 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 2, No. 1, April, 2004, pp.40-47 FINANCING THE MILLENNIUM DEVELOPMENT GOALS: IS MORE PUBLIC SPENDING THE BEST WAY TO MEET POVERTY REDUCTION TARGETS?i Martin Brownbridge, Macroeconomic Advisor, Ministry of Finance, Planning and Economic Development, Uganda Code Number: hp04011 Abstract
Copyright 2004 - Department of Health Sciences of Uganda Martyrs University
The strategy for expanding public services through donor funding is flawed and is doomed to fail. Donor funding necessitates increased internal public expenditure. This shifts resources away from the export-oriented private sector, which would bring about economic growth and provide a basis for a more comprehensive poverty reduction. There are also absorptive limitations in the use of large donor aid. Donor funds distort Government’s budget allocation pattern, cohesion and stability. The funding gap envisaged under MDGs by donor aid advocates ranges between 6.4% to13.6% of Uganda’s GDP, which are enormous. Large donor aid will lead to contraction of the private sector, appreciation of the shilling and falling prices of agricultural produce. It would mean that the Government would have to depend on donors for over 60% of its budget. And yet donor funding is volatile and unpredictable. The strategy of achieving MDGs through large donor aid should be abandoned. Instead, as projected in the long-term expenditure framework, Uganda should concentrate on the current budget policy to increase economic growth. In 10 years, revenue will have increased by 150% and health expenditure will be about 15% of the Government expenditure. Introduction
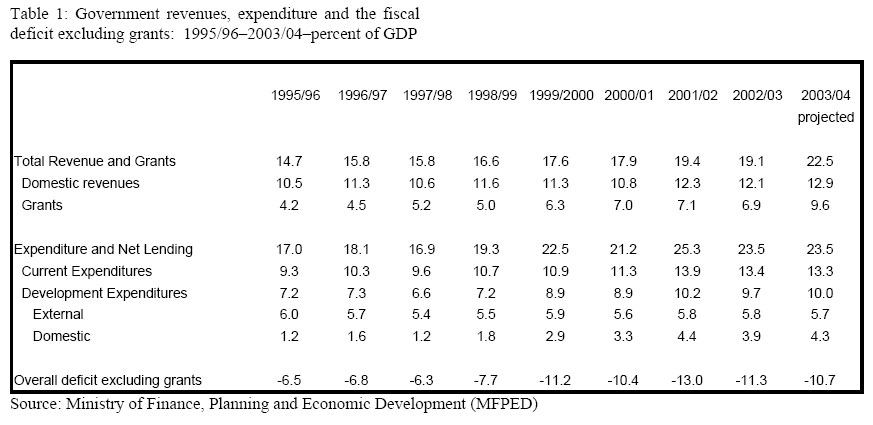
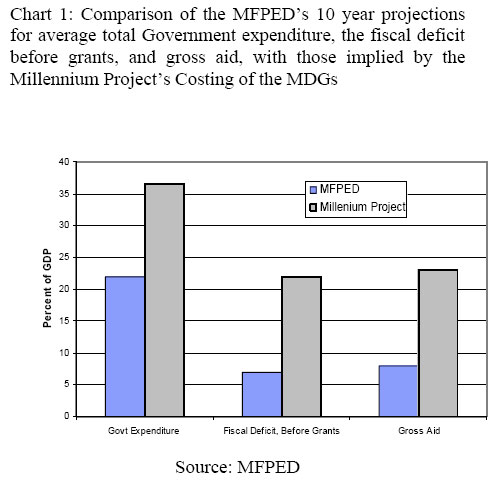
The development agenda currently being articulated by some of the international and donor agencies to achieve the Millennium Development Goals (MDGs) entails a substantial expansion of public expenditure on basic social services, such as education and health, financed by increased donor aid (UNDP, 2003). For example, the Commission on Macroeconomics and Health advocates increases in donor funding for health expenditures in Least Developed Countries which would amount to an average of 7% of the GDP of these economies (Commission on Macroeconomics and Health, 2001). This approach to tackling poverty in the developing world has motivated the setting up of global funds such as the Global Fund for AIDS, Tuberculosis and Malaria (GFATM), and the Education for All Fast Track Initiative (EFA-FTA), which aim to mobilise resources from donors to finance a scaling up of social service provision in the health and education sectors respectively. This paper argues that the MDG approach to development, based on a large donor funded expansion of public services is flawed, and risks failure. The main reason why the approach is flawed is that it fails to recognise that there are unavoidable trade offs between achieving the various MDGs, which more donor aid alone cannot resolve because the bulk of the resources required to tackle poverty must be generated from within the domestic economy. Public expenditure competes with the private sector for scarce resources. In the long run, the economic growth which is essential for reducing both income poverty and for improving the health status of the population, depends on a dynamic export-oriented private sector, but the growth of this sector will be stifled if the public sector commands too large a share of the economy’s resources. There are also absorptive constraints within the different sectors that would stand to receive additional funding under the MDG approach which would impede the effectiveness with which additional spending is translated into an expansion of public services for the population, but that is not the main argument of this paper. Even if the different sectors individually could usefully absorb much more resources, a constraint would still operate at the level of the macroeconomy because, to achieve an expansion of each of the sectors together (i.e. an expansion of health, education, water, roads, etc) would require a huge transfer of real resources into the public sector from the rest of the economy. This would be detrimental to private sector led growth. It would also drive up unit costs in the public sector, with the result that the real increase in the provision of public services would be much less than the nominal increase in public spending. The second drawback with the approach advocated by the international organisations, most notably with the global funds, relates to the adverse impact which this would have on budget policy planning and management in Uganda. The global funds essentially involve Uganda’s budget being determined outside of the country’s normal budgetary process, on the basis of how much additional resources could be mobilised from donors to finance the specific categories of expenditures eligible to receive financing from these funds. This would distort both inter-sectoral and intra-sectoral budget allocations, and would undermine many of the important budget reforms, such as the introduction of the Medium Term Expenditure Framework (MTEF) and the sector working groups, that Uganda has implemented since the mid 1990s to improve budget planning and management. As such, they will force budget allocations away from what would be considered optimal by the Ugandan Government and damage the efficiency of public expenditure. Finally, there would also be serious dangers, both to the sustainability of public finances and to macroeconomic stability, if Uganda became even more heavily dependent upon donor aid, which is a source of budget funding outside Government’s control. This paper is organised as follows. Section 2 outlines recent fiscal trends in Uganda and reviews estimates of the additional public spending required to achieve the MDGs. Section 3 evaluates whether increased public spending is compatible with rapid economic growth. In section 4, the consequences of the MDG approach for the vulnerability and sustainability of public finances is discussed. Section 5 assesses the compatibility of global funds and other "earmarked" donor aid inflows, and the proposal for setting up a National Commission on Macroeconomics and Health with the budgetary reforms which Uganda is implementing. Section 6 concludes the paper with the policy implications for long term budget policy in Uganda. Recent fiscal trends and implications of the MDGs for public spending Table 1 below gives details of the main Central Government fiscal aggregates, as percentages of GDP, from the mid 1990s to the current fiscal year. Three points are pertinent for this paper. First, there was a large increase in total Government expenditure between 1997/98 and 2001/02, amounting to 8.4 percentage points of GDP. In real terms (i.e. adjusted for inflation in the cost of public services), this amounted to a 42% increase in this period. Second, domestic revenues (taxes and non tax domestic revenues) increased only slowly in this period, by less than two percentage points of GDP. Consequently the fiscal deficit before grants (domestic revenues minus total expenditures and net lending) doubled from 6.3% of GDP in 1997/98 to 13% of GDP in 2001/02. Third, because of concerns over the sustainability of the large fiscal deficit, Government began to implement a medium term programme of fiscal consolidation in 2002/03, designed to scale back the fiscal deficit by restricting the growth of expenditures to a slower rate than that of recurrent revenues. As a result the fiscal deficit before grants has been reduced to a projected 10.7% of GDP in the current fiscal year. Over the next 10 years, the Ministry of Finance, Planning and Economic Development (MFPED) envisages holding total Government expenditure roughly constant as a percentage of GDP while raising domestic revenues to gradually reduce the fiscal deficit before grants. The reasons for this fiscal consolidation are to free up resources in the banking system for the private sector and shift price incentives in favour of exporters in order to stimulate economic growth, and to reduce the excessive dependency of the Government budget on donor aid. This is to ensure that the financing of the budget becomes more sustainable over the long term. The approach to financing the MDGs advocated by some of the international organisations is fundamentally different from that of the MFPED, and implies much higher levels of public spending and the fiscal deficit, before grants, over the next 10 years. It essentially involves estimating the inputs necessary to meet MDG related targets in each individual sector, such as the number of teachers required, costing these inputs, and then calculating the financing gap which must be funded by the donors if the target is to be achieved. The funding gap in each sector is then added together to derive an estimate of the total requirement for additional aid. Estimates of the budgetary cost derived from this approach vary considerably, but all involve a substantial expansion in the size of the Government budget and in the fiscal deficit. EPRC (2002) estimate the annual budgetary cost of meeting Chart 1: Comparison of the MFPED’s 10 year projections MDG related targets in three sectors – education, health and for average total Government expenditure, the fiscal deficit water – based on cost estimates in the respective sector before grants, and gross aid, with those implied by the investment plans and demographic projections up to 2015. Millennium Project’s Costing of the MDGs EPRC estimates a funding gap equivalent to 6.4% of GDP in 2003 which declines to 4.8% of GDP in 2015.ii The funding gap of the health sector, including HIV/AIDS, is estimated at 3.9% of GDP in 2003. The Millennium Project (2003) attempts to identify and cost a set of interventions which it considers necessary to meet the MDGs over the 11 year period 2005-2015.iii The Percent of GDP results, which are preliminary, would entail MDG related Government expenditures equivalent to an average of 24.3% of GDP over this period, funded from both domestic and external resources. Of the total MDG related public expenditures, health expenditures account for 37% (9.1% of GDP).iv It is assumed that domestically financed non-MDG related and non-defence Government expenditures remain roughly constant at 10.7% of GDP. Therefore, total Government expenditures would have to rise to around 37% of GDP,v an increase of around 13.5 percentage points of GDP over the current fiscal year’s level of Government expenditure. The Millennium Project estimates an external financing gap (i.e. the amount of donor aid required) equivalent to 16.6% of GDP over the period. This is likely to be an underestimate, as it appears to be based on an assumption that Uganda could generate domestic revenues of over 20% of GDP in this period. In reality domestic revenues are likely to average about 15% of GDP in this period, hence net aid inflows equivalent to 23% of GDP would be needed to fund the level of Government expenditures envisaged by the Millennium Project. This is double the current level of aid inflows.vi The Commission on Macroeconomics and Health (2001) sets a target for health spending of $34 per person per year, which in Uganda translates into aggregate health spending of approximately Shs 1,770 billion at current prices, equivalent to 13.6% of GDP. In 2002/03, Uganda spent Shs 700 billion on health in the public and private sectors, equivalent to 5.9% of GDP.vii Hence Uganda would need to raise expenditures on health by about 7.6% of GDP to meet the WHO’s target for health spending. If instead the target of $34 per capita were to be met after 10 years of 3% real per capita GDP growth, Uganda would still need to raise health spending by 5.7% of GDP. To contrast the fiscal implications of the approach of the international organisations to funding the MDGs with that of the MFPED, chart 1 below depicts the average level of Government spending and the fiscal deficit before grants in the MFPED’s Long Term Expenditure Framework (LTEF) with that implied by the funding projections made by the Millennium Project, over the next 10 years. Compared to MFPED’s LTEF projections, the Millennium Project implies higher total Government expenditure by about 15% of GDP, while both the fiscal deficit before grants and gross aid would be approximately three times higher than the LTEF projections. Income growth and health status
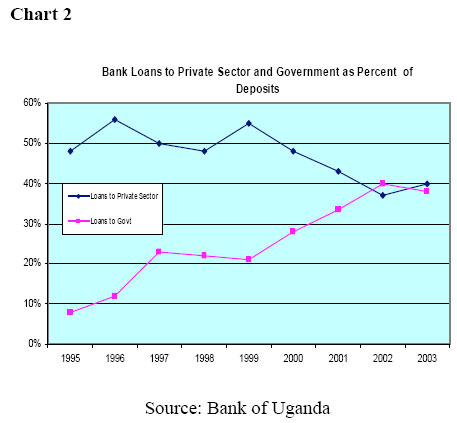
The key strategic question for public policy in Uganda is whether a large increase in donor funded public expenditure is the optimal, or even a feasible, strategy for achieving poverty related objectives. The answer to the question revolves around the impact which higher public spending, and a higher fiscal deficit, would have on the economy’s long term prospects for economic growth, because economic growth is central to both achieving income poverty targets and also achieving other targets such as improving the health status of the population. Improving the health of the population is an important policy objective, but achieving this objective depends much more on generating sustained growth in real incomes than in expanding public health services. Cross country econometric analysis by Filmer and Pritchett (1997) found that 95% of the cross country variation in child mortality is explained by socio economic variables such as per capita income, income inequality and female educational attainment, with per capita income alone explaining 84% of the variation in child mortality. In contrast, public spending on health had a negligible impact -differences in public spending on health accounted for only 0.15% of the cross country differences in child mortality. While improved health can contribute to income growth and, therefore, higher per capita incomes, by enhancing the productivity of the workforce, the econometric evidence indicates that the net direction of causality runs from income to health status rather than from health status to income (Jack, 1999). This does not imply that well targeted and efficient public spending on health services cannot make a significant impact on the health status of Uganda’s population, but it does mean that sustained per capita GDP growth is a prerequisite for major improvements in the health status of the Chart 2 Ugandan population. It also means that the more equitably distributed is GDP growth, the larger the positive impact that this will have on the population’s health status. Consequently, economic and budgetary policy has to prioritise the acceleration of real broad based GDP growth in Uganda. Expanding public expenditure would have a profound impact on the spending and production structure of the economy. First, demand for non traded goods would increase, because the vast majority of public expenditures consist of non traded goods. As non traded goods can only be produced domestically, the structure of production within the economy would have to shift towards non traded goods and away from traded goods.viii This shift would be brought about by an appreciation of the real effective exchange rate (REER). Hence a contraction of the traded goods sectors would be required to free up the domestic resources required to support an expansion of non traded goods production. Second, because of the expansion of public non traded goods expenditure, there would be an increase in the share of domestic production which supplies public goods and servicesix at the expense of production which supplies competitive markets in both Uganda and especially export markets. Third, the increase in the fiscal deficit before grants would have monetary consequences, because Government expenditures, except for the small share which consists of imports, creates domestic liquidity (base money) which must be sterilised by the Bank of Uganda (BOU) if it is to retain control over the money supply. Sterilisation involves the sale of foreign exchange and Government securities (Treasury Bills –TBs-). Both the foreign exchange market and the domestic financial market in Uganda are very shallow which limits the extent to which they can absorb large sales of foreign exchange or TBs, without destabilising volatility in exchange rates, interest rates and private sector credit. Because of the large increase in the fiscal deficit between 1997/98 and 2001/02, the BOU had to increase TB issues tenfold, which crowded out private sector borrowing from the banking system. Conversely, in 2002/03, the cut in the fiscal deficit allowed for a smaller increase in TB issues, which created room in the banking system for a rebound in private sector credit. Chart 2 shows bank lending to the private sector and bank lending to Government (mainly in the form of TBs) both as a share of bank deposits. Bank lending to Government took an increasing share of bank resources, especially between June 1999 and June 2002, because of the rise in the fiscal deficit, at the expense of bank lending to the private sector which fell as a share of bank deposits. These trends were only reversed in 2002/03 when the fiscal deficit was cut. What impact would higher public spending have on the economy’s long run rate of growth? Economic growth depends on the growth of factors of production – capital and labour – and in total factor productivity - the efficiency with which factors of production are used. Increased Government spending could improve the quality of the labour force – through better education and health - and could also add to public capital, such as infrastructure, both of which have positive effects on the economy’s growth potential. However, these positive effects on growth will be limited by absorptive constraints in the public sector and in the wider economy. For example, although there was a very steep increase in public expenditures on fixed capital investment between 1997/98 and 2002/03, most of the increase was absorbed by higher unit costs of construction, with very little change in real investment expenditure. There are also serious concerns about the poor quality of public construction expenditures, such as classrooms built with the School Facilities Grant. Further expansion of public expenditure would exacerbate these absorptive constraints with the result that the contribution made by additional public spending to economic growth will be at best very limited. Any positive effects of higher public spending on growth are likely to be outweighed by the significant negative impacts, because of the effects which this will have on the private sector, on price incentives and on the structure of production, though several channels. First, it is likely that real private sector investment will decline for two reasons: because of the crowding out effect of higher fiscal deficits on the private sector’s access to bank credit and because higher levels of public construction investment will drive up investment costs for the private sector. In general, private investment has stronger effects on growth than public investment, hence unless there is a large increase in total investment, a shift in the relative shares of investment, from the private to the public sector, will depress the economy’s growth rate. Second, the shifts in the structure of production, with a larger share of production supplying public goods and services as opposed to goods and services for the market, and a larger share of production consisting of non traded goods as opposed to traded goods, will negatively affect the growth in the efficiency of resource use in the economy, which in turn will depress the economy’s growth rate. This is because competitive markets, and especially export markets, create pressures which force firms which sell on these markets to continuously improve efficiency in order to compete and survive. The public sector does not face similar pressures to continuously improve efficiency, because it does not have to sell its output in the market.x In the long run, it is the growth in the efficiency of factor use which will make the greatest contribution to increases in per capita real incomes in Uganda. Therefore if the market pressures on domestic producers which drive increases in total factor productivity are reduced, because a larger share of output is produced by, or sold to, Government, total factor productivity will fall. In addition, export sectors are especially important for driving rapid economic growth because export markets are very competitive and because they offer opportunities for realising economies of scale and specialisation of production which cannot be realised in small domestic markets. Consequently a shift in the price incentives against export production, because of the appreciation of the real exchange rate, will further depress economic growth. Moreover, because Uganda’s comparative advantage lies in agriculture and because this is the sector where the majority of the poor earn their living, an appreciation of the real exchange rate induced by higher public spending will be regressive for income distribution.xi Real exchange rate appreciation will reduce the real farm gate prices which cash crop farmers, such as coffee farmers, receive for their produce. Also, a real appreciation of the exchange rate will make imported food, which competes with domestically produced food, cheaper, thereby driving down the farm gate prices received by food crop farmers, which will reduce their incomes. Dependence on donor aid and vulnerability of the budget and the economy
The MDG approach would increase the vulnerability of the Government budget and the wider economy, because it would worsen the dependence of the budget on donor aid. Fiscal vulnerability is defined as a situation where the fiscal position may be sustainable in the current circumstances, but would become unsustainable in the event of some sort of exogenous shock to revenues or expenditures (Ize, 1991: 67). The budget is already heavily dependent on donor aid, which is one of the reasons why Government is scaling back the fiscal deficit over the medium term. In the current fiscal year, domestic revenues – taxes and non tax revenues – will be sufficient to fund only 52% of Government expenditure and external debt repayments, with gross inflows of aid funding almost all of the remaining 48%. If Government expenditure is to be increased to the levels envisaged by the Millennium Project, Government would be dependent on donor aid to fund over 60% of its expenditures. Donor aid is both volatile and unpredictable. Bulir and Hamann (2003) examined the volatility of aid flows in a sample of 72 developing countries, and found that aid was more volatile than fiscal revenues (expressed as a percentage of GDP), especially in aid dependent countries. They also found a systematic tendency for aid commitments from aid donors to exceed aid disbursements. In countries with IMF programmes, disbursements of programme aid (e.g. budget support) were on average 25% less than projected, even when there were no interruptions to their IMF programmes (i.e. their IMF programmes were "on track"). Greater dependence on donor aid would entail severe disruption for the budget in the event of a cutback in aid disbursements, relative to commitments. Although purely temporary shortfalls in aid can be accommodated through running down the BOU’s foreign exchange reserves, any shortfalls which are not purely temporary would necessitate budget cutbacks. Because large areas of the budget, such as the wage bill and statutory expenditures, cannot be reduced in the short term, budget cutbacks fall disproportionately on a relatively small share of the non wage budget, which is very disruptive for the delivery of public services. It is not prudent budget management for the Government budget to be excessively dependent on budgetary resources which are volatile and over which Government has no direct control. In addition, increased aid dependence would also have consequences for the wider economy in the event that aid disbursements fall short of commitments. An aid funded expansion of public services would entail large sales of foreign exchange by the BOU to the private sector, as the counterpart to Government expenditures in domestic currency. Hence if there were serious shortfalls in aid disbursements, other than purely temporary shortfalls, the BOU would have to cut back its sales of foreign exchange to protect its reserves. This would trigger an exchange rate depreciation and possibly capital flight, leading to a balance of payments crises, which would be very damaging for the wider economy. Budget Policy Formulation
Since the mid 1990s, Uganda has implemented major budget reforms, including the introduction of the MTEF, the establishment of Sector Working Groups and preparation of sector investment plans. These reforms are intended to strengthen national ownership of the budget, ensure that the medium term inter and intra sectoral allocation of the budget accords with Government’s own strategic priorities, and improve the efficiency of Government expenditure. However, the budget reforms will be undermined by two elements of the approach to funding the MDGs advocated by some of the international organisations: the concept of additionality of spending attached to the use of global funds, and the recommendation for setting up a National Commission on Macroeconomics and Health to determine the health sector’s budget. The basic principles on which the Government budget is formulated are as follows. First, the MFPED determines the overall size of the Government budget on the basis of the projected budgetary resource envelope and macroeconomic objectives. Second, the MFPED allocates expenditure ceilings to each of the sectors in accord with agreed priorities (which include commitments given to donors), subject to the constraints imposed by the need to fund non discretionary expenditures, such as statutory expenditures. Third, the sector working groups prepare their medium term budgets, consistent with their sector expenditure ceilings, to reflect the sectors’ priorities as identified in their sector expenditure plans. To implement these principles, it is essential that all of the resources used to fund Government expenditures are channelled into a common "pool" of resources, from which expenditures can be allocated according to Government’s own budgetary priorities, and that all Government expenditures are determined as part of the national budget process. These principles are not compatible with the approach implicit in the global funds, or with any form of aid (including project aid and earmarked sector budget support) which is directly tied to specific expenditures or increases in sector budgets. The concept of "additionality"xii associated with the global funds implies that the size and/or inter sectoral composition of the Government budget, as well as the intra sectoral composition of the relevant sector budget, would effectively be determined outside of the Government’s normal budget process, on the basis of how large a volume of financial resources can be mobilised from donors. For example, if more aid is promised by the GFATM, Government spending on those items in the budget which are financed from the GFATM will have to rise by the full amount of the additional funds promised by the GFATM. This means that, either the whole Government budget increases by the amount of the additional GFATM funds, or some other items of expenditure, either within or outside the health budget, will have to be squeezed to accommodate the GFATM funded expenditures. The expenditures which are cut may be a higher priority for Government than the expenditures funded by the global fund, either because they better reflect Government’s own priorities or because they offer better value for money, in which case the money provided by the global fund will have distorted the Government budget in a manner which is suboptimal. International organisations and donors are hardly better placed to determine Uganda’s optimal budget allocations than is Government through its consultative budget process. Moreover, whereas Government formulates its medium term spending plans in a comprehensive manner, taking account of the needs of all sectors of the budget, so that inter-sectoral allocations reflect the relative priorities and needs among the different sectors, each global fund focuses only on the budgetary needs of its sector in isolation from all other sectors of the budget. Consequently, if sector budgets were determined on the basis of the resources provided by global funds, or any other type of earmarked donor funds, this would destroy the internal coherence of the budget, reflected in the optimal balance of spending between sectors. It is imperative for rational budget planning that the size and composition of the Government budget is determined through a centralised process, driven by the MFPED, and not through an atomised process driven largely by the availability of sector specific donor funds, in which each individual sector’s budget is determined without any reference to the needs of other sectors or other economic objectives. The Commission on Macroeconomics and Health (2001) advocated the setting up, in each developing country, of a National Commission on Macroeconomics and Health, comprising Ministries of Finance and Health and other agencies, to "scale up" health spending, draw up financing plans and determine spending priorities. This proposal would also directly undermine rational budget planning, because it would effectively take the planning of health spending out of the normal budget process, and give it privileged status over other sectors of the budget. The size and financing of all components of the Government budget must be the responsibility of the Ministry of Finance if public finances are to remain on a sound footing, not a national commission whose main objective, however important, is not sound fiscal policy. Conclusion
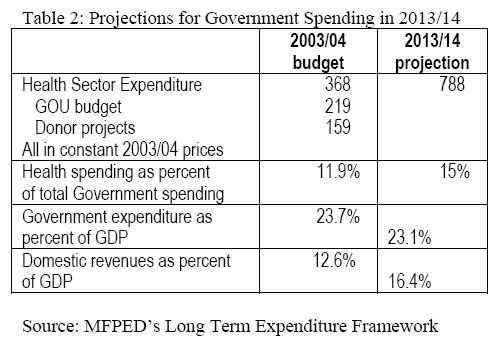
To achieve Uganda’s poverty reduction targets, set out in the Poverty Eradication Action Plan, fiscal policy must support private sector and export led economic growth. In particular, the fiscal deficit cannot be too large that it shifts price incentives against traded goods production or crowds private sector borrowers out of credit markets. This inevitably constrains the growth rate of public expenditures, hence to maximise the expansion of those public services which best contribute to poverty reduction, it is essential to improve the efficiency of public spending, control unit cost increases and better focus the allocation of public expenditures on priority areas. In terms of sector budget policy, it means that each of the sectors must plan their budgets within the constraints of their sector ceilings, by improving efficiency and identifying the priority targets which can be achieved within the sector ceilings. The hard budget constraint provided by the sector ceiling gives the sectors strong incentives to prioritise their expenditures, improve efficiency and control costs. This is a fundamentally different approach from that advocated by some of the international organisations, which envisage each of the sectors costing the expenditures required to meet all of their targets, and then seeking to mobilise the resources required to fund these expenditures from donors. Such as approach provides no incentives to the sectors to control costs or prioritise expenditures. The MFPED has drawn up a Long Term Expenditure Framework (LTEF) which sets out a 10 year budget ceilings that are consistent with projected budget resources and macroeconomic objectives. Total Government spending will increase, in nominal terms, by almost 150% over the next 10 years, provided that Government can meet its domestic revenue generation targets. The health sector is a priority area for budget policy and can, therefore, expect to be allocated an increasing share of the budget over the next 10 years. If Government raises the health sector’s share of total Government expenditure to 15%, the health sector can expect to receive a nominal increase of 213% over the next 10 years. If average inflation in the public sector can be held in line with projected underlying inflation of 4% per annum, real spending on health will rise by 114% over the next 10 years, or by 55% in per capita terms if population growth remains at 3.4% per annum (see table 2 below). Government policy is to reduce the share of Government expenditures which comprise donor funded projects, and increase the share of the GOU budget. Over the next 10 years, this should enable the share of the health sector’s expenditures funded from the GOU budget to rise from the current level of 60% to between 80% and 90%, which will facilitate an improvement in the efficiency of expenditure and a better prioritisation of expenditures, because many donor funded projects involve high unit costs and low priority expenditures.xiii The health sector’s GOU budget could triple in real terms if donor funded projects were restricted to 15% of total Government health spending. Adopting a prudent fiscal strategy which will support robust and broad based economic growth, does not mean that Uganda cannot achieve any of the MDGs. The income poverty goal and at least some of the social sector goals should be attainable if strong GDP growth is sustained over the next 10-15 years. In contrast, Uganda would undermine its prospects for achieving the MDGs if it were to pursue too expansionary a fiscal policy which damaged the prospects for rapid and equitable long term economic growth. References
End Notesi Ranson et al (2003) examine the extent to which expanding access to health care is constrained by factors other than lack of finance, such as constraints related to demand for health services, weak health systems and broader economic, social and political factors. They draw up a country typology with 84 developing countries classified into four quartiles, from the most to the least constrained quartile. Uganda is classified in the second most constrained quartile for most of the indicators used to evaluate the constraints. ii The funding gap is defined as optimal spending minus current spending. iii The Millennium Project estimates funding requirements in 10 areas: hunger, education, gender equality, health, environment, water supply and sanitation, improving the lives of slum dwellers, science and technology, energy and roads. iv The Millennium Project assumes no household contribution to basic health care spending. vI have assumed that defence expenditures average 2% of GDP: the Millennium Project does not project defence expenditures. Total Government spending would be higher than 37% of GDP if some of the donor funded projects are not in MDG related areas, as is currently the case. vi As well as the gap between total expenditure and domestic revenues, gross aid inflows would also have to cover repayment of external public debt, which will average about 1% of GDP over the 2005/15 period. vii Government expenditures in the health sector amounted to Shs 337 billion in 2002/03. The Uganda National Household Survey 2002/03 found that households allocated an average of 4% of their consumption expenditures to health, which amounts to a total of Shs 365 billion (Uganda Bureau of Statistics, 2003: 45) viii It would only be possible to expand public expenditure on non traded goods without shifting resources out of traded goods sectors if there was excess capacity in non traded goods sectors which could be brought into production by increasing demand, but this is unlikely to be the case in Uganda, because aggregate demand in Uganda has grown rapidly for many years. Over the last 10 years, nominal expenditures have grown by an average of 12.4% per annum, hence it is unlikely that production in the economy is constrained by a lack of aggregate demand. ix Public goods and services can be provided directly through Government provision or through private sector contractors selling goods and services to Government. x The provision of public goods may help to improve the static efficiency of resource allocation in the economy, where these goods involve positive externalities or help to mitigate market imperfections, but the public sector does not face pressure from market forces, in the sane way as does the private sector supplying competitive markets, to continuously improve the efficiency with which goods are produced. xi In 2002/03, 50.4% of households whose head reported that his/her main activity is crop farming (both food and cash crop farming) were living below the consumption expenditure poverty line. These households comprised 69.9% of all households which were below the poverty line in Uganda (UBOS, 2003: 53). xii Additionality is easier to define in principle than to apply in practice. In principle, it implies that an additional dollar of global funds will be added in full to the existing budget for the expenditures to which it is targeted, so that those expenditures are one dollar higher than they would have been in the absence of the global funds. In practice, the base to which donor funds should be added is rarely static until a budget is finally appropriated by Parliament (when it cannot be increased without a supplementary appropriation), hence there is no definitive base to which donor funds can be added. xiii Analysis by the Ministry of Health indicates that only 32% of the expenditures under donor funded projects comprise the priority expenditures costed in the Health Sector Strategic Plan (Republic of Uganda, 2003B). |

{kind=link}
{kind=link}
{kind=link}
{kind=link}