 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 2, No. 1, April, 2004, pp. PRIMARY HEALTH CARE AND SECTOR-WIDE APPROACHES
Murindwa Grace, Health Planning Department, Ministry of Health Code Number: hp04007 Abstract
Primary Health Care and Sector-Wide Approaches to health development are among the major health sector reforms that have been undertaken in Uganda aimed at building a strong and cohesive health system. Inevitably, these reforms presented big challenges and some of the challenges still exist; however, there have also been encouraging achievements, which have showed that undertaking the reforms was the way forward for the health sector. Introduction
Primary Health Care (PHC) and Sector-Wide Approaches (SWAps) to health development are among the major health sector reforms that have been undertaken in Uganda. Both reforms are aimed at building strong and cohesive health systems for delivering health services to improve the health status and well being of the people. Primary Health Care
At Alma Ata in 1978, PHC was declared as a strategy to be adopted by all countries. PHC was defined as essential health care based on practical, scientifically sound and socially acceptable methods and technology, made universally accessible to individuals and families in the community through participation and at a cost that communities and country can afford to maintain at every stage of their development in the spirit of self-reliance and self determination. Four basic principles underlie the PHC approach. These are universal accessibility and coverage in relation to need; community and individual involvement and self-reliance (establishing firm roots within the community with active involvement of the people); Intersectoral action for health (coordination and collaboration with other sectors) and appropriate technology and cost-effectiveness in relation to the available resources. PHC was an innovative approach with the main thrust of strengthening health systems to provide comprehensive health services but with emphasis on preventive, promotive and rehabilitative health services, to address the main health problems in the community. The PHC approach is therefore more than the provision of "primary level services". It envisaged a seamless referral system from the community all the way to the most sophisticated health care available. Implementation of PHC required an extensive network of functional health infrastructure, with referral networks to provide a continuum of care. It required comprehensive planning and a lot of resources, which most developing countries didn’t do or have. With the assistance of multi/bilateral agencies, many countries established vertical programmes, mainly disease specific interventions, as a way of providing the preventive and promotive health services. At that time, another argument about whether to adopt selective PHC or comprehensive PHC raged on. For Uganda, the preference tended to be selective PHC, which effectively introduced many vertical programmes. These vertical programmes were piecemeal interventions, which did not result in the envisaged improvements in peoples' health. Instead, these programmes fragmented health services. Sector-Wide Approaches
After 20 years, since the inception of PHC at the Alma Ata conference, the Sector Wide Approaches (SWAps) were born in an attempt to address some of the shortcomings of PHC. SWAps are defined as a sustained partnership, led by national authorities, involving different arms of government, groups in civil society, and one or more donor agencies, with the goal of achieving improvements in people’s health and contributing to national human development objectives and in the context of a coherent sector, defined by an appropriate institutional structure and national financing programme through a collaborative programme of work. For the health sector, the policy objective of adopting SWAps was to provide an enabling environment that would allow for effective coordination of efforts among all partners in Uganda’s national health development, increase efficiency in resource application, achieve equity in the distribution of available resources for health and effective access by all Ugandans to essential health care (MoH 1999). Principles of SWAps
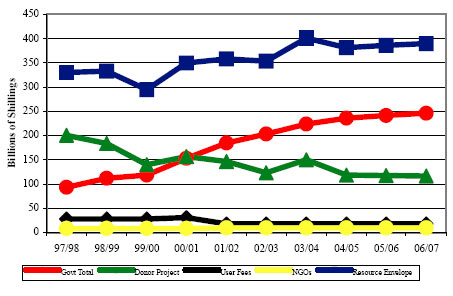
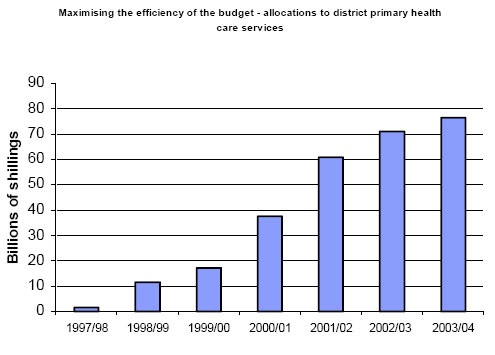
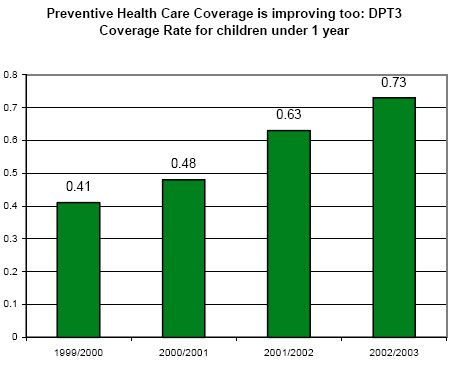
SWAps are bound by the following principles: all investments in the health sector would follow an agreed programme of work; all the partners in the SWAps arrangement should agree on common management arrangements (i.e. on a framework for monitoring sector performance, on financial management, and on procurement of goods and services); funding for the implementation of the programme of work should be channelled through government systems (central budget support), in effect and crucially, this discourages project funding; and lastly, there should be partnership agreements and working arrangements amongst the different partners. Implementation of SWAps in UgandaA comprehensive programme of work, the Health Sector 450 Strategic Plan, was developed through a consultative 400 process between the Ministry of Health, related ministries, the development partners and other stakeholders. This collaborative undertaking agreed on the common management arrangements with regards to planning, budgeting, disbursement, procurement, reporting and monitoring. These common working arrangements are employed with the objective of using and strengthening existing Government of Uganda systems and structures. Development partners are encouraged to fund the Health Sector Strategic Plan through Central Budget Support in line with the Government of Uganda strategy towards Comprehensive Development Framework. However, in the interim, the Government of Uganda has adopted a flexible approach to give time to development partners to adjust to the new arrangements (MoH 2000). Accordingly, the modalities for funding the HSSP are: central budget support; district budget support; and projects. The Statement of Intent was signed to proceed with a sector-wide approach. Structures for overseeing SWAps implementation were set up and these include: The Health Policy Advisory Committee; The Health Sector Review Committee; Joint Supervision Missions; The National Health Assembly; and Sector Working Groups. A Memorandum of Understanding (MoU), which governs SWAps implementation, was signed between GoU and partners. Achievements It has raised the status of health among donors, administrators and politicians and also strengthened partnerships between government and all stakeholders in health. There has also been increased mobilisation of resources for health. Big and well-funded health programmes were established to address the major health problems, and most of the funding for the programme of work (HSSP) is now being channelled through central budget support (GoU budget) rather than projects, as is shown in the figure below. (Figure) Further, the working arrangement has seen funding for PHC becoming a priority for GoU and partners, and this is being channelled through the Poverty Action Fund (PAF). The proportion of the health sector budget allocated to district Primary Health Care has increased from less than 20 billion to nearly 70 billion in the financial year 2003/04 as is shown in the figure below. Dramatic increases are seen from about the time that SWAps are introduced and adopted (FY 2001/02). (Figure) There has also been improved accessibility and coverage of the population to the basic health services; rural populations have especially benefited. The accessibility to health facilities (within 5 km radius) has increased from 49% in 1999 (pre- HSSP) to 69.5% in 2001. Further, more health units have been constructed since then and access is estimated to have increased to approximately 72%. This collaboration has witnessed improvements in service delivery outputs, both preventive and curative services. The figure below shows the steady increase in DPT3 coverage rates for children under 1 year over the years, more so in the years following the introduction of SWAps. (Figure) Further, as is again shown in the figure below, the new OPD attendances in both public and PNFP units have also gradually been increasing over the years with dramatic increases in the years immediately following the introduction of SWAps. (Figure) There has been improved integration of health service delivery. All health facilities provide curative, preventive and promotive health services, and a Minimum Health Care Package (MHCP) was adopted to be delivered by every health facility. Further, planning and resource allocation for health service delivery (MHCP) are done by level of care (service delivery points). Lastly, there is improved and streamlined monitoring of the health sector performance. A framework and indicators for sector performance were agreed upon and donor supervision and monitoring missions have been greatly minimised. Challenges
Challenges also exist. First of all, there are still inadequate resources to fully implement both PHC and SWAps. Secondly, project funding is still persisting and especially global initiatives have been more difficult to incorporate in the HSSP. Thirdly, intersectoral collaboration remains a very big challenge. Functional linkages have not yet established. Human resources for health, especially trained health workers to deliver health services, particularly the Minimum Health Care Package, remain inadequate and this has presented a big challenge to the health sector. Finally, the health information systems, especially from communities, have remained problematic in terms of data collection, analysis and eventual utilisation of this data to improve on health services. Conclusion
PHC and SWAps have been some of the major health sector reforms ever undertaken in Uganda. Both reforms were aimed at building strong and cohesive health systems. Building on the foundation and experiences of PHC, SWAps should establish strong and robust health systems able to deliver health services and improve the health status and well being of the people. References
Copyright 2005 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp04007f3.jpg] [hp04007f4.jpg] [hp04007f2.jpg] [hp04007f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}