 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 2, No. 1, April, 2004, pp.33-39 THE EFFORT TO ACHIEVE THE MILLENIUM DEVELOPMENT GOALS IN UGANDA: REACHING FOR THE SKY? Christine Kirunga Tashobya1 and Peter Ogwang Ogwal2
Code Number: hp04010 Abstract At the United Nations Millennium Summit in September 2000, world leaders placed development at the heart of the global agenda by adopting the Millennium Development Goals (MDGs). The Government of Uganda is a signatory to this and the Poverty Eradication Action Plan (PEAP), which is also the Country's Poverty Reduction Strategy Paper (PRSP), is Uganda's national development framework and medium term planning tool to achieve the MDGs. In the health sector, targets are not yet being met. Introduction
At the United Nations Millennium Summit in September 2000, world leaders placed development at the heart of the global agenda by adopting the Millennium Development Goals (MDGs). The goals set clear targets for reducing poverty, hunger, disease, illiteracy, environmental degradation, and discrimination against women by 2015. In support of these Goals, United Nations (UN) Secretary-General launched the Millennium Project to recommend the best strategies for achieving the MDGs. The Millennium Project's mandate focuses on identifying the operational priorities, organizational means of implementation, and financing structures necessary to achieve the MDGs. The Goals, and the commitments of rich and poor countries to achieve them, were affirmed in the Monterrey Consensus that emerged from the March 2002 UN Financing for Development conference, the September 2002 World Summit on Sustainable Development and the launch of the Doha Round on international trade. World leaders from countries rich and poor described the Monterrey conference as marking a compact between them in support of shared development goals. That commitment forms the basis for the Millennium Development Compact; a Compact through which the world community can work together to help the poor countries achieve the Millennium Development Goals. This compact calls on all stakeholders to orient their efforts towards ensuring the success of the Goals, in a system of shared responsibilities. Poor countries can insist on increased donor assistance and better market access from rich countries. Poor people can hold their politicians accountable for achieving the poverty reduction targets within the specified timetable. And donors can insist on better governance in poor countries and greater accountability in the use of donor assistance (UN, 2003). Breaking out of poverty traps requires a multifaceted approach, and one of the six policy clusters recommended by the Compact is investing in human development – nutrition, health (including reproductive health), education, water and sanitation – to foster a productive labour force that can participate effectively in the world economy. This needs to be bolstered by much larger donor contributions before economic growth takes hold. Indeed, because better health and education are both goals of human development and precursors to sustained growth, investments in these areas are important for a later takeoff in private activities (UN, 2003). The importance of the MDGs in health is, in one sense, self-evident. Improving the health and longevity of the poor is an end in itself, a fundamental goal of economic development. But it is also a means to achieving the other development goals relating to poverty reduction. The linkages of health to poverty reduction and to long-term economic growth are powerful, much stronger than is generally understood. The burden of disease in some low-income regions, especially sub-Saharan Africa, stands as a stark barrier to economic growth and therefore must be addressed frontally and centrally in any comprehensive development strategy. The Compact requires development stakeholders to adopt a goal-oriented approach to policy and practice, and to consider, amongst other issues - can a country achieve the MDGs under current constraints? What needs to be done for each country to achieve the MDGs? Health MDGs
The MDGs have provided the world with measurable goals and even global targets based on which countries are supposed to develop national targets. Of the eight MDGs 4 are particularly health-related, although all of them have a relationship with health in one way or the other. Goal 4 focuses on the reduction of child mortality. The target of the goal is to reduce by two-thirds, between 1990 and 2015, the under-five mortality rate. Goal 5 targets the improvement of maternal health. The target of this goal is to reduce by three-quarters, between 1990 and 2015, the maternal mortality ratio. Goal 6 is to combat HIV/AIDS, malaria and other diseases. For this, one of the targets is to have halted by 2015 and begun to reverse the spread of HIV/AIDS. The second target is to have halted by 2015 and begun to reverse the incidence of malaria and other major diseases. Goal 7 is to ensure environmental sustainability. The health-related targets are to halve by 2015, the proportion of people without sustainable access to safe drinking water and improved sanitation. And lastly, Goal 8 is the development of Global Partnership for Development. A health-related target is to provide access to affordable essential drugs in developing countries, in cooperation with pharmaceutical companies. Cost of Achieving the Health MDGs
Essential health interventions cost money, though surprisingly not as much as one might expect. Through a variety of methodological approaches, the Commission on Macroeconomics and Health estimates that an essential set of interventions to reduce avoidable deaths in low-income countries would require outlays of around $30 -$40 per person per year, including the costs of fighting the AIDS pandemic. The specific financing needs will of course vary across countries and regions, depending on the disease epidemiology (e.g. the incidence and prevalence of malaria, HIV/AIDS, and TB) and local economic conditions. Most of the $30 - $40 will have to come through public outlays, for two reasons: to cover public goods (like infectious disease control), where individuals lack the incentive on their own to take the necessary protective actions; and to ensure access for the poor, who lack adequate household funding (WHO, 2001). The Commission further stresses that their estimate is a lower bound. Not a lot of quality health services can be purchased at $30-$40 per person, certainly not the kind of comprehensive care found in the high-income countries, where outlays are around $1,900 per year. The Commission’s estimates refer to a rather minimal health system, one that can attend to the major communicable diseases, maternal and perinatal conditions, and micronutrient deficiencies that account for a significant proportion of the avoidable deaths in the low-income countries. The Commission’s costing estimates do not include some key categories that will need to be part of any operational health system, such as: trauma and emergency care (broken bones, appendectomies); tertiary hospitals; and family planning (including distribution of contraceptives). The Commission therefore regards its estimates as lower bounds of total health care costs, but an accurate assessment of what is needed for a decisive drop in avoidable deaths due to the disease conditions on which it focussed. The costs will mainly be incurred on: health systems (scaling up of system-wide human resources and infrastructure, and also on interventions designed to improve system quality); child health; maternal and reproductive health; HIV/AIDS; malaria; tuberculosis; and access to essential medicines. MDG Financing in Uganda
Uganda spends about USD 20 per capita on health, of which about USD 3.5 is government public expenditure and the balance is donor aid (USD 4) and private expenditure (USD 12.5) (Draft NHA Report 98/99 to 2000/01). The cost of delivering a minimum health care package in Uganda has been estimated at approximately USD 28 per capita -this would best be accomplished by funding through the public system, as the private sector does not necessarily prioritise the health services articulated in the minimum package which are in alignment with the MDGs. The cost is less than what has been indicated by the Commission for Macro-economics and Health mainly because the Uganda estimate did not include provision of free anti-retrovirals to all those infected with HIV/AIDS. Therefore a glaring funding gap exists. The Minister of Finance's 2003/04 budget figures put the health sector's share of the Government of Uganda's budget at 9.6%i. It is a considerable increase from earlier years as is shown in the figure below, but still is inadequate. It is also still far below the recommended 12 – 15% of national GNP expenditure. (Figure) Source: Ministry of Finance Planning and Economic Development. Poverty Eradication action Plan 2001-2003, Vol. 1. Ministry of Health. Health Financing Strategy Paper for Uganda. Draft March 2002. National Health Accounts 2002. Ministry of Finance Planning and Economic Development, Budget Speech 2003/04, June 2003. The problem of inadequate funding of the sector has further been aggravated by inefficient allocation of available resources within the sector. Internal resources for health Ugandans should certainly improve health-sector
management, and should raise domestic resources for health within their limited means. In Uganda, the principal health The costs will mainly be incurred on: health systems (scaling up of system-wide human resources and infrastructure, and also on interventions designed to improve system quality); child health; maternal and reproductive health; HIV/AIDS; malaria; tuberculosis; and access to essential medicines. Tax-based financing: Health services are paid for out of general government revenue such as income tax, value added tax, import duties etc. User fees: Patients pay directly, according to a set tariff, for the health care services that they use. This is the most common way of paying for privately provided health services in Uganda, but is also used as a component of financing for public sector services. Private insurance: Membership of the private insurance schemes is voluntary, the insurance fund is held by a private (frequently for profit) company. Community-based health insurance: Again membership is voluntary, but the insurance fund is held by a private not for profit entity. The very poor are unable to make any significant financial contribution for health services; so government must secure health care financing for them. Further, government must play an important role in protecting the poor, not only through financing health care services, but also through providing regulatory and policy frameworks for the various forms of financing. Tax-based financing is the predominant form of health care financing in Uganda simply because it is pro-poor. This system is to some extent progressive irrespective of the small formal sector, and protects the poor from financial shocks associated with large health care costs. The main concern is however the low level of funding available from this source. It is mainly constrained by the limited tax bases in Uganda. Further, a relatively small share of the total government budget is allocated to health care. Strengthening planning, budgeting and monitoring systems so the Ministry of Health can better demonstrate how funds are effectively used may help to increase government allocations to health. Private insurance is generally confined to a relatively elite and politicised group. As such, it does not form a substantial form of financing for the health sector. User fees have been tremendously unpopular with the poor in Uganda as evidenced by decreases in service utilisation. Low household incomes means that the revenue generating potential of user fees is low. Community-based health insurance schemes have continued to emerge in Uganda with the aim of attempting to mitigate some of the worst equity effects of user fees by spreading contributions between the healthy and the sick and allowing people to spread their contributions over time in a predictable manner, rather than paying when they fall sick. These schemes are mostly covering those outside of formal sector employmentii. External resources for health
Given the limited capacity of low-income countries to mobilize government revenues, and the considerable demands on those revenues for public administration, infrastructure, agriculture, police, defence, education, and debt servicing in addition to health, it is probably optimistic to expect that low-income countries could muster even 4 percent of GNP for health. In short, domestic resource mobilization will not begin to close the financing gap between current spending and totals needed to coverage essential health services (WHO, 2001). The Report of the Commission on Macroeconomics and Health found an irreducible gap between financial means and financial needs for low-income countries, which the donor world will have to fill for success in meeting the MDGs. For Uganda, with a per capita GNP of around USD 300, the country cannot be expected to adequately finance the health sector and so that is why Uganda must look to sustained donor grant financing to meet the needs of universal access to essential life saving interventions. Only donor assistance can close that financing gap Uganda i.e. in order to close the gap between the costs of essential services and the available resources. However the complexity of all this assistance is that the various donors impose widely differing standards for accessing funds, and both subtle and overt political agendas. Recent work at the Ministry of Health has shown that up to 70% of donor funding in the country may not be targeting the key inputs for the minimum package of services as laid out in the Health Sector Strategic Plan and the Health Financing Strategy. The recent trend to increase donor funding through the budget has shown that without an overall marked increase in funding from the donors, channelling of funds through the government budget can lead to an increase in health outputs. Uganda’s efforts on MDGs & the PEAP
As part of the overall development strategies, the Monterrey Consensus emphasises the importance of nationally owned strategies for reducing poverty. Since the late 90’s a number of developing countries including Uganda have been preparing Poverty Reduction Strategy Papers (PRSPs), which provide a framework for financing, implementing and monitoring such strategies. PRSPs emerge from participatory processes involving government, civil society and external partners, including the World Bank and International Monetary Fund (IMF). Though far from perfect, PRSPs move poverty reduction closer to the centre of development strategies. They also provide a framework for donor coordination based on national priorities (UN, 2003). The Poverty Eradication Action Plan (PEAP) is Uganda's national development framework and medium term planning tool, prepared in 1997 through wide stakeholder consultations and participation. The PEAP, which is also the Country's Poverty Reduction Strategy Paper (PRSP), guides the formulation of government policy and implementation of programmes through sector wide approaches and a decentralized governance system. The expenditure implications of the PEAP are translated into concrete spending decisions through the Medium Term Expenditure Framework (MTEF) and annual budgets. The PEAP 2001 that was revised last year (2003) is structured around four overarching pillars: fast and sustainable economic growth and structural transformation; good governance and security; increased ability of the poor to raise their incomes; and increased quality of life of the poor. There is a substantial overlap between the PEAP targets and MDG Goals. Like the MDGs, the PEAP also has broad national goals for poverty eradication, UPE, gender, child and maternal mortality, HIV/AIDS (but not malaria), environmental sustainability and partnership principles. Both also share the same overall objective of holding Government and development partners accountable for development progress (MFPED 2003). The crucial difference lies in the quantitative targets that each of them embody. The PEAP targets relating to poverty, UPE, HIV/AIDS and water are more ambitious than the MDG targets. On the other hand, the MDG targets for gender equality in education, infant mortality and maternal mortality are more ambitious than those set out in the PEAP (MFPED 2003). There are several good arguments for letting the national PEAP targets predominate. First of all, it was never felt that the intention that the MDGs should superimpose its quantitative targets on the national level, rather these should be seen as global targets. The purpose of the MDGs was to induce developing countries to set their own national targets through a process of consultation. Further in comparison with the MDG targets, the PEAP targets are typically more realistic and relevant. Despite the predominance of PEAP targets, the MDGs can play several useful and important roles. First, the MDG targets have already been fully embraced by certain sectors, such as education. Secondly, they can be used to enrich the existing list of poverty monitoring indicators, notably in relation to MDG goal 6 (HIV/AIDS, malaria and tuberculosis). Finally, the MDGs are useful for international comparisons so that Uganda can measure its own performance against that of similar countries using the same yardstick. Child Mortality
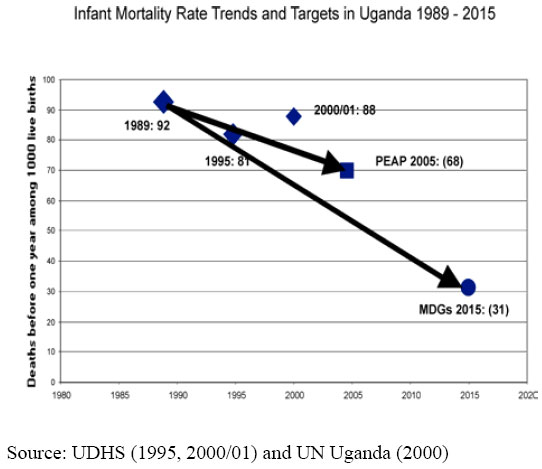
Child mortality is an important indicator of the successful implementation of the PEAP. This is so because the level of child mortality is affected by a broad range of government interventions, such as access to education, safe water, basic health care and provision of security and stability. Despite high economic growth and poverty reduction, infant (under1) mortality has stagnated over the last decade; in fact, there has been almost no progress since 1970. With 88 infant deaths per 1,000 live births in 2001, government missed the PEAP target of 78 deaths per 1,000 live births by 2002. The new PEAP target of 68 deaths per 1,000 live births by 2005 is ambitious, but can potentially be attained if serious policy action is taken. The MDG target of 31 deaths per 1,000 live births by 2015 is even more ambitious than the national target, and appears very ambitious in light of past trends (MFPED, 2003). (Figure) Some of the reasons why infant mortality has not improved include a high fertility rateiii, low birth spacingiv, a high proportion of socially and economically vulnerable women (widowed, separated and divorced), a high number of unsupervised deliveries; a deterioration in levels of immunised children; uneven economic growth and insecurity in some parts of the country (MFPED, 2003). Maternal health
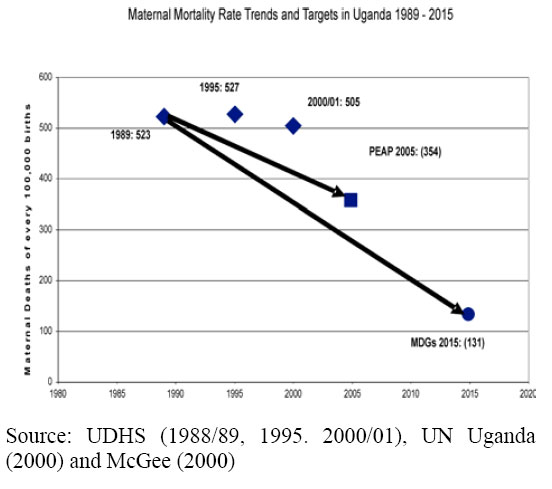
There have been virtually no improvements in maternal health in Uganda over the last decade. Between 1989 and 2001, maternal mortality fell only slightly from 523 to 505 deaths per 100,000 live births. Government therefore missed its target of 354 per 100,000 live births by 2000. This target has subsequently been postponed to 2005. The MDG target is substantially more ambitious than the government target at 131 deaths per 100,000 live births by 2015. Uganda has been listed as one of eighth countries with the biggest maternal mortality rate in the world (MFPED, 2003). Some of the most important direct causes of maternal mortality in Uganda are bleeding, infection, abortion, hypertension and obstructed labour. The predisposing factors are: poor maternal nutrition, short birth intervals, early age at first birth, and lack of trained assistance at birth. (Figure) Malaria and other diseases
Malaria is a major public health concern in Uganda, and is the leading cause of morbidity and mortality. This disease particularly affects under-5s and pregnant women. There is some evidence that morbidity associated with malaria has increased since 1994. The proportional morbidity for adults and children associated with malaria increased from 25% in 1995 to 37% in 2000 (MoH 2001). Anecdotal and participatory evidence also point to an increased frequency and severity of malaria episodes (MFPED 2000). The 2000/01 UDHS estimates that only 13 percent of all Ugandan households have a mosquito net and that only 8% of children under five usually sleep under one. Around a third of all Ugandan women take drugs against malaria during pregnancy. An important reason for the increase in the frequency of malaria is increased drug resistance to chloroquine, and consequently the Ministry of Health has now changed the first line of treatment to Fansidar and Chloroquine. Government has also abolished taxes and tariffs on mosquito bed nets in an effort to make malaria protection more affordable to the people and also government has introduced home-based management of fever, which provides free, pre-packaged malaria treatment for children through community distributors only. HIV/AIDS
Committed and sustained political leadership, early intervention, a strong focus on prevention and a multisctoral approach has led to the reduction in HIV prevalence from around 20% in 1991 to 6.5% in 2001 (MoH 2002). The international target is to halt by 2015 and begin to reverse the spread of HIV/AIDS. Uganda achieved this target in 1996. Past progress in reducing HIV/AIDS prevalence is to some extent reversible, as the recent increase in prevalence from 6.1 to 6.5% suggests. Government will continue its current information, education, and communication campaign, promoting condom use, scaling up of PMTCT and voluntary counselllling and testing facilities to prevent mother-to-child transmission. Finally, government is finalising plans to make ARVs freely available to the people. Safe water and sanitation
Over the past decade, government has made substantial progress in terms of increasing access to safe drinking water. Rural coverage increased from 24% in 1991/92 to 55% in 2001/02, while urban coverage increased from 60 to 62% between 2000 and 2001. Performance in the rural sub-sector has been in line with the PEAP target of 65% coverage by 2005 and full coverage by 2015 with an effective use and functionality rate of 80 to 90% (MFPED, 2003). However, sanitation and the associated environmental household behaviour is very poor in the country with detrimental consequences for health and productivity. According to UNHS (1999/00), 83% of the Ugandan population use a pit latrine and 2% a flush toilet, while 14% do not have access to any toilet facility. The 2001 Poverty Status Report however observes that many of the pit latrines may be extremely rudimentary and cites only 51%v of the rural households can be said to have access to safe excreta disposal. The reasons for this poor sanitation have been a general lack of interest and demand for household sanitation (MFPED 2002). Secondly, ensuring access to sanitation has also not received the same priority attention as has safe water provision, this despite the fact that the interventions are interdependent. Lastly, coordinated government intervention is further hampered by the fact that the institutional responsibility is spread over three different sectors, namely health, education and water, and until recently, the roles of each institution remained unclear and interesectoal collaboration basically non-existent. This nonexistent collaboration also hampered performance monitoring due to the existence of conflicting targets in various sector plansvi (MFPED, 2003). Access to Essential Medicines
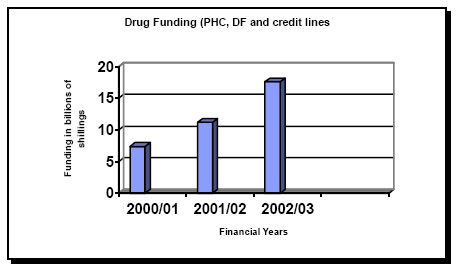
The last 2 years have shown an increased drug funding and improvements in drug management. Drug funding has increased from Ug. Shs. 7.4 billion in 2000/01 to 11.2 billion in 2001/02 and 17.6 billion in 2002/03 as is shown in the figure below. (Figure) Drug procurement by the districts (including the use of drug credit lines) has also been instituted to improve on drug management. The sustained high OPD utilisation seems to agree with this. However, there is still need for improvement considering the ever increasing OPD attendances and the high population growth. The pressure on the drug resources is going to be from the introduction of antiretrovirals and the new vaccines. What are the chances of Uganda achieving the MDGs?
The feasibility of meeting the MDGs in the low-income countries is a universal debate with wide ranging views. On one side of the debate are those who believe that the health goals will take care of themselves, as a fairly automatic by-product of economic growth. With the mortality rates of children below 5 years in the least-developed countries standing at 159 per 1,000 births, compared with 6 per 1,000 births in the high-income countries. They take the view that it's just a matter of time before the mortality rates in the low-income world will converge with those of the rich countries. This is unlikely to happen for two reasons. First, the disease burden itself will slow the economic growth that is presumed to solve the health problems; second, economic growth is indeed important, but is very far from enough. Health indicators vary widely for the same income level. The evidence suggests that 73 countries are far behind in meeting the MDGs for infant mortality and 66 are far behind for meeting the MDGs for child mortality. The other side therefore argues that the poverty and/or disease burden can and should be brought down in line with the MDGs by a concerted, global strategy of increasing the access of the world's poor to essential health services. Meeting these goals is feasible but far from assured. Success in achieving the MDGs will require a seriousness of purpose, a political resolve in countries, and an adequate flow of resources from high-income to low-income countries on a sustained and well-targeted basis, and the efficient, equitable and transparent management of these resources in the recipient countries (WHO, 2001). Responsibility for achieving these goals is at four levels. At global level are the multilaterals, bilaterals and multinationals whose role would be the coordination of the economic and health systems, and also the mobilisation of funds. The leadership of the multilaterals at this level is particularly important. Although the UN agencies and the World Bank/IMF have all signed up to the MDGs, the latter organisations do not seem supportive as shown by their support of decreasing public spending in developing countries. The MDGs cannot be achieved without substantial increases in public spending for social services in developing countries. At the national level responsibility, lies with heads of governments and the Ministries of Finance as they determine the macroeconomic policies including the rate at which public budgets can grow, including the allocation between sectors. The heads of governments and other arms of government (executive, legislative and judicial) also play a big role in determining the wider political and governance environment. This has been well appreciated in the Ugandan PEAP. The ongoing insecurity in Northern Uganda has continued to have a negative social and economic impact on the development indices. The recent stagnation of public expenditure as seen in the draft Long Term Expenditure Framework (LTEF) and the draft 2004/05 MTEF is likely to deliver neither the PEAP nor the MDGs. At sector level the Ministry of Health and other health stakeholders have the responsibility to allocate available resources efficiently and equitably, and supervise health services delivery at all the levels of the health system. Lastly the operational level, the local government leaders, health workers and the community are responsible for improvements in health services and health. The pursuance of PEAP and MDG goals inevitably exerts an increased pressure for public spending on social sectors, such as health, education and water and sanitation. A substantial number of interventions are necessary if we are to meet all the poverty goals. Full implementation of the PEAP would require an additional 63% of current government spending, while attaining the MDGs would be far more expensive. Currently the social sectors are heavily under funded. Uganda’s continuing economic development requires a further intensification of investments in human capital – the health and education of its people. With these investments, Uganda can fulfil its potential as one of the world’s great success stories in economic development. Without these investments, however, Uganda will flounder, with slowing economic growth, insufficient foreign investment inflows, and unnecessary human suffering. The Uganda budget should make ample room for all donor-financed grants for health that Uganda can attract. Artificial ceilings on health expenditure, in the name of macroeconomic stability are a false economy. There is no true stability without health, and the Ugandan economy can usefully absorb massive increases in foreign grants for health – indeed, and also, much greater amounts than the donors are likely to make available (Sachs JD, 2002). Growth in health expenditure is essential if Uganda is to meet its poverty eradication goals. Although high mortality is a health outcome, it is not solely the responsibility of the health sector and activities geared towards reduced mortality are essentially multi-sectoral. Further, high mortality is not due to lack of appropriate policies in Uganda, but rather due to inadequate policy implementation. Mortality reduction is likely to require substantial resource investments in the social sectors. The single most important activity is probably expanding access to obstetric emergency health care facilities, which also happens to be one of the most expensive interventions. References
End Notes i The health sector’s share of the GoU budget is about 9.6%, still unfavourably low compared with other similarly progressive countries
(Zambia 13.3%, Ghana 13%, Mozambique 12%).
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}