 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 2, No. 2, Aug, 2004, pp. 85-89 THEME ONE: Coping with armed conflict PLANNING HEALTH CARE FOR INTERNALLY DISPLACED PERSONS: EXPERIENCES IN UGANDA Okware Samuel, Bwire Godfrey, Ogwang Ogwal Peter, Ministry of Health Code Number: hp04018 Abstract
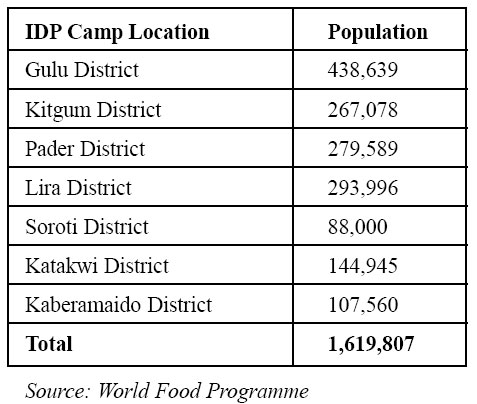
A significant proportion of Ugandans have at one time or another been forced to flee their homes. In 1997 alone, point prevalence revealed that 2,000,000 persons were displaced and it is estimated that currently about 1.6 million Ugandan are internally displaced. The ten districts in the north and northeastern Uganda have the biggest problems of displacement with Gulu district having the highest number of IDPs. The status of IDPs is unpredictable. The objective of health care services for IDPs is to reduce excess mortality (currently twice that of districts without IDPs) and morbidity among the Internally Displaced Persons through interventions that target the most vulnerable (women, children, disabled) in these communities. The natural response in Uganda for the affected districts in the North and North- Eastern parts of the country has been multisectoral. This paper proposes how priority health interventions can be designed and delivered in IDP camps, above all stressing the role of coordination. Introduction Status of IDPs in Uganda as of April 2004
Internally Displaced Persons (IDPs) are people who The status of IDPs as of April 2004 is presented above: have been forced to flee or leave their homes or places of habitual residence as a result of or in order to avoid the effects armed conflict, situations of generalized violence, violations of human rights, natural or manmade disasters, and have not crossed an internationally recognized state border (GOU, 2003). A significant proportion of Ugandans have at one time or another been forced to flee their homes. From 1979 to date, civil conflicts and cattle rustling have affected cumulative about 7,000,000 persons. This cumulative number is increasing with time. In the southwest, the Allied Democratic Forces (ADF) displaced 150,000 persons and in 1997, 300,000 people were displaced in Katakwi. In 1997 alone, point prevalence revealed that 2,000,000 persons were displaced. The western part of Uganda is currently free from displacement, however the ten districts in the north and northeastern Uganda have the biggest problems of displacement. Status of IDPs in Uganda as of April 2004 The status of IDPs as of April 2004 is presented above: (Table) Gulu district, as is shown in the table above, has the highest number of IDPs. Other districts include Apac, Kumi and Adjumani, however the figures in these districts could not be ascertained. The status of IDPs is unpredictable. Below is a map of Uganda showing the districts with recent IDPs. (Figure) IDP health care services The objective of health care services for IDPs is to reduce excess morality (currently twice that of districts without IDPs) and morbidity among the Internally Displaced Persons through interventions that target the most vulnerable (women, children, disabled) in these communities. The natural response in Uganda for the affected districts in the North and Northeastern parts of the country has been multisectoral. This paper will only be limited to the health sector interventions. The priority areas in health care services for IDPs re below: Coordination
This has been a major area of concern attracting many stakeholders. Coordination has been streamlined through a number of processes. The overall coordination at central level is by the Office of the Prime Minister. UN-OCHA is responsible for multilateral coordination and their office is the Chair of bilateral organizations involved with IDPs. The Ministry of Health heads the National Task Force overseeing health carer service delivery and it reports to the Office of the Prime Minister. This Task Force is charged with developing comprehensive national plans and also making appeals for assistance. Other key sectors include the Department of Water Development (DWD), Ministry of education and Sports, Ministry of Defence, Ministry of Agriculture, Ministry of Finance and the Ministry of Local Government, Ministry of local Government and Ministry of Culture and Gender. At the district level, the District Disaster Management Committee of which the Chairman Local Council 5 or Chief Administrative Officer (CAO) is the Chairman and the District Director of Health Services (DDHS) the secretary is responsible for coordination of IDPs activities. This committee has representation from other key sectors in the district such as Department of Education, Department of Water Development, Department of Culture and Gender, Internal Affairs (Police) and Defence. This Committee reports to the Office of the Prime Minister and the DDHS reports to the Ministry of Health. The committee manages all interventions at the district level. Initial assessment
Initial assessment is key for decision makers and technical staff in identification, planning and implementation of priority interventions. This involves rapid collection and analysis of data within few days on; the background of displacement; the affected population; major health problems; information on the environment; the required resources (persons and material) and the operating development partners. The first rapid assessment (within 3 days) gives data/ information on whether or not to intervene. The second phase (1-3 weeks) gives quantitative and qualitative data for proper planning of interventions. Measles immunization
In our experience, measles is a major cause of childhood mortality in displaced populations. However, this can be prevented through mass immunization and Vitamin A supplementation of all children aged 6 months to 15 months. Displacement, overcrowding and poor hygiene in camps are all factors that encourage the emergency of serious epidemics. Mass immunizations should always be done within the first week and it should be followed by integration into routine immunization. Vaccination coverage of 100% in the target population should be aimed at. Control of communicable diseases and treatment of common diseases/conditions. Over 75% of top ten diseases responsible for morbidity and mortality re preventable through basic interventions. A. Control of communicable diseases Malaria, diarrhoea, Acute Respiratory Infections and measles account for 50-95% all reported mortality and morbidity in displaced populations. Other communicable diseases include meningococcal meningitis, hepatitis, typhoid fever, typhus etc. The interventions aim at reducing excess morbidity and mortality these diseases through prevention and control of epidemics. Control measures involve good surveillance; improving the environment and living conditions of IDPs; good epidemic preparedness is the key to prevention and control of these diseases. Health teams must be ready to respond to epidemics through vaccination of the vulnerable groups; early treatment of the cases (personnel, drugs, protocols, health facilities) and each outbreak requires a response specific to the disease (meningitis and measles vaccination). B. Public Health Surveillance IDPs are vulnerable to serious outbreaks of communicable diseases. Surveillance systems provide early warning of epidemics by determining the main health problems and by guiding interventions. The data collected should be simple and limited to 5 categories i.e. demography, mortality, morbidity, basic needs and data on interventions. During the emergency phase, crude mortality rate is the most useful indicator as it measures the magnitude of the problem. Morbidity data should cover common diseases that are major cause of deaths or have epidemic potential. And lastly, data should be analysed and communicated to decision makers by means of weekly reports during emergency phase. C. Case Management Case management is vital to reduce mortality early during displacement. Major interventions such as provision of water, food and shelter are very useful in reduction of mortality and morbidity; however, they cannot be implemented very fast. Health care interventions can be implemente4d quickly with the aim of reducing excess mortality and morbidity among the IDPs by ensuring appropriate medical care and response to epidemics. Health care services should fulfil the following: provide curative treatment for priority communicable diseases (malaria, acute respiratory infections, diarrhoea, sexually transmitted infections, HIV/AIDS, worms, emergency obstetric care, etc); reduce the suffering from other debilitating diseases; have capacity to carry out active surveillance and cope with high demand of curative services; provide easy access to other levels of health care (referral, peripheral facilities, outreaches/home visiting); should have basic supplies and equipment (drugs, guidelines, laboratory etc) and lastly they should provide Home Based Care (Homapak, First Aid kit and Mama Kits). Home based Care is very useful in this type of situation. This approach is based on community participation in Health Care delivery. In each village or a camp a number of community persons who are chosen and trained to provide simple treatment against common illnesses. Each such person (called Community Health Care worker) is assigned between 50-100 households nearest to his home. In a camp there are several trained Community Health care Workers depending on the size of the camp or village population. The sum total of these workers in the camp or village form what is called “Village Health Team”. Each village health team member serves between 250-500 population most of whom may actually be related and is provided with the following: A First Aid Kit and A Safe Child Birth Delivery kit. It is important that drugs are made available through special measures suitable for emergency situation. The Ministry of Health put in place additional specific actions to increase drugs in the 17 affected districts in Northern and North-eastern Uganda: The revision of district allocations to include IDPs as a variable besides population; and a Ministry of Health circular to the districts that would make re-allocation of district Poverty Alleviation Funds easier and more flexible for emergency use. Additional resources are available to support these districts (Teso, Lango, and Acholi) under the SPECIAL NEEDS PROJECT by Danish International Development Agency (DANIDA) which opened up essential credit lines with the National Medical Stores and Joint Medical Store for regional hospitals, district hospitals, Health Sub Districts to increase the drug supply to the affected districts. There is also a special emergency supply from Ministry of Health, World Health Organisation (WHO), and United Nations Children Education Fund (UNICEF), United Nations Family Planning Association (UNFPA etc. usually provided on request Water and sanitation
Water is critical in IDPs both in quantity and quality. Communicable diseases, such as diarrhoea, resulting from lack of water and poor environmental sanitation are a major cause of morbidity and mortality in displaced populations. During the emergency phase, priority should be given to the provision of sufficient quantities of water (1520 litres per person per day) and one hand pump for 500 – 750 persons. The quality of the supplied water should be improved as soon as possible le to contain less than 10 fecal coliforms/100 ml and this should not affect the quantity supplied. Excreta disposal facilities and general hygiene should initially be one latrine/50 – 100 persons, but later it should be onelatrine/20 persons. Lastly health education on basic hygiene should be conducted. In addition, measures to control vectors (flies, mosquitoes, fleas etc) and solid waste and disposal of the dead should be instituted. The health sector has to work with Department of Water Development to achieve all this. Food and nutrition
Food adequacy has been a major challenge in the IDPs camps especially for children, pregnant women, the sick and disabled. Provision of food is the responsibility of the districts working with the Office of the Prime Minister, however, the risks of nutritional problems are more in IDPs than others and thus the nutritional intervention by health sector is very important. The aim of the nutrition intervention is to reduce the high mortality and morbidity related to malnutrition. Nutritional surveys should therefore always be part of the initial assessment. The nutrition status of children aged less than 5-years is used as an indicator (global acute malnutrition rate of 5% should act as a warning). A minimum daily food ration of 2,100 Kcal/person should be ensured for all. (This is equivalent to 400 grams of cereals and 150 grams of pulses (beans) per person per day). The following factors aggravate malnutrition and call for higher levels of nutritional intervention; a Crude Mortality Rate of more than 1/10,000 pop/day; epidemics of measles, shigella, or any other communicable disease. Nutrition intervention (selective nutrition targeting the vulnerable) involves; therapeutic feeding programmes to treat the severely malnourished; targeted supplementary feeding programmes to prevent malnutrition in vulnerable groups (under 5 yrs, pregnant women, lactating mothers and medical cases). Shelter and site planning
During the initial phase shelter is a big challenge. Provision of shelter is also the responsibility of the local district and the communities working with the Office of the Prime Minister; however, health sector involvement is key during site planning and improvement. Site planning and improvement should be done early to minimise overcrowding and also to allow for efficient service delivery. The site plan must ensure: security, access to water, provision of adequate space (30m2/person/house), and must be free from environmental risks. Small sites are preferred, however consideration of culture and social patterns is important. Provision of materials for temporary shelter is a priority early after displacement. However later the communities should be encouraged to use the local material (grass, reeds, papyrus, etc). A gap of 75 metres should be provided for every 300 metres to prevent fire hazard. Human resource and training
Adequate staff and training is required to respond to demands of the various interventions mentioned above. It is important to provide human resources capable of performing the different tasks involved in health interventions with the overall goal of effective and coordinated implementation of the top 10 priorities. Recruitment, management and training of personnel are essential. Standard staff policy must be defined in line with Ministry of Health and Ministry of Public Service. Several trainings may be necessary and must be preceded by a Training Needs assessment. Conclusion
The first major challenge is the persistent insecurity and the greatly dynamic population movements, which makes provision of health care very difficult. The insecurity results in widespread destruction of health infrastructure, which inevitably disrupts service delivery. Improving access through mobile outreach services in such an environment is very challenging. Coordination of field partners especially Non-Government Organizations (NGOs) is so far providing problematic as some of them do not want to fully disclose their plans and activities. Mainstreaming the disaster management policy into sectors, district and communities remains a difficult task, which demand cooperation from all the key sectors. Another challenge is the sustainability of IDPs interventions (resources, manpower, supplies etc). Social mobilization and dialogue need to be intensified by all the stakeholders working with and amongst the IDPs and lastly an exist strategy to rehabilitate IDPs, communities and the districts needs to be formulated at this state. References
Copyright 2004 - Department of Health Sciences of Uganda Martyrs University |

{kind=link}
{kind=link}