 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
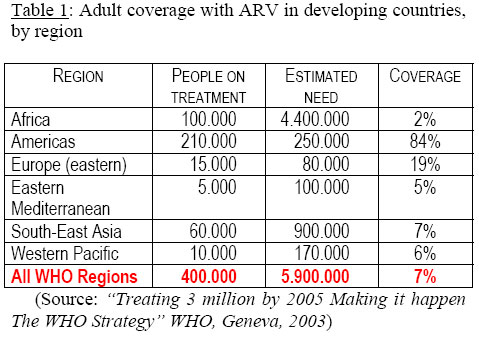
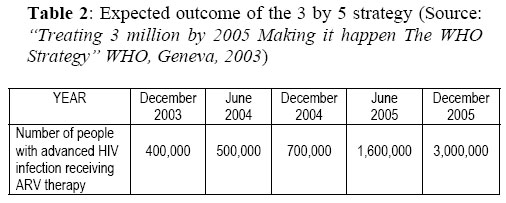
Health Policy and Development Journal, Vol. 2, No. 1, April, 2004, pp.52-61 ARV TREATMENT IN POOR SETTINGS: THE STATE OF THE ARTLuigi Cicciò, Visiting Lecturer, Department of Health Sciences, Uganda Martyrs University Code Number: hp04013 AbstractUniversal access to antiretroviral drugs (ARVs) has created enormous debate and controversy in developing countries. But it seems to be a more feasible prospect by the day. Prices of ARVs have dramatically come down, and there is an unprecedented commitment by the international community to make universal access to ARVs happen, under WHO’s initiative of 3 by 5. However there are a number of issues to address. First, the criteria for selection of those to be on treatment have not been agreed upon, especially using clinical methods. Second, the compliance to ARVs has been found to be problematic in Africa. It would require a Directly Observed Treatment Strategy (DOTS) approach to improve on compliance. Third, universal access to ARVs will require integration into national health systems, and strengthening these systems. Fourth, monitoring ARV treatment for safety, effectiveness and acceptability will be critical. This will require investment in laboratory services as well as in information management systems. Fifth, sustainable financing of ARVs will require Governments to commit, for a long time to come, substantial funding for ARVs, and to the health systems into which ARVs are to be integrated. Lastly, there are risks that need to be expected and prepared for up front. These include increasing the infectitious periods of people on ARVs by prolonging their lives; leakage and misuse of ARVs and the consequent drug resistance that may occur; and a possible disabling or even collapse of health systems because resources are shunted to universal ARV provision. Nevertheless, the treatment of AIDS that was denied to poor countries on grounds of cost, lack of infrastructure, and other excuses is now more than ever possible to the people of these countries. IntroductionFew areas of public health have generated as much debate, controversy and protest as the drive to expand access to antiretroviral (ARV) treatment in developing countries. Several years ago it was a futile discussion: drug annual cost of US$ 10,000 per patient was a major obstacle for a widespread diffusion of treatment in developing countries. Nowadays, largely as a result of a powerful combination of public activism and generic competition, prices have substantially dropped, with triple therapy now available for as little as US$ 132 per patient per year (1). Subsequently, the debate about this sensitive issue has grown, together with the concern of expanding the tangibly beneficial effects of ARV therapy to the most HIV-affected areas of the world. Arguably, this debate delays the urgent need to implement a comprehensive global AIDS strategy, where treatment and prevention are complementary and should not compete with each other for efforts and resources. A series of papers (2,3,4,5) have been produced in late 2003 about introduction and scaling-up of ARV therapy in resource-poor settings, slightly shifting the discussion from ethical and philosophical concerns to practical and concrete steps to be taken and critical issues to be considered. There is widespread awareness that the inequality between the rich world – where ARV therapy has heavily contributed in drastically reducing HIV-related morbidity and mortality (6) – and the poor world – where over 90% of the estimated 40 million infected persons live – is truly unacceptable and represents a "moral scandal"(7). Universal access to antiretroviral drugs (ARVs) has created enormous debate and controversy in developing countries. But it seems to be a more feasible prospect by the day. Prices of ARVs have dramatically come down, and there is an unprecedented commitment by the international community to make universal access to ARVs happen, under WHO’s initiative of 3 by 5. However there are a number of issues to address. First, the criteria for selection of those to be on treatment have not been agreed upon, especially using clinical methods. Second, the compliance to ARVs has been found to be problematic in Africa. It would require a DOTS approach to improve on compliance. Third, universal access to ARVs will require integration into national health systems, and strengthening these systems. Fourth, monitoring the ARV treatment for safety effectiveness and acceptability will be critical. This will require investment in laboratory services as well as information management systems. Fifth, sustainable financing of ARVs will require Governments to commit, for a long time to come, substantial funding for ARVs, and to the health systems into which ARVs are to be integrated. Lastly, there are risks that need to be expected and prepared for up front. These include increasing the infectitious periods of people on ARVs by prolonging their lives; leakage and misuse of ARVs and the consequent drug resistance that may occur; and a possible disabling or even collapse of health systems because resources are shunted to the universal ARV provision. Nevertheless, the treatment of AIDS that was denied to poor countries on grounds of cost, lack of infrastructure, and other excuses is now more than ever possible to the people of these countries. (Table 1) The expected scaling up within December 2005 is shown in Table 2. Though this commendable initiative by WHO is very much welcome, trying to reduce a striking disparity that Nelson Mandela defined "a travesty of human rights on global scale" (9), there are a number of issues to be analysed, that need a close examination in order to successfully implement the 3 by 5 strategy. Selection of patients Clear biomedical, economic and social criteria are required to determine eligibility for treatment in contexts where ARV will not be available initially to all those who could benefit. WHO guidelines for resource-poor settings (10) recommend treatment for people who have a CD4 cell count below 200 and people with WHO-defined symptomatic disease stages of 3 or 4. But it has been argued that these guidelines may be less appropriate where most HIV-associated infections occur in patients with CD4 cell counts above 200, highlighting the need to look critically at the potential benefits of starting treatment earlier (11). Moreover these guidelines are not easily applicable wherever the CD4 cell count is not available because too expensive or too sophisticated: in these cases, the presence of a total lymphocyte count of 1200/dl or below may be used as a substitute indication for treatment in the presence of symptomatic HIV disease. However, the presence of symptoms is often suggestive of low immunological status: a study in Rakai District, Uganda, compared patterns of reported symptoms with CD4 count above 350 (12). In the meantime, cheaper and simpler alternatives to CD4 lymphocyte count and HIV-1 RNA – the two basic measurements for patient assessment and monitoring – are being tried and tested, showing some contradicting results (13). A simple method (14) that uses dried blood spots could significantly reduce the cost of CD4 cell counting, but the procedure proved less reliable for counts lower than 200/mm3, thus limiting its future utilisation. Both of these tests involve sending blood to qualified laboratories where trained technicians use sophisticated equipment to obtain reliable and reproducible results. The cost of these tests can range from $60 to well over $100 each. There are a number of ongoing efforts to simplify the measurement of HIV RNA and CD4 counts by using alternative technology that doesn’t require expensive laboratory equipment or by relaxing the precision of the tests so that they simply return a pass/fail result instead of a numerical readout, but these advances are years away (15). Another avenue of research into affordable diagnostics has been to develop alternative markers of treatment success that don’t rely on HIV RNA. One of these methods involves looking at blood levels of an HIV protein called p24, but the promise of p24 as a cheaper and reliable marker of treatment response failed in a study conducted in Western Africa (16). However, clinical aspects are by no means the most difficult ones to agree upon: in the case of insufficient availability of drugs, where the "necessary evil" of setting priorities among all the potential beneficiaries of the treatment is compulsory, clear and transparent criteria for selection are required. The pilot ARV scheme conducted by MSF in South Africa (17) offers an interesting example of how to manage such a sensitive and difficult issue: in the suburban setting of Khayelitsha, HIV clinics have been providing treatment only to those patients meeting the following set of criteria: biomedical (CD4 cell count), adherence (having regularly attended the clinic for three months) geographical (living within the catchment area of the project) and social (number of dependants, health status, income and degree of activism). Moreover, a participative method was introduced that involved the community in the process of selecting patients: a number of community representatives met regularly together with health care providers to assess candidates and determine who would ultimately be placed on therapy. CompliancePast experience on adherence suggests that compliance with prescribed drug treatment in Africa may be problematic: this represents one of the major concerns for extensive scaling up of ARV therapy, given that its success depends on long term, regular, time specific dosing. It is a widely held assumption that people in resource-poor settings will be unable to be adherent for long to antiretroviral therapy, providing yet another barrier to their access to medicines essential to their care. It has been proposed that administering ARV therapy through the directly observed treatment short course (DOTS) strategy would ensure the necessary adherence (18): indeed, tuberculosis has some similarities with HIV/AIDS and the two diseases share many management requirements. A community-based project implemented in Haiti (19) has obtained a very notable degree of compliance. Yet, DOTS itself has met with mixed success and controversial results, with many African countries still under the cure rate of 70% (21). Furthermore, pilot studies reporting successes in providing ARV drugs in Africa have had relatively strict exclusion criteria, with most of them delivered in urban settings to individuals with above average education level and income, and therefore not very representative (21,22). However, a recently published paper (23) reports the findings from an investigation designed to measure adherence in a cohort of semi-urban South Africans living in extreme poverty: the achieved adherence and viral suppression results match or even surpass those reported in most observational or clinical trial cohorts in developed countries. The authors’ important conclusion is that low socio-economic status individuals should never be discriminated in access to ARV treatment on the basis of otherwise unsubstantiated expectations of poor adherence. It is even important to remember that the majority of HIV-infected individuals receiving ARV therapy in most European countries initially consisted of one of the less compliant population of patients, that is the intravenous drug users, but this never prompted clinicians and public health specialists to exclude them a priori from treatment! In the South Africa MSF experience (24), the major factors positively affecting long-term adherence to treatment were an easy-to-take drug regimen and dispensing health facilities within easy reach of the patients; besides, individual support through "treatment assistants", peer support and educational material were shown to be also important. When proper treatment compliance is not fulfilled the very serious consequence is drug resistance. Like for TB treatment, this is the heaviest threat to ARV therapy: from the individual perspective, being cross resistance common among drugs of the same class, drug resistance would affect the success of the therapy, limiting the number of possible valid alternatives. From the public health perspective, drug resistance virus strains are transmissible and have the potential to undermine the effectiveness of the drug regimen in the newly infected individuals. Currently, in industrialised countries, up to 23% of incident infections are with virus strains resistant to one or more drugs (25). Drug resistance can be also induced by sub-optimal drug regimens, unable to reduce the viral load and the emergence of resistant strains. This was distinctly highlighted in the evaluation of the Uganda Drug Access Initiative (26), where the 47% of patients were prescribed the less suppressive dual rather than triple therapy regimen and developed more frequently drug resistance, particularly to lamivudine. Actually, delivering ARV medicines outside the officially accredited health facilities or providing them according to the patients’ ability to pay, they both bear the concrete risk of utilising ineffective regimens and allowing virus replication, thus introducing new resistant virus strains. Therefore, one essential requisite for the ARV treatment scaling up consists of the integration of the programme into the existing health system. Integrating ARV treatmentA number of countries have already started to provide ARV therapy, and recently many more have announced plans to introduce or scale up its provision (27). The increase in the number of countries with plans for large-scale public sector distribution is largely due to the availability of additional resources from the GFATM and other sources. Approaches to introducing and scaling up public sector provision of ARV vary: these approaches tend to fall into one of three categories or ‘models’: provincial or regional hospital delivery, district level delivery, and community clinic or community level delivery. But scaling up care and treatment programmes is best achieved through collaboration and coordination between a mix of providers: therefore, other key ARV providers are the nongovernmental organisations and the private sector. The former are well represented by MSF primarily, which is running pilot programmes in Cameroon, Kenya, Malawi, South Africa and Mozambique; by the Lighthouse Trust in Malawi, which combines charitable funding and government support and works closely with the Ministry of Health; by Uganda’s Joint Clinical Research Centre (JCRC), which is the generic drugs leading distributor in Uganda and operates an ARV clinic in Kampala. The latter consists mainly of private company schemes and private physicians. A growing number of private companies – mostly large enterprises and multinational companies – are starting to provide ARV to their employees: for example, Coca-Cola has established since 2000 an employee health care programme, which is operational in most African countries (28), including access to ARV treatment. There is evidence from Africa that introducing ARV therapy to HIV-infected employees leads to substantial cost saving for companies (29): a survey conducted among 216 companies in Uganda, Kenya and Tanzania showed that qualified and experienced workers infected with HIV are reported to be seeking early retirement, thus leaving sensitive operations to inexperienced employees, resulting in low productivity (30). At the same time as some companies are expanding treatment access, there is also a trend among private sector firms in Africa to shift the burden to households and to government, through practices including pre-employment screening and restructuring and reducing employee benefits (31): in Uganda, for instance, the New Vision, Standard Chartered Bank, BAT and Sheraton Hotel expect employees to pay 50 per cent of the cost of ARV (32) and almost a third of the organisations surveyed in Uganda in late 2003 exclude HIV/Aids treatment from their health care package (33). Controlling the HIV epidemic requires large scale investment in the public health infrastructure of resource poor countries as well as action to tackle factors such as poverty and external debt. A major objection to the expansion of ARV therapy in developing countries is the chronic inefficiency of their health systems, their dilapidated infrastructures, their poorly-remunerated, often untrained, demotivated staff, their poor management of supplies and logistics. This current situation is seen to be possibly overwhelmed by the formidable burden of activities required by scaling up ARV treatment. The challenges to meeting the urgent demand for ARV care include widespread knowledge about treatment, making decisions about new regimens, early detection of emerging drug resistance, uninterrupted drug supplies, highly accessible voluntary counselling and testing, laboratory capacity for treatment monitoring, trained healthcare workers (34). Strengthening the Health SystemsThe key issue facing policymakers, therefore, is not whether to include ARV therapy into the essential package of services, but strengthening the existing health system capacity and determining the proper balance of resources to be devolved to each intervention. In such a situation it is not surprising that initiating treatment services would take the easier route of providing ARV in the "comfort zone" of academic hospitals and the main urban areas (35), where beneficiaries are likely to be educated, higher-than-average income people, whose accessibility to services would be further enhanced. For sake of equity’s issue, it is essential that this implementation will not drain resources away from the already under-financed rural and poorer regions and to ensure that the expansion programme, with its skills and resources, will be deployed in the entire health system. The possible risk, otherwise, is that "ARV [programmes] introduced in a selective way based on the capacity to run programmes and in those districts with the best services, will be given extra resources. This will not only increase inequity directly but also indirectly, by attracting scarce human resources. Even if ARV are introduced everywhere, the likelihood is that there will be good care in some areas and inadequate and sub-standard care in the poorer areas" (36). There are three paramount issues concerning the strengthening of public health systems in the process to ARV treatment expansion: infrastructures, human resources and drugs supply. There is a lack of clarity about minimum infrastructure for ART delivery and how to cost this. Kenya is one of the few countries to conduct a situation assessment of public health facility infrastructure. The assessment identified a number of infrastructure constraints: some facilities were found to have inadequate physical infrastructure and to require expansion and upgrading, including the design and arrangement of laboratory and pharmacy space (37). In Uganda, the Ministry of Health developed accreditation criteria for clinical centres that would be authorized to prescribe ARV therapy. Currently, 25 sites have been accredited in Uganda and 23 are providing ARV therapy. Of the 10 regional hospitals, 6 (Arua, Mbarara, Kabale, Lira, Masaka and Gulu) are providing ARV therapy. The minimum criteria for a health facility to be accredited include setting and achieving targets for the comprehensive basic health care services as outlined in the minimum health care package, the presence of basic physical infrastructure (space for HIV counselling and testing, clinical assessment, drug storage and laboratory), minimum numbers of qualified personnel with experience in HIV/AIDS management and the ability to ensure the provision of follow-up care and support for families and communities with people living with HIV/AIDS (38). Health sectors in poor countries face a crisis in human resources (39): inability to recruit and retrain an appropriately skilled and motivated workforce stems from problems of low pay and morale, poor working conditions and inadequate management. Shortage of staff is moreover worsened by migration to other countries (40,41). In this consolidated context, HIV impacts on organisations in a number of ways (42):
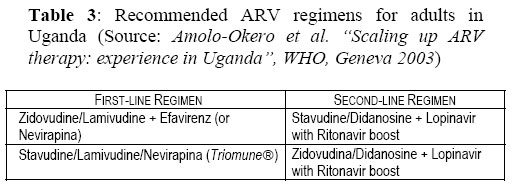
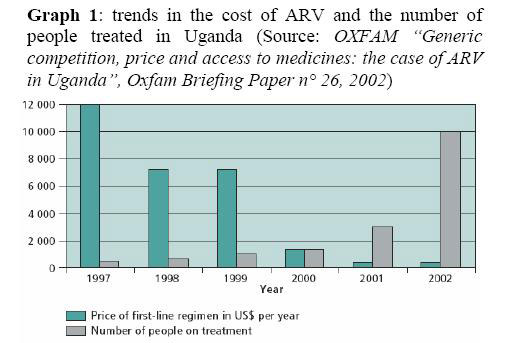
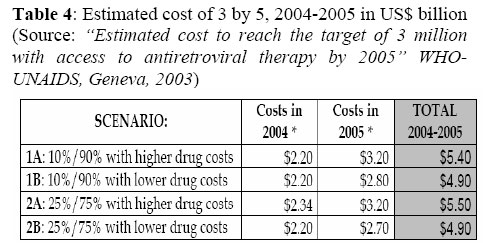
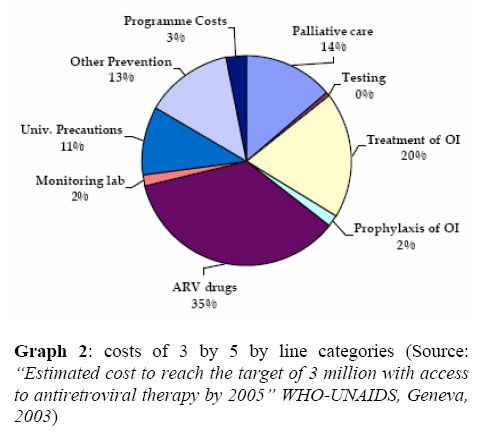
These severely affected health systems are called to overstretch its workforce with the additional task of expanding ARV therapy to PHC facilities. Crucial issues are the training or re-training of personnel, with special emphasis on the use of drugs (appropriate combinations of triple therapy, alternative choices, monitoring of effectiveness and side effects, etc.) and also on drugs logistics and management. The challenge of building a reliable system ensuring a regular, uninterrupted supply of drugs, reagents and other supplies is the third issue health sectors are facing in scaling up ARV treatment. In many countries, the registration process is slow and complex and legal barriers to the importation of generics still exist. Logistics challenges associated with procurement include: lack of information for appropriate drug selection, delays, corruption, and lack of management capacity. The most common weaknesses in drug management (not only ARV drugs!) are: poor storage facilities, weak transportation systems, problematic customs processes, diversion of products, inadequate training, lack of information systems, inaccurate quantification and forecasting (45). An important issue is accurate estimation of drug requirements: in most developing countries, this is based on consumption rather than morbidity data (46), applying annual changes in an "incrementalist" manner; but the consumption method, though quick and easy, is heavily affected by and cannot provide corrections of inaccurate recording or irrational prescriptions, which are very common problems in resource poor health sectors (47). Finally, the necessary Logistics Management Information Systems to be installed will need to be user friendly, have a minimal burden on health workers, be able to provide timely data, and be flexible enough to respond to changes in consumption due to patient mobility, regime changes, drug substitution. Monitoring ARV treatmentAlthough safety, effectiveness, and acceptability should govern the choice of ARV, individualised regimens may not be possible in many environments. National guidelines on standardised first-line and second-line regimens, eligibility criteria for starting ARV therapy, and patient monitoring are essential, to assist planning of drug procurement, limit the number of drugs to manage, simplify training of health care providers using standard clinical management protocols and education of patients, and develop simple and effective monitoring and evaluation systems. Clinical guidelines need also to describe how to manage adverse effects, where and when to refer patients and to include treatment of opportunistic infections, aiming to maximise the benefits of ARV. These national guidelines are very much needed when many providers are involved in ARV treatment delivery, to keep therapy approaches uniform; what is most important, is to avoid illogical prescriptions of mono or dual-therapy, which have very narrow prospects of being effective in the long-term and create an illusory confidence in patients. Uganda provides a very good example of how ARV treatment can be simplified in practice (48): two regimens have been prescribed as first-line treatment and two as a second-line alternative (see Table 3). The first-line treatment utilises a non-nucleoside as the third drug, because it is less expensive, and preserves the possibility to use a protease inhibitor at a later stage (49). Deciding when to initiate ARV therapy is not the only clinical key issue: decisions whether and when to change treatment are absolutely essential. Changing too soon carries the risk of exhausting ARV options, whereas continuing with a failing regimen may lead to viral resistance (50). An apparently promising alternative to established ARV treatment scheme is the structured treatment interruption, whose clinical outcomes seem to be comparable to those of uninterrupted treatment (51). This method could potentially reduce costs, minimise side effects and simplify monitoring procedures for providers, though it requires clear instructions for both clinicians and patients. In January 2003, the DART study for evaluating interrupted treatment was initiated in Uganda (52), and it will be followed up for the following five years, to evaluate its potential feasibility settings. ARV treatment has several characteristics suggesting that regular laboratory monitoring is important. If clinical algorithm are useful to orientate health providers in the choice of the first and second line regimens, good quality laboratory facilities are required to inform clinicians of immunological and virological response to treatment, as well as drug side effects. Among the latter, anaemia (to which ARV toxic effects contribute together with nutritional deficiencies and parasitic diseases), abnormal liver function, pancreatitis and peripheral neuropathy are among the most common, creating the need for their early detection by a quick and reliable laboratory. Monitoring the virological and immunological condition appears to be much more difficult: the available tests are prohibitively expensive and technically more complex. Whilst the price of antiretroviral drugs has fallen, the price of CD4 (approximately US$50) and viral load (approximately US$150) monitoring tests has not (53). Meanwhile cheaper and simple alternatives are identified and tried, the best combination of syndromic management, less frequent surveillance and simpler monitoring tests could provide with a way to overcome the barrier of inadequate ARV monitoring. Financing ARVsOne of the biggest issues about the expansion of ARV treatment in Africa is the question of who will pay for it. African national governments are urged to give themselves a policy framework for a comprehensive national response to HIV/AIDS (54), which can provide guidance for activities geared towards preventing the spread of HIV and mitigating its effects. This framework should consistently be part of the poverty reduction strategy, given that the poor are usually the more vulnerable and less privileged in accessing any health care provision. As a matter of fact, most household expenditure in Africa takes the form of direct fee-for-service payments, predominantly, and community financing schemes, which are still at their infancy. Unless mechanisms to exempt the poor from user charges exist, they can result in untreated morbidity, reduced access to care and long-term impoverishment: but previous experience has shown that exemption schemes for the poor frequently do not work (55). Translating this situation to ARV scaling up strategies requires the proportion of health financing coming from out-of-pocket payments, if any, to be drastically reduced to minimise health systems inequities. Decreasing drug prices have been a significant factor in enabling governments to provide ARV through the public sector. Drug prices have come down substantially, as a result of increasing competition and availability of generics. Competition among generic producers has also pushed brand medicine prices down. Bulk international procurement by Foundations or international agencies is much more convenient in bargaining lower prices, than it may be for national governments separately. Besides, an analysis of additional tests, procedures and out-patient visits associated with the provision of ARV concluded that the cost ranged from $70 per month to $140 per month (56). Oxfam conducted a study of generic competition, price and access to ARV, using Uganda as a case study (57): during the Accelerated Access Initiative in 2000, 5 drug companies agreed to reduce the price of some ARV and subsequently the JCRC started to import low-cost generics from India, increasing the number of patients it was able to treat (see Graph 1). Its conclusion is that generic competition is crucial, reducing the price of patented medicines dramatically; that relatively poor people will buy life-saving medicines, but make enormous sacrifices to do so; that there is a the need for systematic and transparent tiered pricing and to maximize the use of TRIPS (considering that after 2005, countries like Uganda will no longer be able to import generic versions of newly-patented drugs, because generic producing countries like India will no longer be able to export them). Studies have tried to establish the appropriateness of introducing and maintaining a ARV provision programme, using the lens of economic evaluation (58,59,60): some of them reached the conclusion that other interventions are still more cost-effective than providing ARV to HIV-infected people in poor countries. However, these arguments often ignore that ARV are the best prophylaxis for opportunistic infections, thus no longer requiring primary or secondary expensive chemo-prophylaxis or high rate of hospitalisation. The extent to which the cost of purchasing antiretroviral drugs is totally, or partially, offset by savings through the reduced number of hospitalisations and opportunistic infections remains unclear. However, once indirect costs (i.e., productivity losses associated with morbidity in HIV-infected individuals) are taken into account, ARV therapy is clearly cost-saving in developed societies (61,62). It is now necessary to acknowledge that prevention-only interventions cannot stand alone and need to be sided by curative interventions, considering the worrying high prevalence rate of the adult population. The dramatic reduction in drug costs together with the implementation of the current recommendations to initiate treatment at a level no lower than 200 CD4 cells (a baseline condition with higher probability of survival) should then improve the cost-effectiveness ratio (63), making convenient what has shown to be already feasible. Nevertheless, a joint tireless effort is required by the national health sectors, the donors, the international agencies, in order to make the expanded access to treatment sustainable and never to recede once it has started. In fact, WHO says that even with the cheapest drug prices, the cost of implementing 3 x 5 will reach $4.9-5.5 billion by the end of 2005 (see Table 4) (64), with only 35% of that cost comprises ARV(see Graph 2). Predictable risksARV therapy has demonstrated effectiveness and positive long-term outcomes. These outcomes are primarily for patients themselves, in terms of reduced mortality, reduced episodes of opportunistic infections (including TB) and improved quality of life (65); for the households and communities, both sharing a positive social and economic impact (66); for the private sector companies, which experience reduced hospitalisation, absenteeism, and treatment costs for ill employees; and eventually for the health system due to the unequivocal reduced burden on health facilities of HIV-related admissions and morbidity. Yet, there is a notable debate about possible negative implications of introducing and expanding ARV in developing countries. First, the prolonged individual’s life could increase the period of infectiousness and therefore the risk of spreading HIV infection. This can be partially balanced by the reduced viral load of patients under regular treatment and by sustaining health education among patients and their relatives. Secondly, there is a concern that availability of drugs could divert attention from preventive measures and behavioural change, thus driving people towards unsafe behaviours and practices. The overall impact on behaviour and implications for the spread of the epidemic in developing countries remain unclear: anyway, in Brazil, AIDS case reporting has increased, indicating that the availability of treatment provides an incentive for people to seek HIV testing (67). Programmes that have strong community links are likely to have noticeably more positive outcomes; however, education remains a critical component to correct misconceptions about ARV, in particular the idea that these drugs are a cure for HIV/AIDS. Another concern is about the possible "leakage" of drugs outside the official channels into the open market. The large experience with drug pilferage in government health units and the expected "ARV craving" from people still unable to access it through the dispensing facilities could realistically foster this dangerous problem. In fact, according to a recent report (68), drugs were being sold in Nairobi’s street markets, where people could purchase a few tablets or substantial quantities of drug without doctors’ prescriptions. This is obviously very risky, both for the severe and complex side effects of the medicines and for the possible resistance emerging from inconsistent drug use. This situation of unregulated ‘therapeutic chaos’ is likely to lead to further inequity as the poor more commonly use informal and unqualified providers, being the victim to unscrupulous practice(69), and is likely to lead to the emergence of drug-resistant viral strains that need new combinations of drugs or new drugs altogether(70). Finally, the large scale implementation of ARV therapy could be seen as absorbing resources and energies from other health activities and basically from prevention programmes. Instead, treatment could provide a way of contact with the health provider, who can reinforce prevention messages(71), as well as with peers, whose support, advice and experience is essential for maintaining motivation of patients. Besides, improving care will serve directly to strengthen prevention in a number of ways. These include: increasing demand for voluntary counselling and testing(72); reducing stigma and promoting greater openness in discussions of HIV/AIDS in the community; and helping to keep families intact and economically stable, thus slowing the growth of at-risk populations such as orphans and sex workers (73). And eventually, pregnant mothers would be much more willing to undertake mother-to-child transmission prevention programmes, if drugs were available to continue with treatment after delivery. ConclusionDira Sengwe ("Act now!") was the slogan of the first South African AIDS National Conference last August: this could very significantly highlight the urge to introduce ARV therapy in a country where the political climate has ever been controversial on this matter (74). Elsewhere, the opponents of a ARV scaling up process are still quite many and their arguments cast relevant doubts on an issue perceived by the majority as an ethical one. However, many of these arguments tend to ignore that African countries in particular are facing the most challenging public health emergency they have ever experienced. In the face of such a dreadful pandemic, it appears unjustified to limit their access to the treatment they badly need. The international agencies, the policymakers, the politicians and the Global Fund architects and partners should rather integrate the availability and affordability of ARV treatment for all HIV-infected populations in resource-constrained settings as one of their primary, most fundamental goals. We have reached a turning point in AIDS where access to treatment for HIV-infected adults and children in developing countries can no longer be refused on cost grounds, lack of infrastructure, or other priorities. For the first time, there is evidence that a change in paradigm is now attainable. References
Copyright 2005 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp04013g1.jpg] [hp04013t2.jpg] [hp04013t1.jpg] [hp04013t4.jpg] [hp04013g2.jpg] [hp04013t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}