 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
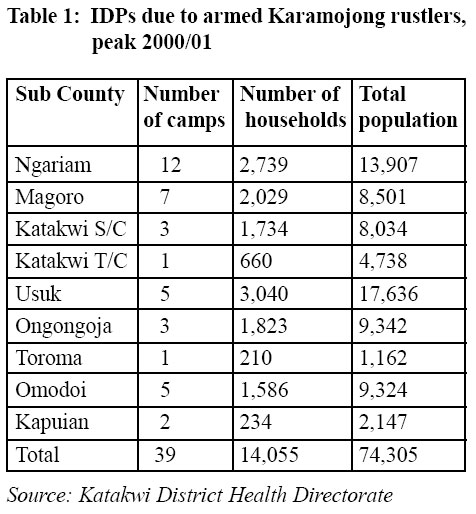
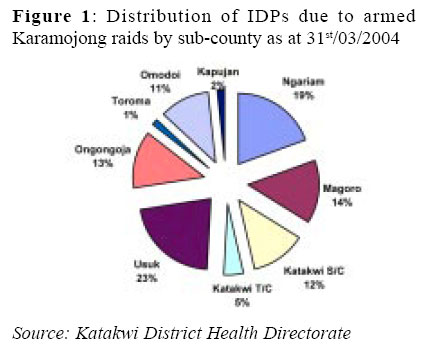
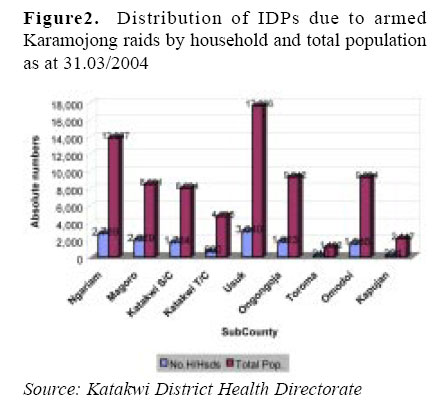
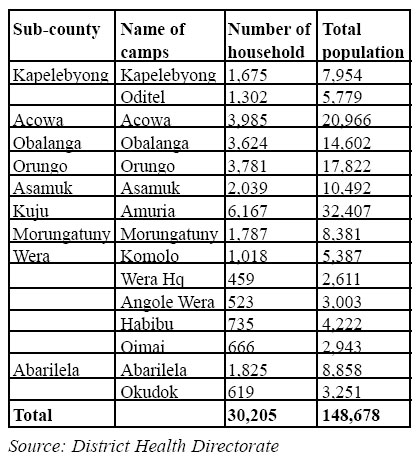
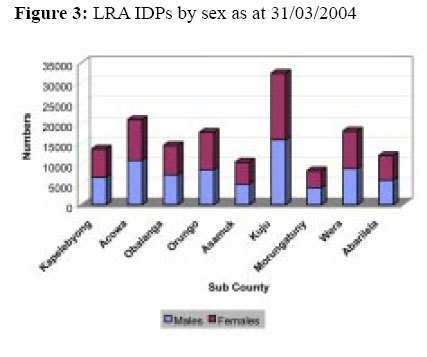
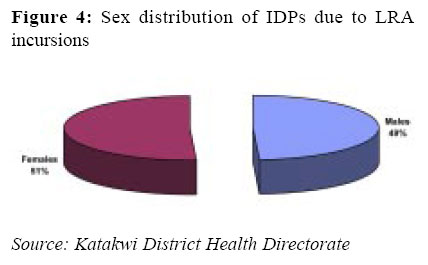
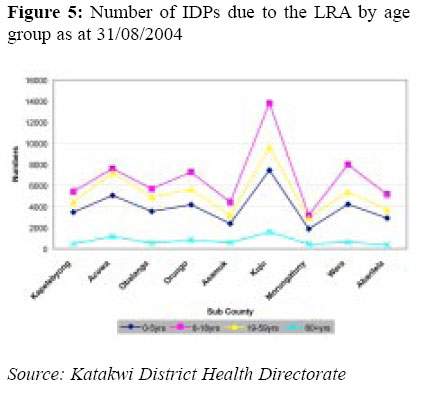
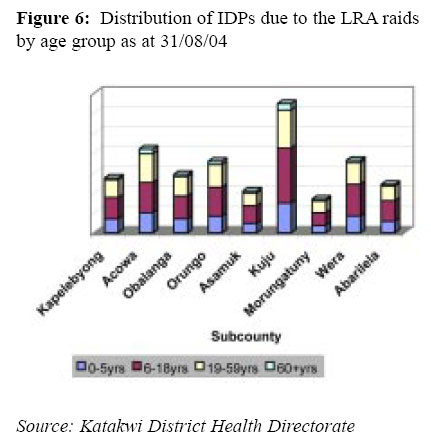
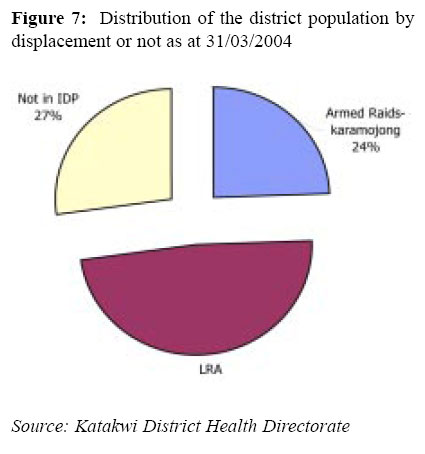
Health Policy and Development Journal, Vol. 2, No. 2, Aug, 2004, pp. 90-95 DELIVERING HEALTH CARE TO IDPS: EXPERIENCES AND CHALLENGES IN KATAKWI DISTRICT Onyige T. A. Katakwi District Code Number: hp04017 Abstract There are two broad categories of IDPs in Katakwi district by cause; those displaced by the Karamojong rustlers and those displaced by the Lords Resistance Army (LRA) incursion. Sporadic Karamajong raids started over 50 yrs ago and they are still ongoing to date. By 2001 there were an estimated 75,846 persons from 17,660 households living in 48 IDP camps, mainly in areas bordering Karamoja. Incursions by the LRA started around the 16th June 2003 and lasted till April/May 2004. Rebels of the Lord's Resistance Army invaded the district from Obalanga Sub County and within two weeks, the pillage had spread to 9 other sub counties, mainly in the Counties of Kapelebyong and Amuria. This paper gives a bird's eye view on the extent of displacement in Katakwi, the health status of the IDPs and proposals for improved service delivery. Introduction Katakwi district was established in 1997 and is located in the northeastern part of Uganda. It shares borders with the districts of Soroti, Kumi, Moroto, Kotido, Lira, and Kaberamaido. It is composed of 3 counties of Amuria, Usuk and Kapelebyong. It has 18 subcounties plus a Town Council, 93 parishes and 664 Local Council ones (LC1s). The district has got three Health Sub Districts, namely Usuk HSD, Amuria HSD and Kapelebyong HSD. In the 2002 population census, the total District population was 307,302, distributed as follows; 123,215 in Usuk HSD, 122,086 in Amuria HSD and 61,731 in Kapelebyong HSD. (UBOS, 2003.) There are two broad categories of IDPs in Katakwi district by cause; those displaced by the Karimojong rustlers and those displaced by the Lords Resistance Army (LRA) incursion. (Katakwi Local Government, 2004). Karimojong rustlers Sporadic Karamojong raids started over 50 years ago and they are still ongoing to date. By 2001 there were an estimated 75,846 persons from 17,660 households (1/3 of the district population then) living in 48 IDP camps, mainly in areas bordering Karamoja in the Health Sub-District catchment areas of Kapelebyong and Usuk. The displacements as a result of the Karamojong raids by Sub-county are shown in table 1 below: The proportions of those displaced by the Karamojong raids by sub-county are further presented in figure 1 below: The sub-counties of Usuk and Ngariam were the worst affected by the Karamojong cattle rustlers. Below is a further illustration of the extent of the displacement again showing that Usuk and Ngariam were the worst affected. (Figure 2) LRA incursions Incursions by the LRA started around the 16th June 2003 and lasted till April/May 2004. Rebels of the Lord’s Resistance Army invaded the district from Obalanga Sub country and within two weeks, the pillage had spread to 9 other sub-counties, mainly in the counties of Kapelebyong and Amuria. These incursions led to massive displacements as is shown below: (table) The sub-county of Kuju was the worst affected followed by Acowa. The displacements were in equal proportions, males and females as is shown in figures 3 and 4 below: An analysis of the ages of the displaced was further carried out and the results are presented in figure 5 and figure 6 below: Overall, the elderly (60 + yrs) were the least and teenagers and middle ages the most. This definitely has implications on the type of health services that have to be planned for. Lastly, figure 7 below shows the distribution of the district population by displacement or not as at 31/3/ 04. As is shown, the effect of the LRA incursion into Katakwi has been the most disastrous, far overshadowing the chronic armed Karamojong raids. The health of IDPs
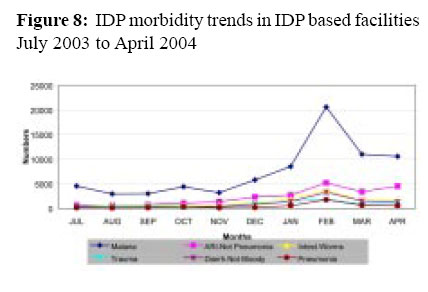
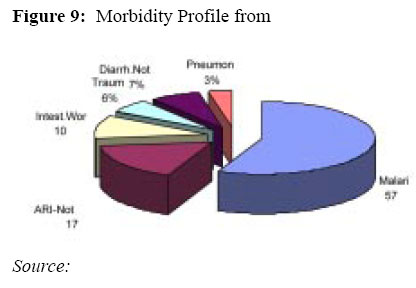
Morbidity profile 2003/04 The reported number of cases of the leading causes of morbidity in the IDP based facilities from July 2003 to April 2004 are presented below: As figure 8 clearly shows, the reported number o cases of malaria increased greatly during the months of December 2003 to March 2004 and so did the reported numbers of the other diseases. Again figure 9 below shows that malaria was the leading health problem in the IDP camps from July 2003 to April 2004 followed by acute respiratory infections that are not pneumonia. Other selected health indicators
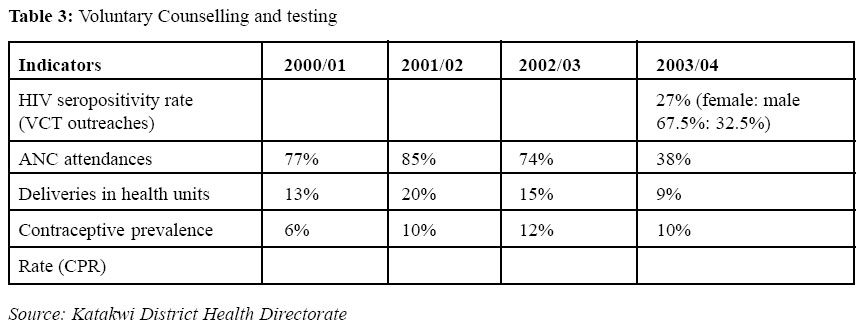
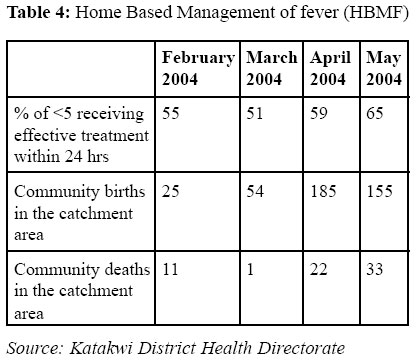
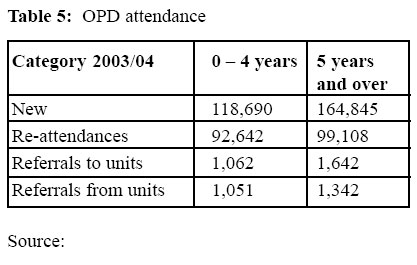
Table 3 below further shows some selected indicators, HIV/AIDS and maternal health indicators. In 2003/04 during the LRA incursion, the HIV seropositivity rate greatly increased and the number of ANC attendances decreased together with the number of deliveries in health units and CPR. Table 4 shows some recent statistics on home-based management of fever (HBMF). The percentage number of children under 5 years receiving effective treatment within 24 hours has steadily been increasing however community deaths in the catchment areas have also been increasing. Lastly, table 5 shows OPD attendance figures during the period of insurgency. Challenges about IDPs
Health services delivery amongst IDPs is very challenging. In Katakwi, provision of basic curative services particularly maternal and child health care is very challenging especially to populations that are distant from health facilities. The district health services have however continued to provide emergency referral services in the identified health facilities security allowing and the presence of landmines and sniper fire. Health workers have also endeavoured to provide routine immunization and other health preventive services in those health facilities within IDPs camps, emphasising hygiene and sanitation. With all these efforts, challenges still exist. First and foremost, getting and convincing the few accessible medical staff to go to the camp units to provide the above services is difficult. Secondly close linking up with other active partners n health service delivery in order to optimise the available resources for service delivery so as to provide comprehensive services amongst IDPs has been difficult. Attempts have been made to hold coordination meetings and also to share information but in vain. Further, currently in the camps in Katakwi, there is wide spread unhealthy social behaviour i.e. alcoholism, promiscuity and apathy. These have posed a serious challenge and will further be problematic during the transition period and there after. The question of how to organize and offer services in the transition period between camp life and resettlement has not yet been seriously addressed. In Katakwi, some IDPs re returning to their homes and these also have to be catered for. Lastly there is the issue of mobility of IDP populations according to the state of security in the district, especially as the Karimojong problem has been long standing and might not be about to end. How do district health services accommodate this in their dayto-day work? District Partners
The major partners that have been involved in organizing and delivering health services for the IDPs in Katakwi include the Ministries of Health; Finance and Defence. Development partners include WHO, UNICEF; UNFPA; MSF; OXFAM; ACTIONAID [U]; RERDCROSS; MEDAIR; MEDICALID [U]; CCF; AIM and UPHOLD. Indigenous NGOs such as HEALTHNEED [U]; SOCADIDO; AIC; COU and YWAM have also been active in Katakwi. There are also 22 CBOs and also private individuals. However all these partners have various areas of focus. Strategies for improved service delivery
The district health service team plans to ensure timely procurement of drugs, sundries and medical equipment based on needs. There will be liaison with other active partners in the provision of Primary Health Care outreach services to communities in the three Health Sub Districts. There are however fewer partners engaged in curative services. Active awareness creation among the community and promoting their participation in health programmes will be encouraged through IEC and their direct involvement in voluntary community based service delivery e.g. the Community Own Resource Persons (CORPs). Sensitisation meetings and the commemoration of National Health Days will be encouraged. There will be improvement in HMIS and in the utilization of service data generated timely with special focus on IDPs in order to facilitate lobbying, planning, supervision and monitoring. The district will engage in capacity building, recruitment and training of staff and the communities in liaison with partners. Emphasis will also be put in strengthening support supervision at all district levels through supervisory teams. Lastly continued wide lobbying for funds and other support essential for health service delivery and infrastructure development (health unit construction and procurement of transport) for easing access to the remote service areas will actively be pursued. Conclusion
There are formidable but not insurmountable constraints and challenges. Staffing problems will cause a major challenge together with sustaining timely supplies of drugs and sundries. Ensuring sustained community involvement, ownership and concern for their health is another challenge and this will be very vital in order to ensure the sustainability of intervention. Uncertainties about timely reception of funds for activity implementation have always been in existence but in such a situation of need they pose a real challenge. Conditional ties for some donor funds with no flexibility at all in the utilization of these funds leaves health workers with their hands tied. Occasional political interference, especially at times of allocation of resources is also sometimes a hindrance to effective service delivery. Bureaucracy especially in tendering processes is a big problem. Uncoordinated supervisory visits by central/donor supervisors wastes time and remove health workers from their routine duties. Lastly, maintaining staff working in areas of conflict and Internally Displaced Persons camps is not going to be easy. A number of recommendations can be made based on the experiences. The current staffing gaps should be filled with qualified health workers and means of giving these health workers incentives to work in hostile environments need to be explored. There should be an increase in effective partnerships and coordination of government service providers with GO and meetings for information sharing should be encouraged. Provision user-friendly yet robust means of telecommunication and transport are now more vital than ever. Its effective services are to deliver and coordinate. Devising sustainable and timely funding mechanisms and also procurement and distribution of drugs and sundries very important. Lastly, there should be an increase of community own resources persons (COR). References
Copyright 2004 - Department of Health Sciences of Uganda Martyrs University The following images related to this document are available:Photo images[hp04017t2.jpg] [hp04017f6.jpg] [hp04017f9.jpg] [hp04017f1.jpg] [hp04017f7.jpg] [hp04017f8.jpg] [hp04017f4.jpg] [hp04017t4.jpg] [hp04017t5.jpg] [hp04017f2.jpg] [hp04017t1.jpg] [hp04017f3.jpg] [hp04017f5.jpg] [hp04017t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}