 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 2, No. 1, April, 2004, pp. AIDS, Primary Health Care and Poverty Maurizio Murru, Senior Lecturer, Department of Health Sciences, Uganda Martyrs University Code Number: hp04014 Abstract
Copyright 2004 - Department of Health Sciences of Uganda Martyrs University
This paper analyzes the complex interrelation between poverty and AIDS. Poverty, in its many and diverse aspects and with its many and diverse consequences, creates a fertile breeding ground for the expansion of HIV/AIDS. In turn, HIV/AIDS, for its mode of transmission and its epidemiological features, badly affects the livelihood of its victims, their families, their entire communities and countries. Sub Saharan Africa bears the brunt of the epidemic. With about 10% of the world population, it has about 66.5 % of the world seropositive cases. In three Southern African countries the HIV prevalence in the adult population reaches or exceeds the level of 30 %. Recent WHO estimates put life expectancy in Sub Saharan Africa at about 47 years and that, without AIDS, it would be at about 62 years. The development achievements of the last decades risk being lost and the future of the continent is at risk. But numbers, alone, don’t tell the whole story. They don’t talk of millions of orphans, dilapidated health services, crumbling educational systems, illiteracy, gender discriminations, harmful cultural practices, uncontrolled urbanization, conflicts and civil wars, refugees and internally displaced people, entire economies on the verge of collapsing. In the rich countries, AIDS is no more a death penalty. It is a chronic disease that, although with problems, can be treated. For years the idea that the poor "had to be" excluded from the benefits of Antiretroviral Treatment (ART), simply because they are poor, has been accepted somehow passively. Things are now changing. The paper briefly touches upon ART and its implications. It is also stated that all deaths due to poverty and deprivation are unacceptable, not just those due to AIDS. The main conclusion is that the fight against HIV/AIDS is the fight against poverty. The resources to win this war are not lacking. What seems to be lacking are vision, political will and genuine interest in all human beings. Introduction
Primary Health Care (PHC) was not born at the Alma Ata Conference of September 1978. The Alma Ata Declaration produced by that Conference (WHO/UNICEF, 1978) resulted from the analysis of and the reflections on the experiences of the previous 20 to 30 years of delivery of health services. The most common approach had been curative, disease oriented, top down and health unit based. There had been exceptions. Disillusioned with the results achieved by that approach, many health workers, especially in poor countries, tried different strategies: community oriented, community based, health centred. The approach outlined in the Alma Ata Declaration was borne out of these experiences and out of the conviction that "health" is much broader than "absence of disease" and actions to protect and promote it go well beyond the health sector. The strong reaffirmation of "health" as a "fundamental human right" gave PHC its developmental approach and its highly political overtones. Obvious to many (although not to all) was the fact that to ensure a decent level of health to all (Health For All by the Year 2000) was a highly political undertaking. What was at stake was the use of the world resources, to achieve the morally imperative objective embedded in equity and social justice. Morally imperative as it was (and is) the PHC approach was a tall order, especially, as its call coincided with the first "oil shock" and came in the middle of a severe world economic recession. The proponents of PHC were strong in ideals and generosity but weak in the grey analysis of financial needs and economic implications. PHC was not granted the resources needed, the dreams waned and the promises were not kept. Throughout poor countries, this resulted in ineffective health systems, persistent poor health and stagnating development. Since the promises were not kept, many concluded that PHC failed. This is a blatant example of the "blame the victim" attitude (Segall 2003). What failed was the political will of ensuring that the PHC goals were achieved through a more equitable and just redistribution and use of the world resources. It was odd and somehow sad to see that even WHO, in its 2000 World Health Report, downgraded PHC to the rank of a mere "second generation" health reform (WHO 2000: 13-17). That the 2000 WHO Report was not only criticised but, for other reasons, strongly discredited (Musgrove, 2002), came as very little consolation for such an astonishing stand. If PHC is a "second generation" health reform, it is only natural for it to be replaced by "third generation" health reforms, inspired by a neoliberal economic approach, geared towards National Minimum Health Care Packages where cost-effectiveness is more important than equity. This technicist top down approach is not new. Its essence was outlined, when the ink of the Alma Ata Declaration was barely dry, by Warren and Walsh (Warren and Walsh, 1980). The philosophy behind it is reductive, it concentrates on diseases and technical short term measures loosing sight of the long term much wider measures necessary to face the real problems leading to poor health: poverty and inequality. Probably not by chance, this approach completely neglects the wider development agenda that is an integral part of the comprehensive PHC approach (Petersen and Swartz, 2002). The AIDS pandemic and its devastating wide range effects, especially in Sub Saharan Africa, reaffirm, in our opinion, the need of a broad based comprehensive approach. Technical narrowly sectorial remedies will not solve this dramatic crisis. An all round, multisectorial approach is needed. The role of poverty and inequality must be clearly recognised and the necessary political conclusions must be drawn. In this article we will touch upon the most important of the many facets of the complex problem of AIDS and its tight links to poverty, exclusion, discrimination and deprivation. The HIV/AIDS numbers
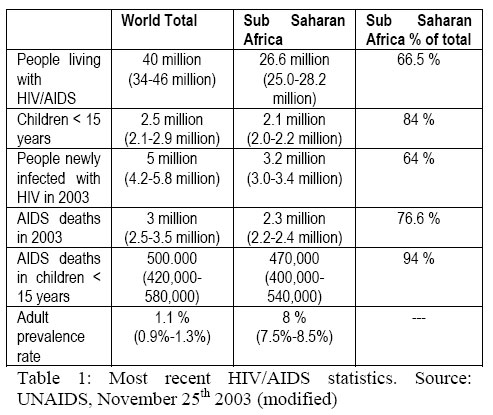
On June 5th 1981, the "Morbidity and Mortality Weekly Report" of the Centre for Disease Control (CDC) of Atlanta described, for the first time, what came to be called "Acquired Immuno Deficiency Syndrome" (CDC, 1981). The first cases in Sub Saharan Africa were reported in 1983 (Clumeck et al., 1983). By 1986 the magnitude of the epidemic in the continent began to be understood (Quinn et al., 1986). Today very few people fail to appreciate the seriousness of the AIDS problem in Africa and its even more catastrophic potential developments in the near future. Finally, even the South African Government, for years stuck on an inexplicable inertia fuelled by the intellectually flawed positions of President Thabo Mbeki, is waking up to the emergency and taking serious measures. Table 1, below, shows the most recent HIV/AIDS statistics, released by UNAIDS on November 25th 2003 (UNAIDS/WHO 2003 a). Sub Saharan Africa, once again, is bearing the brunt of the epidemic. With about 10% of the world population, it has well above its share of people living with HIV/AIDS (adult and children) and HIV/AIDS related deaths. As scaring as these statistics are, they are bound to worsen up to the end of the current decade. The AIDS epidemic is still at its initial stages in many African countries. Its impact will be felt, more and more, during the next decade and beyond (UNAIDS/WHO, 2002). In three Southern African countries the HIV prevalence in the adult population reaches or exceeds the level of 30 %: Botswana (39 %), Lesotho (30 %), Swaziland (39 %). Southern Africa, with about 2 % of the world population, has about 30 % of the People Living With HIV and AIDS (UNAIDS/WHO 2003). Recent WHO estimates put life expectancy in Sub Saharan Africa at about 47 years and add that, without AIDS, it would be at about 62 years (WHO 2002 a). There is much more than numbers Numbers often speak. But they rarely tell the whole story. In this era of high tech information, statistics are churned out easily and abundantly (sometimes irrespective of their real value and meaning. It is necessary to go beyond numbers and statistics. It is necessary to pause and ponder on the human meaning and realities implied in the dry numbers. As a recent UNAIDS report put it, "HIV infects and kills people, it tears apart families, destabilizes communities, slows economies, disrupts social services and weakens democracies. Entire societies become vulnerable to implosion".(UNAIDS 2003). Complex, simple reasons
The reasons for this desperate situation are complex and simple at the same time. They are complex because they are numerous, interlinked, with many social, economic and cultural ramifications. They are simple because they are rooted in one basic cause: poverty. Poverty itself is not a simple concept. At least four main different approaches are currently used in the attempt to define and measure it (Ruggeri Laderchi et al. 2003): the monetary approach (focusing on income and consumption), the capability approach (focusing on, less tangible realization of human potentials), the social exclusion approach (focusing on deprivation and marginalization) and the participatory method approach (focusing on people’s own perceptions and definitions of poverty through Participatory Poverty Assessments -PPA-). We see poverty as the result of a complex set of circumstances leading to material and social deprivation and lack of choice. Poverty, however one defines it, has many causes, many faces and many consequences. We will try to examine some of them. Dilapidated health services
In poor countries, health services are chronically and grossly underfunded. The average total health expenditure per capita, in Sub Saharan Africa, in 2000, was US $ 29, compared with US $2,735 in high income countries (4,499 in the United States) (World Bank, 2003). This leads to health services of unacceptably low quality delivered in dilapidated infrastructures by underpaid, undertrained, frustrated and cynical personnel lacking basic drugs and equipment. This situation has many consequences. One is that sexually transmitted diseases are diagnosed late and poorly treated or not diagnosed at all and never treated (Buvé et al, 2001). This favours the spread of HIV. Poverty, at the individual as well as the national level, implies no access to Anti Retroviral Treatment (ART) that can prolong life and improve its quality. In rich countries, thanks to ART distributed in the framework of well functioning health systems, AIDS is now a chronic disease rather than a deadly one. We will discuss the access to ART more in detail later in the article. Illiteracy
The average net primary school enrolment ratio, in Sub Saharan Africa, was 59 % in 2000 – 2001, compared with 97 % in high income countries, 93 % in middle income ones and 74 % in low income ones (UNDP, 2003). This statistics doesn’t capture the quality of education. This is very low in schools lacking books, elementary teaching materials, space, and with a pupil / teacher ratio of 47 (against 17 in high income countries) (World Bank, 2003). Poor education reduces the possibilities of appreciating a problem, understanding it and its solutions and making responsible decisions on what sort of behaviour to adopt in relation to it. Gender discriminations
Poverty also means greater and more engrained discriminations against women. In many African societies women occupy a lesser place within the family and within society at large (Caldwell et al., 1989). In the last 40 years the average period of schooling of women in Sub Saharan Africa increased by 1.2 years: the lowest growth rate in the world (World Bank 2000 a). Lesser social status means less power in deciding with whom, when and how to have sex. Young women often marry or have sex with older men. It is common for men to think that it is safer to have sex with teen age girls as they are more likely to be HIV free. Due to cultural as well as legal restrictions, in many African countries women have little access to property and little control of resources (Human Rights Watch, 2003, a.). Engaging in sexual relationships for money or "gifts" is common for many poor women who can not be defined as "sex workers" (Ferry et al. 2001). In these unequal partnerships women have little or no say on safer sex practices. Women account for about 58 % of people living with HIV and AIDS in Sub Saharan Africa (Human Rights Watch 2003 b). In several Sub Saharan African countries, the HIV prevalence rate in women between 15 and 19 years is four to seven times higher than in men of the same age (Human Rights Watch 2003 b). Biological and physiological factors also play a role. However, the fact that, worldwide, women represent about 46 % of people living with HIV and AIDS (UNAIDS 2002) suggests that the situation in Sub Saharan Africa is the result of power, not of biology. Harmful cultural and social practices
Poverty favours the survival of harmful cultural practices such as wife inheritance and ritual cleansing. Wife inheritance means that a widow is inherited by the brother (or another male relative) of the dead husband. Ritual cleansing means that a widow must have sex with a social outcast (usually paid for this "task") to be freed of her late husband’s "evil spirits". In these circumstances, safe sex is not the rule and sex is often forced on understandably unwilling women (Human Rights Watch 2003 b). The possible role of these practices in spreading HIV is obvious. Female Genital Cutting (FGC) is another harmful practice still widespread in many Sub Saharan African Countries. FGC is practiced in at least 28 countries worldwide. Prevalence rates among adult women vary from 5% in the Democratic Republic of Congo to 98 % in certain areas of Somalia (UNFPA 2000). Many African countries, like Burkina Faso, Djibouti, Egypt, Ghana, Senegal, Tanzania and Togo, have banned FGC. The enforcement of these laws is often weak. The cutting is usually carried out by untrained personnel and in unhygienic conditions favouring infections. Poverty, with its corollaries of poor education and lack of knowledge also leads to harmful practices. A fairly common one is that adult seropositive men, aware of their HIV status, do whatever they can to have sex with young girls, virgins, below the age of 15. The widespread belief is that this sort of sexual intercourse will "clear" the infection. Obviously, those who were seropositive remain so. Those who were seronegative become positive more often than not due to the physical trauma (over and above the psychological one) associated with this sort of sexual intercourse. Scientific studies on these practices are difficult to be conducted. The men don’t want to be identified. The young girls are overwhelmed by shame and either prefer or are forced to remain silent. Domestic violence is another widespread social practice playing a role in the spread of HIV (Human Rights Watch 2003 c). Domestic violence does not just mean wife battering. It often means rape and other forms of abuse. Domestic violence is a worldwide problem, not just an African one. In many African countries, it is culturally sanctioned and traditionally accepted. It is not seen for what it is: a blatant violation of human rights. There are no specific laws protecting women from it. Its role in HIV spreading is often ignored. Uncontrolled urbanization
Poverty and lack of opportunities in rural areas lead to high rates of internal migration. According to the World Bank, the urban population in Sub Saharan Africa is growing at an average annual rate of 5.1 % with peaks of about and over 6 % in Burundi, Cape Verde, Gambia, Kenya, Mozambique and Niger, 7.7 % in Tanzania and 9.3 % in Malawi (World Bank 2002). This rapid urbanization process is due to high urban birth rates and sustained migration from rural to urban areas. It takes place in an environment unprepared for it. Poor housing, inadequate water supply and sanitation, insufficient and inadequate health and education services are a common feature of many African cities. The vast majority of rural migrants come to the towns jobless and remain so because of lack of jobs. They are absorbed in the so called informal economic sector made of petty jobs (Lankinen et al. 1994). The majority of them are young and unmarried. Those who are married often leave their spouses in the villages. The traditional family and social structures protecting individuals from marginalisation are becoming weaker and weaker even in rural areas. They are virtually non existent in urban areas. The urban environment is more permissive than the rural one. Initiating sex at younger ages, multiple sexual partners and alcohol abuse are frequent (Zulu 2000). Nowadays many young women migrate from rural to urban areas. Usually poorly educated and unskilled, they end up exchanging sex for money or in outward prostitution. All these factors facilitate the spread of HIV. Visits from the cities to the villages of origin are one of the mechanisms promoting the spread of HIV in the rural areas of Africa. Conflicts and civil wars
Poverty and lack of opportunities lead to huge numbers of young people without a job and without perspectives. They are the ideal cannon fodder needed to fight the countless conflicts that have bloodstained the Continent in the last decades. At least 20 of the 48 countries of Sub Saharan Africa are currently ravaged by civil war, on the verge of it or painfully trying to emerge from it. From the Second World War onwards, about 90 % of war victims are civilians. As it always happen, it is the weakest and most vulnerable, women and children, who pay the highest price. HIV prevalence is much higher among members of the army than among the civilian population: between 15 % and 30 % in Tanzania, between 40 % and 60 % in Angola and Congo, around 70 % in Malawi and 75 % in Zimbabwe (Foreman 2002). There are no statistics on the HIV prevalence among the many armed guerrilla groups. It seems reasonable to suppose that the situation must be similar to that of the official armies or, probably, worse. Soldiers, militiamen, guerrillas, are very mobile. They are often seropositive, they have a very active and promiscuous sexual life. Finally, they often "help themselves" to what they want by the use of force. Every war is accompanied by prostitution, rape and other forms of physical violence on women. It is evident how this can promote the spread of HIV. Edward Hooper, in his book "The river: a Journey Back to the source of HIV and AIDS" meticulously analyzes the circumstances that led to very high HIV incidence rates in the border region between Rakai District, in Uganda and Kagera Region, in Tanzania. That area was the theatre of the war fought by the two countries from October 1978 to April 1979. Hooper comes to the conclusion that it was this war, the army movements, the violence linked to them, that led to the high HIV incidence. His conclusions make a lot of sense. Situations similar to that of Kagera and Rakai back in 1978 and 1979 are present in at least 20 African countries today. Displaced and Refugees
Conflicts and war, among other calamities, also force millions of people to become either refugees or Internally Displaced People (IDP). Out of about 13 million refugees currently in the world, about three million are in Africa (Interaction 2003 a). Out of about 25 million IDPs worldwide, about 13 million are in Africa (Interaction 2003 b). Displacement, either outside or inside the country of origin, leads to overcrowding, breaking down of social cohesion mechanisms, promiscuity, destitution, desperation, stress, violence. All these factors promote the spread of HIV. The vicious cycle: poverty – AIDS – poverty
As it often happens in complex situations, causes and effects are so intimately linked to one another that they often exchange their roles. So, as it is true that poverty is a predisposing factor to HIV/AIDS, the opposite is equally true: HIV/AIDS favours and aggravates poverty. The impact of AIDS on national economies
About 92 % of people living with HIV and AIDS are adults, the economically productive part of the population (UNAIDS 2002). Mainly affecting the most productive members of society, AIDS threatens the economic survival of the worst hit countries. Countries with 20 % of their adult population seropositive are heading towards an annual 2.6 % decrease of their GDP (Gross Domestic Product) (UNAIDS 2003 a). Various attempts to model the economic impact of HIV/AIDS in poor countries reach the conclusion that it decreases per capita income in the range of 0.5 % to 1.8 % per person per year (OXFAM 2002). The most important mechanisms behind this are clear: decrease of the labour supply, decreased productivity due to mortality and morbidity, decreased exports and, most likely, increased health expenditures and increased imports. Several studies suggest that the AIDS pandemic already reduced the average national economic growth rates by 2 % to 4 % across the continent (Dixon et al 2001). According to some estimates, by 2010, the South African GDP per capita will be about 8 % smaller and the consumption per capita 12 % lower than what they would have been without AIDS (Arndt et al 2000). The World Bank made projections of the macroeconomic impact of HIV/AIDS for various African countries. According to them, the average growth rate of GDP between 1991 and 2015, because of HIV/AIDS, will be 1.5 % lower per year in Swaziland, 1.1 % lower in Namibia, 0.8 % lower in Lesotho (quoted in Dixon et al 2002). About 80% of the population of the majority of Sub Saharan countries depend on agriculture for their survival. HIV/AIDS is taking a heavy toll on farmers. This compromises the survival of entire communities. The Food and Agriculture Organization (FAO) estimates that about seven million agricultural workers have already died from AIDS in 25 Sub Saharan Africa since 1985 and about 16 million more could die from it in the next 20 years (quoted in UNAIDS/WHO 2002). About 14.4. million people need food aid in six countries severely hit by drought: Lesotho, Malawi, Mozambique, Swaziland, Zambia and Zimbabwe. In all these countries HIV prevalence rates in adult population exceed 10%, reaching 15 % in Malawi and 33% in Swaziland and Zimbabwe (UNAIDS/WHO 2002). HIV/AIDS is seriously compromising food security of millions of people. Of the 42 countries currently eligible for debt relief under the Highly Indebted Poor Countries (HIPC) Initiative, 34 are in Sub Saharan Africa. Already, 26 countries are benefiting from debt relief. Yet, this is far from sufficient. The Gambia, Mali, Niger and Zambia still spend more on debt servicing than in education. This proportion is more than twice in Cameroon, Mauritania and Sierra Leone. Even after debt relief in the framework of HIPC, Niger spends more in debt servicing than for public health. Sierra Leone spends 2.5 times more and Cameroon 1.6 times more in debt servicing than in public health (OXFAM 2002). HIV/AIDS, compromising the perspectives of economic development, makes the situation worse. It is a vicious cycle that must be broken by those who have the power to do so. As former South African President Nelson Mandela put it, at the International Aids Conference held in Durban in July 2001, "… [AIDS] is sweeping away what development there has been in the last decades and is sabotaging the future of Africa". The impact of AIDS on families: the orphans crisis
More than 11 million African children have lost one or both parents to AIDS (3.2 million of them are in South Africa). By 2010 this figure is projected at about 20 million only in Sub Saharan Africa (UNAIDS 2003, UNAIDS/UNICEF/USAID 2003). This would bring the total number of orphans in the region at about 40 million (UNAIDS/UNICEF 1999). In Botswana, Lesotho, Swaziland and Zimbabwe more than one in five children will be orphan by 2010 and 80 % because of AIDS (UNAIDS/UNICEF/USAID 2003). About 90 % of these orphans are taken care of by some form of "extended family". Social transformations and social breakdown due to persistent poverty, conflicts, wars, are eroding the extended family. HIV/AIDS has greatly contributed to this. For many families it is extremely difficult or, even, impossible, to take care of the children orphaned by AIDS. The reason is as simple as it is brutal: they are too many to be catered for. Many of the families where parents die of AIDS, especially if it is the mother, eventually break up. In many African countries it is not uncommon to come across families made of several children and one adult, the adult being a grand parent. The generation in between has been decimated. Grand parents are often impoverished. For simple demographic reasons, grand parents are unlikely to be there for the coming generation of AIDS orphans. At the other extreme we find families entirely made of children below the age of 15 (Foster et al 1997). These "anomalous" families are usually poor and vulnerable. The children inevitably drop out of school. If they manage to get some petty or temporary jobs, they are paid less than adults since they don’t have the same bargaining power. Millions of children grow up without the love and the guidance of parents and family. They are also denied education. Many of them end up in the town streets, live day by day, work and eat when they can, sniff glue or fuel. For girls child prostitution is the almost inevitable outcome. This growing number of dysfunctional young adults will add to the instability of already fragile societies. Another dramatic facet of the compound tragedy of AIDS and poverty. According to UNICEF, orphaning rates equal or higher than 5% exceed the capacity of extended families and communities to take care of the children. To take but one example, in Zambia 12 % of children are orphans because of AIDS (UNAIDS/UNICEF/USAID 2003). More than half of the countries in Sub Saharan Africa don’t have national plans to care for AIDS orphans. The burden of HIV /AIDS on health services
AIDS is today the main cause of death in Sub Saharan Africa, having overtaken older scourges such as Malaria. Caring for patients suffering from full blown AIDS or from opportunistic infections is a rapidly increasing burden for most African health systems. HIV infected patients occupy from 50 % to 80 % of beds in urban hospitals in Cote d’Ivoire, Zambia and Zimbabwe (World Bank 1999). HIV makes it more difficult to control other diseases like Sexually Transmitted Infections, Tuberculosis and even Malaria as it increases their incidence manifolds (Corbett et al. 2002). In Zambia, the incidence of Tuberculosis increased five times since the early nineties (OXFAM 2002). In the same country, the cost of treating one AIDS patient is estimated at about US $ 200 while the total health spending amounts to US $ 3 per person per year. It is further estimated that, by 2014, half of Zambia’s hospital beds will be taken by AIDS patients (OXFAM 2002). In South Africa, in 1999, 20 % of nursing students were estimated to be HIV positive (Bollinger et al 1999). In several African countries morbidity and mortality rates among health workers increased five to six times because of HIV/AIDS (UNAIDS 2003a). HIV AIDS worsens significantly the plight of already compromised health services by increasing demand and inflicting a heavy toll on the already grossly insufficient health manpower. The effect of HIV/AIDS on the education system
AIDS has devastating effects on demand and supply of education services. When a family member suffers from AIDS, the household income decreases and the expenses increase. Many households incur debts and / or sell family assets to meet the increasing medical costs. In such circumstances many children are forced out of school because the family cannot afford the school fees and the other costs associated with schooling (uniforms, transport, books, etc.). Lack of education adds up to the drama of children growing without a normal family and further compromises their future and the one of the societies they belong to. UNICEF estimated that it would cost about US $ 1.9 billion per year to ensure schooling to all African children (UNICEF 1999). It is overwhelmingly sad to see that, because of ignorance and indifference, the so called "world community" cannot come up with this amount, more or less equivalent to what is spent, annually, to buy play stations for the children in rich countries (Matshalaga et al 2002). With adult people dying in increasing numbers, birth rates are bound to drop. In the longer run, the number of primary school pupils will also drop. According to World Bank estimates, by 2010 AIDS will have reduced the number of children in school age by 12.2 % in Kenya, 13.8 % in Kenya, 20% in Zambia and 24% in Zimbabwe (World Bank 2000). As for the supply of school services, HIV/AIDFS is taking a heavy toll on school teachers. According to the World Bank, in the Central African Republic 85 % of teachers who died between 1996 and 1998 were HIV positive. On average, they died 10 years before they were due to retire. It is estimated that more than 30 % of teachers are seropositive in parts of Malawi and Uganda, 20% in Zambia and 12% in South Africa (World Bank 2003). There is no need to underline the long term catastrophic effects of undermining the education sector for the future of a country. Education is essential in the fight against HIV/AIDS and, in more general terms, in the fight against poverty (OXFAM 2002). The globalisation process is an unstoppable reality. High levels of education are an absolute need for individuals and whole nations not to be left at the periphery of it. Crippled education systems will worsen the marginalisation and deprivation of individuals, families and entire nations. HIV/AIDS and the African middle class
AIDS is much more of a burden for poor countries than for rich ones. Sub Saharan Africa, with about 10% of the world population, has about 66.5% of people living with HIV/AIDS. Within African countries, the less poor, the middle class, pay a very heavy price to the pandemic. Teachers, policemen, public officers, professionals in various fields, are among the most hardly hit. According to an article published by the New York Times in November 1998, a Rwandan pregnant woman has 9% probabilities of being HIV positive if her husband is a peasant, 22% if he is a soldier, 32% if he is a white collar worker and 38% if he is a government officer (McKinley 1998). Members of the middle class have relatively more money and are more mobile. When it comes to extra marital sex, middle class men have a far greater bargaining power. All in all, they have greater chances to get exposed to the infection with HIV. Ignorance and risky behaviour are not only fuelled by illiteracy. Being able to read and understand educational messages does not automatically mean changing behaviour. The seropositive rate among the adult population of Botswana exceeds 38%. Middle class members in the capital Gaborone joke about the meaning of the acronym AIDS: "American Initiative to Discourage Sex". In the Democratic Republic of Congo the french acronym for SIDA (the french for AIDS) is jokingly said to mean "Syndrome Imaginaire pour Dēscourager les Amoureux" (Imaginary Syndrome to Discourage Lovers). In Tanzania AIDS is "translated" in Kiswahili as "Acha Iniue Dogodogo Siachi" (Let it kill me, I won’t give up the young ones). These jokes often hide risky attitudes whose consequences are evident. If AIDS is increasingly a condition affecting mainly the poor, how does it come that the African middle class is so heavily affected? In our opinion this is only an apparent paradox. To start with, the bulk of the African middle class is only rich in relative terms. Rather than being rich, they are "less poor" than the destitute masses surrounding them and living in inhuman conditions of poverty. Income is only one of the many dimensions of poverty. The very fact of living and being part of a poor world, make it easier to be taken by its mechanisms. People don’t live in isolation from the communities of which they are members. Enjoying relative privileges in a poverty stricken environment does not protect from the hazards of that same environment. As much as personal income is an important determinant of health, the type of society one lives in is even more important (Marmot 2002). What is just said above should not obscure the fact that, in African countries, as well as in other countries, there is a minority of people who are very rich in absolute terms. If they become seropositive, they can afford antiretroviral drugs, a good diet and a good life. They can continue living, working and earning. The gap between them and the rest of society is increasing. African People Living with HIV/AIDS: too poor to be treated?
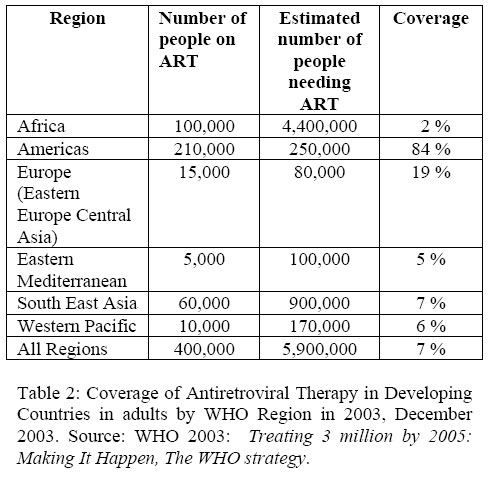
Since 1996, in rich countries, HIV/AIDS is no more a fatal disease. The advent of effective Antiretroviral Treatment (ART) transformed it into a chronic disease manageable although with some difficulties. The situation is very different in poor countries. Even at dramatically reduced price, the cost of ART is still far from being affordable to poor individuals and to entire health systems in poor countries. Perhaps too conservatively, WHO estimates that, at the end of 2003, about six million people, in poor countries, are in immediate need of ART (WHO 2003 a). Of them, only between 350.000 and 400.000 are actually getting the treatment and over 30 % of them live in Brazil alone. In Sub Saharan Africa about 50.000 people are currently receiving ART: about 1% of the estimated 4.1 million needing it (UNAIDS 2003). Table 2, below, gives an overview of the estimated needs and estimated coverage with ART in poor countries. For years, the sheer financial cost of ART (up to US $ 10.000 per person per year) kept it far out of reach of the bulk of those who needed it: the drugs were in the north of the world and those who needed them were in the south. Fashionable cost-effectiveness analysis concluded that treatment of AIDS patients with antiretroviral drugs was not "cost effective" therefore, not advisable (Creese et al 2002). The moral aspects of the question were obscured by the financial obstacles. This situation was somehow accepted by many as a fact of life. The fundamental injustice inherent to it was denounced by a number of people and organizations. Vocal campaigns to expand and insure access to drugs (especially but not only antiretroviral) were set up by various organizations at the national and international level (for instance, the Treatment Action Campaign [TAC] in South Africa, Médécins Sans Frontières, [MSF], International Action Treatment Campaign [IATC] etc.). In June 2001 the United Nations General Assembly Special Session on HIV/AIDS called on all the 189 Member States to " ... make every effort to provide progressively and in a sustainable manner, the highest attainable standard of treatment for HIV/AIDS, including the prevention and treatment of opportunistic infections and effective use of quality-controlled antiretroviral therapy" (United Nations 2001). It took time for such a declaration to start being taken seriously by individual governments and the so called international community. At the beginning of 2002, a number of powerful pharmaceutical industries took the South African government to court because of its declared intention of allowing the local production or the purchase on the international market of generic versions of antiretroviral drugs. This, according to the companies, violated their property rights. The popular pressure against the companies, nationally and internationally, grew stronger and stronger. On April 18th 2002 they abandoned the case. It was an important victory. But the South African Government did not take any immediate decisive action towards providing ART to those who needed it. Three months later the South African Constitutional Court, in a case concerning the provision of Nevirapine for Prevention of Mother To Child Transmission (PMTCT) ruled that this service was "protected by the State Constitution". It was in August 2003 that the South African Government announced its intention of providing ART to those who need it. It is currently estimated that between 400,000 and 500,000 people will fulfill the criteria to obtain ART in South Afica (a CD4 count less than 200 or an AIDS-defining illness. Probably, about 50.000 of them will ask for treatment in the first year. Much will depend on how quickly and easily the treatment will be available. On November 19th 2003 the South African Minister of Health, Manto Tshabalala-Msimang said that there will be one "anti-retroviral service point" in each of the 53 health districts in one year and one service point in each local municipality in five years. The government will not just provide antiretrovirals. In addition, thousands of new health workers will be employed (nurses, doctors, laboratory technicians, counsellors) and trained to make sure that ART, in all its aspects, is carried out safely, ethically and effectively. The whole process is estimated to cost about US $ 45 million for the next seven months and to increase rapidly up to about US $ 700 million per year by the fiscal year 2007-2008 (Baleta 2003). Notwithstanding efforts and progress by several countries to expand access to ART, its coverage in Sub Saharan Africa remains extremely low. But the attitudes are changing. In 2002, in a move very significant both technically and politically, WHO included ten antiretroviral drugs for treatment of AIDS in its Essential Medicines Model List. Nevirapine and Zidovudine were already in the list for prevention of mother to child transmission. To them, the following antiretroviral drugs were added: Abacavir, Didanosine, Efavirenz, Indinavir, Lamivudine, Lopinavir, Nelfinavir, Ritonavir, Saquinavir, Stavudine. In a press release, WHO declared that the inclusion of the above drugs in the Essential Medicines Model List " ... is based on a careful analysis of current evidence of ARV efficacy in developing countries, which shows that these medicines can be used effectively and safely in poor settings" (WHO 2002 b). The normative value of cost-effectiveness analysis in deciding who should have access to life prolonging treatment and who should not, is increasingly challenged. More and more, providing ART is seen not only as feasible but as necessary to fight the epidemic. Prices of ARV drugs are coming down quickly. In September 2003 the Clinton Foundation negotiated a substantial decrease in price with several major pharmaceutical companies. Now the lowest price is about US $ 132 for a full treatment per person per year. MSF started providing ARV drugs in 2001. Currently MSF is running 42 projects providing ART to about 9,000 people in 19 countries, 10 of them in Sub Saharan Africa (MSF 2003). MSF learned few lessons that were shared with WHO to elaborate the "3 by 5" initiative. The most important are:
Potential long term effect of ART
Making ART available and accessible to those who need it in Sub Saharan Africa still requires massive resources to be made available. The cost of providing ART is not just the price of the drugs (now as low as about US $ 150 per person per year for first line drugs). It also includes the resources needed to improve and strengthen the health systems supposed to distribute the drugs and regularly follow up the patients. Health systems in Sub Saharan Africa are not ready to deal effectively with ART. Massive investments will be needed to ensure that human resources are well trained and motivated, equipment for laboratory testing is available and functioning, the supply of drugs and reagents is constant. This will not be an easy task. And it will take time. But it is not impossible. Given the increasing awareness of the HIV/AIDS devastating effects and the growing public outcry against the blatant injustice of the current accessibility of ART, fighting this injustice could boost the thrust to strengthen African dilapidated health systems. If ART becomes widely accessible, one can expect HIV/AIDS, finally, to be treated more and more as any other communicable disease. Voluntary testing could become more popular, since a positive response would not any more be a death penalty. This would also help in decreasing the stigma still attached to HIV/AIDS. Ultimately, it could help to bring and keep the epidemic under control. Several authors argue that universal voluntary knowledge of one’s HIV serostatus is essential to ensure an effective response to the HIV/AIDS pandemic (De Cock et al 2003). According to WHO, by 2005, about 180 million people per year will need HIV testing (WHO 2003 c). If the case of Brazil is something to go by, these are not overoptimistic expectations. The Brazilian government started to make free ART universally available in 1996. It is estimated that, in the following six years, mortality rates decreased by between 40% and 70% and morbidity rates decreased by between 60 % and 80% (depending on the areas). In the same period, it is estimated that by providing universal ART the government spent US $ 1.8 billion and saved US $ 2.2. billions in hospital and ambulatory costs averted (WHO 2003 b). To these savings one should add the economic gains obtained by having people living and working normally. Individual and family lives not being disrupted, physical and psychological suffering being avoided, children not becoming orphans has an incalculable value. The case of Brazil also suggests that universal ART is possible also in a poor setting, with poor infrastructure. Epidemiological modelling studies suggest that, even in poor countries, ART could decrease incidence and, in a longer run, even prevalence of HIV. The beneficial effect of ART on the epidemic is directly proportional to its wide utilisation: the wider the use, the greater the impact on incidence and prevalence (Blower et al 2003). WHO is currently spearheading the so called "3 by 5" initiative, aiming at getting ART to at least three million people in poor countries by 2005. WHO sees the "3 by 5" as a comprehensive strategy including treatment, prevention, care and full social support for people affected by HIV/AIDS (WHO 2003 d). This strategy rotates around five Pillars:
WHO estimates that at least US $ 5.5 billion are needed by the end of 2005 for the "3 by 5" initiative to be successful. The situation in Uganda
The "success story" of Uganda in fighting HIV/AIDS is well known, documented and discussed (Asimwe-Okiror et al. 1997, Kilian et al. 1999, Mbulaiteye et al. 2002, etc.). The estimated prevalence of 6.2 % in the general population at the end of 2002, down from 30 % in 1992 (Ministry of Health, 2003), is a remarkable achievement. Sustained political commitment at the highest level and openness in the aggressive Information, Education and Communication campaign were the main factors that led to widespread behavioural changes (Hogle 2002). The Ugandan experience is almost universally hailed with very few "doubting Thomases" (Parkhurst 2002). It is currently estimated that about one million people live with HIV/AIDS in Uganda (Population Secretariat 2003, Uganda AIDS Commission 2003). According to the latest figure available, the cumulative number of Ugandans who died from AIDS was estimated at 947.552 in December 2001 (Uganda AIDS Commission 2003). The Joint Clinical Research Centre started distributing AZT in 1992 in the framework of a clinical trial. In 1998 Uganda started her participation in the Drug Access Initiative (DAI) funded, mainly, by UNAIDS. Four years later, a study concluded that ". . . AIDS patients in a developing country can be managed successfully with antiretroviral therapy" (Weidle et al 2002). The study, however, was carried out in Kampala and the Authors themselves recognised that major challenges are to be faced when expanding ART in areas with worse infrastructure, less equipment, poorer patients and poorer overall settings. Today, about 100.000 people are estimated to be in need of ART in Uganda but only about 17.000 are getting it. The majority of them pay out of their pocket. A few are catered for, totally or in part, by their employers. Employers paying for ART of their workforce seems not only to be "just". It seems to be convenient as well. Dr. Apollo Kaggwa, of Bank of Uganda (BOU), recently declared that, in the last few years, his institution used to lose about 20 employees to AIDS each year. This carried enormous replacement costs. Since BOU started paying up to 90% of the price of ARV drugs, less than five people are lost to AIDS every year and absenteeism for illness also decreased dramatically (The New Vision, December 2nd 2003). Although more scientific studies are needed to document this aspect, increased productivity after the introduction and funding of ART by employers has been reported from Botswana, Brazil, South Africa and elsewhere. According to the Uganda National Health Policy "Primary Health Care shall remain the basic philosophy and strategy for national health development" (Ministry of Health 1999). In line with this statement, ART is now envisaged as one of the strategies to control HIV/AIDS. A Policy for the provision and monitoring of ART is still at draft stage and plans to operationalise it are also being drafted. So far, 29 centres have been accredited to deliver ART, 14 belong to the government, 15 are private (five Private Non for Profit, five Private for Profit). The current price of antiretroviral drugs in Uganda is about US $ 180 per person per year (about US $ 50 cents per person per day). This price is low, but, as already said, the actual cost of providing ART is much higher. It is also necessary to underline that this relatively low price only concerns first line drugs. Second and third line drugs, to be used when resistance This notwithstanding, the government aims at achieving universal accessibility of ART in a phased manner. There is increasing national and international momentum towards making ART widely available and Uganda’s success in controlling HIV/AIDS, should ensure widespread international financial support. The challenges are many. They are difficult but not impossible to overcome. Conclusion
HIV/AIDS affects the life of millions of people and their families. According to WHO it is the greatest health crisis facing the world today (WHO 2003). Poor countries are more severely hit than rich ones and Sub Saharan African countries are the worse hit. Almost without exceptions, diseases are more of a social and economic problem than a mere medical one. For no disease this seems truer than for HIV/AIDS. Poverty and HIV/AIDS are tightly linked in a vicious cycle whereby one leads to the other in a downward spiral that is deadly for individuals, societies and entire countries. The fight against HIV/AIDS can only be effective within a Comprehensive Primary Health Care approach. Social justice and equity are at the basis of this fight. Combating HIV/AIDS can only be done by combating poverty. Not providing treatment to the millions who need it just because they cannot afford it is morally unacceptable by any possible standard. But providing treatment will not be enough to win the fight. As we have tried to suggest in the previous pages, HIV/AIDS has its root causes in global poverty and injustice. It does not make much sense to tackle HIV/AIDS without tackling its underlying and basic causes. Enormous amounts of human, financial and material resources are wasted to fight wars (about US $ 800 billion per year; one billion US $ per week for the war in Iraq ...). As many studies suggest, winning the war against HIV/AIDS and poverty would cost much less. So far the impact of HIV/AIDS on all aspects of life and all sectors of society, especially in poor countries, has been devastating. If the response to this crisis will be just more of the same, the worst has still to come. True, resources to combat HIV/AIDS increased in recent years, even if they are still very far from what is needed. The resources are not lacking. What seem to be lacking is vision, political will and genuine concern for human beings - all human beings. References
|

{kind=link}
{kind=link}