an explicit and implicit rationing process within the package of services and across population coverage. It is this re-prioritization that in part works against quality, equity and utility of benefits to the users. Figure 2 illustrates the hierarchical nature of the Ugandan public and PNFP health care infrastructure. Given the infrastructure plan, a comprehensive MHCP is only available from functional Health Center IV and at hospital levels. Hospital services are by plan mostly in major urban/township centers. With the majority of the people living in rural areas with significant costs for time and travel to attend hospitals in towns, the infrastructure plan rations hospital care using distance, travel and time costs. The National Household Survey 2002/03 indicate that the mean distance to a hospital is 13Km and 6 Km for rural and urban population respectively. The mean distance to clinics, dispensaries and health centers are 4 km for rural households and between one and three kilometers for urban generally ignored although such costs tend to be much higher than user-charges paid to providers (Levin, 2003). Service guidelines that recommend multiple clients’ visits to the facility to receive interventions are bound to have compliance problems or are likely to attract the wealthier groups (Buor 2003; Okafor 1990; Muller 1998). On average, 49 percent of Ugandans are within a 5 km distance from a health facility. Given that health facilities have different service profiles and capacity, the coverage and quality for the complete range of MHCP is much less. The National Household Survey results presented in Table 1 indicate curative service coverage at household level (UBOS 2001). Overall, only about 30 % of the population enter the health system through which the government channels its services, both public and PNFP. Judging from these results, 70 % of the population that stand to benefit from the basic curative care are not reached by the public investments in health services. The majority of both rural and urban populations are seeking services in the private clinics and drug shops, or self medicate at home. These sources of care attract out-of-pocket payments on the part of the households and are a reflection of inadequate coverage and or quality of the curative services delivered through the public and PNFP sectors. The survey trends indicates that curative service utilization at the Health Centers has increased by four fold between the 1999 and 2002 while hospital OPD utilization reduced by a half. This trend represent an optimistic trend of taking the minimum package further down the infrastructure hierarchy and closer to the population. Indeed, the survey indicates a reduction in the self medication practice of about 50 percent. Of concern however, is the increase in the percentage of the population using the private clinics. The percentage increase in the use of the private clinics and drug shops between the two survey points is highest for the rural population i.e. 30 compared to 25 percent for the rural and total population respectively. This utilization pattern implies a mixed system of service provision and a failure of universal access to provide free services as implied in MHCP. The predominance of out-of-pocket sources of medical care implies high health care costs to households with their attendant effects of impoverishment and inequity (Wagstaff 2002). Inequitable pattern of access in the utilization pattern across different social economic groups is illustrated by access to specific interventions in the minimal package assessed in the Uganda Demographic and Health and Survey 2001/02 (Figure 3). The households in the wealthiest twenty percent of the population (quintile) consume more of these services in the minimum package than their poor counterparts. This finding illustrates the equity implications of the rationing process that takes place due to the combined factors of infrastructure plan/geography, information/education, and socioeconomic status. Rationing quality of services Although rationing on the basis of quality is ethically unacceptable, it is implied in the MHCP approach adopted in Uganda. The operational policies have explicitly sought for low-cost substitutes to health care with clear quality tradeoff. For example, huge investments were directed into training traditional birth attendants (TBA) in attempts to bring down maternal mortality while little efforts were paid to scaling up midwifery training, motivating rural deployment nor provider performance incentives (Kyaddondo 2003). At the inception of the TBA approach, cost-effectiveness was implied (WHO 1982, Hoff 1997). In the last couple of years, the Ministry of Health has sunk over two billion shillings "professionalizing" nursing aids as another explicit strategy for substituting professional cadres in hard to reach areas. These operational policy decisions to delegate professional tasks to less competent cadres are examples of how quality of care is explicitly rationed by the state. Other forms of rationing are more implicit. The budget ceilings that are imposed on the planning units by the treasury is an implicit form of rationing. The effect this has is usually felt in terms of shortages of drugs and supplies at the facility levels but also outright ineffective therapeutics options dispensed. Health providers through their autonomy in clinical judgment assign patients of different social-economic status to different treatment options. For example, patients with ability to pay receive prompt care procedures while the poor ones wait longer or never receive some of the standard services (Ssengooba et al, forthcoming). Figure 4 illustrates that there are marked quality gaps for one of the simplest (and one of the most consumed) interventions - antenatal care in the MHCP. Such quality shortfall cannot be attributed to providers conspiring to ration the service but rather inadequate inputs available to providers to observe the recommended standards of care. Conclusions
Rationing in infrastructure development, financing and quality of care has made the minimum package ineffective and inefficient. Poor targeting of the package to the poor/vulnerable groups means that the groups with the highest capacity to benefit from the package are not the largest beneficiaries of the interventions. The Uganda Participatory Poverty Assessment exercise identified ill-health as the main cause of impoverishment at households (MOFP&ED 2003). With the kind of results shown in this paper, it should not surprise policymakers that the National Household Survey 2002/03 has confirmed that poverty is on the increase (UBOS 2003). With a goal to contribute to poverty eradication, the health sector needs to ensure that it refines the service package in accordance to the system capacity for financing, human and technology context, and focus on delivering an effective minimum package but not to attempt to cover more ground by giving less or differential quality. For the health sector to make a contribution to reducing poverty it should re-examine the minimum package approach to improving population health. With the modest resources available in the short to medium term, it may be best to focus resources to meeting the needs of the poor and vulnerable groups. An explicit and vigorously pursued targeting is needed. As the rationing experiment in the Oregon state in USA showed, it is cost-effective to narrow the benefit package and pull into the system the poor and vulnerable groups than to flung the gates open for universal access, especially when the system resources can not cope (Maynard 1998). The relative success of the Oregon experience implies that benefit analysis should applied to population of beneficiaries i.e. the groups that stand to benefit most in improving the aggregate population health (Tengs 1996). As the findings on the infrastructure plan indicate, targeting the most needy should encompass a policy decision to reduce access costs to services for the rural population. PHC "without walls" approach is needed to take the action at the level of the beneficiaries. Such a policy would entail a pro-community planning and financing as opposed to the facility-based approach. For example, Navrongo Health Project in Ghana has succeeded in taking services of nurses and midwives to the communities with impressive health results. After about 3 years, the community-based approach to service delivery reduced childhood mortality by 38 percent among remote district population (Phillips 2003). A community-based approach has the potential to identify workable strategies in different localities to effectively link with facility-based services. In the short term, efforts to expand and commit resources to outreach services can reduce the inherent barriers to accessing a large number of interventions in the minimum package. The innovations in the delivery strategies not withstanding, significant increase in the financial and other resources will be needed for the minimum package in its current scope, more so if the universal access remains the goal. Failure to align the resources to a feasible range of interventions and to target them where they are needed most, will mean that it will be impossible to buy a $28 package for every Ugandan with a purse of $8 per capita. References
Copyright 2005 - Department of Health Sciences of Uganda Martyrs University |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}