 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 2, No. 2, Aug, 2004, pp. 112-121 MALARIA AND DDT: MYTHS AND FACTS Maurizio Murru, Department of Health Sciences, Uganda Martyrs University Code Number: hp04021 Abstract Around the world, about 2,400 million people, in about 100 countries and territories, are still at risk of contracting malaria. Between 300 and 500 million of them get the disease each year and between 1.1 and 2.7 million die from it. In Uganda, malaria is the first cause of morbidity and mortality. It accounts for 29%-50% of all out-patients consultations, 30% of inpatients admissions and 9%-14% of inpatient deaths. Up to 23% of deaths in children under five years of age are due to malaria. The Uganda Minister of Health recently announced the intention of using DDT for Indoor Residual Spraying to decrease malaria morbidity and mortality. This spurred a heated debate. The available scientific evidence, accumulated over the years, strongly suggests that DDT, when properly used, is harmless to human beings. The attempt to control malaria, without DDT, is futile. This paper advocates an evidence based approach, free from preconceived ideas. Politicians should help to inform and sensitise public opinion, rather than spread false information harmful for public health. Introduction
Malaria has been with us for more than 4,000 years but was recognised as a disease about 2,500 years ago. The word, "malaria" is a combination of two Italian words "malaria", literally meaning "bad air". This name was given to the disease sometimes during the XVIII century because people associated it to the foul air found near the marshy areas. Much later, in France, malaria was called "paludisme", still implying a link with marshy areas (the French word for "marsh" is "palud"). Scientific knowledge about the vectors, the causal agents, their transmission and life cycle, started to be developed towards the end of the XIX century by the French Charles Louis Laveran, the Italians Golgi, Marchiafava and Bignami and by the British Ronald Ross (Bruce-Chwatt, 1985). A combination of factors, mainly Indoor Residual Spraying (IRS) with DDT, improved living conditions, sustained environmental interventions, urbanization, industrialization and availability of drugs, led to the disappearance of the disease from most of the rich countries in North America and Europe, in Taiwan and Jamaica, and to its effective control in Algeria, Egypt, Lybia, Morocco, Tunisia, Mauritius, Singapore, Hong Kong and parts of Malaysia, India and Sri Lanka. But malaria prevalence persisted in the rest of the developing world. Thus, the goal of global malaria eradication, adopted by the 8th World Health Assembly in 1955, proved to be optimistic. It was replaced, about two decades later, by the goal to control malaria. The current malaria situation
Today, about 2,400 million people, in about 100 countries and territories, are still at risk of contracting malaria. Between 300 and 500 million of them get the disease each year and between 1.1 and 2.7 million die from it. Sub Saharan Africa (SSA) bears about 90% of the global burden of malaria morbidity and mortality. About 1 million of those who die from malaria are children below five years of age. About 25% of the child mortality in SSA is due to malaria. This means a stunning average of about 3,000 African children dying of malaria, every single day (WHO, 2000 I, UNICEF, 2004). It is estimated that malaria costs Africa between US$ 10 and 12 billion in lost GDP growth (UNICEF 2004). According to the "Africa Malaria Report 2003, between 25% and 40% of all outpatients visits and between 20% and 50% of all hospital admissions, in SSA, are due to malaria. Yet, it is estimated that only about 40% of the total malaria morbidity and mortality is seen in the formal health sector (WHO-UNICEF, 2003). Malaria in Uganda
Malaria is the first cause of morbidity and mortality in Uganda. According to the Ministry of Health (MOH), it accounts for 29%-50% of all outpatients consultations, 30% of inpatients admissions and 9%14% of inpatient deaths. Up to 23% of deaths in children under five are due to malaria (MOH 2003). Malaria epidemics have occurred in several Ugandan districts. The Uganda Malaria Control Programme is based on four main intervention strategies:
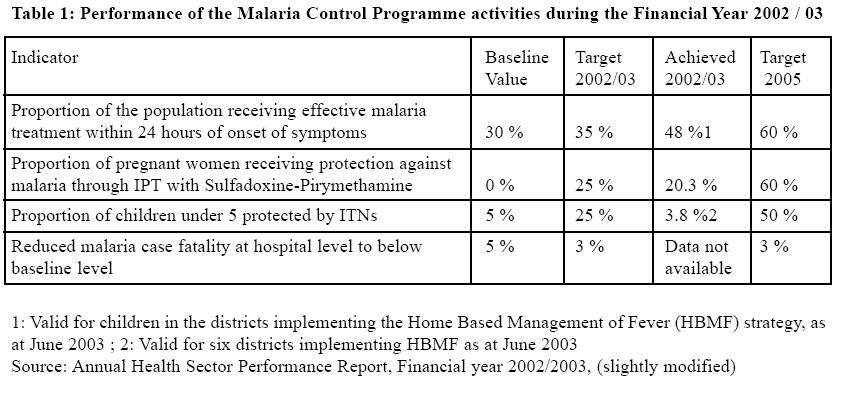
In 2002, the Home Based Management of Fever (HBMF) strategy started in 30 districts and is currently at different stages of implementations in different districts. Preliminary evaluation results suggest high levels of community satisfaction and decreased levels of under five morbidity and mortality reported in Health Units (MOH, 2003, Mwesezi, 2003). Table 1, below, shows the performance of the Malaria Control Programme during the Financial Year 2002/ 2003. Roll Back Malaria (RBM)
The RBM initiative was born out of the consideration that malaria, as a health problem, was not receiving the due attention. The fact that it was (and is) mainly a problem of poor people in poor countries, had a lot to do with this neglect. RBM was jointly launched, in 1998, as a global partnership, by WHO, UNICEF, UNDP and the World Bank with the stated goal of halving the world's malaria burden by 2010. This ambitious goal was endorsed, two years later, on April 15th 2000, by several African Heads of State in Abuja, Nigeria. The main interventions promoted in the framework of RBM are:
The set of measures needed to control malaria would require at least US$ 1 billion per year. Currently, the available funds don't exceed US$ 200 million per year. In 1998, when RBM was launched, the funds allocated to malaria control, worldwide, were a mere US$ 60 million. The Abuja Declaration On April 25th 2000, high ranking representatives of 44 out of the 50 African Countries affected by malaria, met in the Nigerian capital Abuja for the "African Summit on Roll Back Malaria". At the end of the summit, they adopted a common declaration in which they committed themselves and their governments to: Initiate appropriate and sustainable action to strengthen the health systems to ensure that by the year 2005:
They also called upon the Development Partners "… to cancel in full the debt of poor and heavily indebted countries in order to release resources for poverty alleviating programmes, such as Roll Back Malaria and to allocate substantial new resources of at least US$ 1 billion per year to Roll Back Malaria" (Roll Back Malaria / WHO, 2003). This is the highest political endorsement of the global fight against malaria so far. Unfortunately, the year 2005 is very near and the targets set in Abuja are still very far. Is Roll Back Malaria a failure?
Since the launch of RBM, the world malaria situation has not improved. It has worsened. The "Africa Malaria Report 2003" recognises it by stating, in a rather muted style that "Roll Back Malaria is acting against a background of increasing malaria burden." The same Report adds that "…It is possible that the start of intensified control efforts coincided with increasing malaria mortality, meaning that - without them - the situation might have been substantially worse than is now reported" (WHO-UNICEF 2003). In an editorial published by The British Medical Journal on May 8th 2004, Gavin Yamey puts it much more bluntly: "Roll Back Malaria is currently a failing health initiative" (Yamey 2004 I). Apart from the global estimates on malaria morbidity and mortality, already mentioned, other figures suggest failure. Only about 15% of young children, in SSA, sleep under a bed net and only about 2% sleep under an impregnated bed net (WHO-UNICEF 2003). Household surveys carried out in 28 SSA countries suggest that only about 42% of children under 5 years of age receive an anti-malarial when they needed it. About 80% of them receive Chloroquine alone (which is largely ineffective). In addition they receive it long after 24 hours from the onset of fever (WHO-UNICEF 2003). Malaria during pregnancy is estimated to cause between 75,000 and 200,000 infant deaths each year, mainly due to low birth weight (Steketee 2001). Yet, less than 5% of pregnant women, in SSA, have access to effective malaria treatment and control measures. Demographic and Health Surveys carried out in a few SSA countries suggest that about 10% of pregnant women sleep under a bed net. The coverage with ITN is at a much lower 3% (WHO-UNICEF 2003). About 110 million Africans live in areas at high risk of malaria epidemics. In recent years, disastrous malaria epidemics were reported from Botswana, Mozambique, South Africa, Zambia, and Zimbabwe. Statistical assumptions suggest that about 110,000 people die every year, in SSA, during malaria epidemics (as part of a total malaria death toll estimated between 1 and 2.7 million people). The current knowledge about surveillance systems in the majority of SSA countries makes it reasonable to believe that we are still far from achieving it. On the bases of these facts, it is tempting to agree with the BMJ editorial. Clearly, renewed efforts are needed. More must be done
Two issues, very important in combating malaria, hit the headlines in recent months. One concerns effective malaria treatment. Effective drugs are available but, because of their cost, they are not accessible to those who need them. Artemisinin-based Combination Therapy (ACT) offers an effective alternative to the now ineffective drugs still widely used simply because of their low cost (like Chloroquine and, although to a lesser extent, Sulfadoxine-Pyrimethamine). ACTs are cheap in absolute terms but expensive when compared to old (and largely ineffective) anti-malarial. What is more important, they are far too expensive for poor people in poor countries. The average price for the full treatment of malaria of an adult outpatient is US$ 0.13 with Chloroquine, US$ 0.14 with Sulfadoxine-Pyrimethamine, US$ 0.20 with Amodiaquine and US$ 1 - 3 with ACTs (WHO-UNICEF 2003). It must be noted that the reported price of Artemisinins reflects only the production costs, without anything added to recover research and development (R&D) costs. This is because ACTs related research and development costs were, globally, mainly borne by the public sector (Institute of Medicine, 2004). The current world production capacity of ACTs is at around 30 million of annual treatments. The needs are likely to be almost ten times bigger. Satisfying these needs will require up to US$ 500 million per year (Yamey, 2004 II; Institute of Medicine, 2004). Currently, only six African countries have started using ACTs: Burundi, Mozambique, Senegal, South Africa, Zambia and Zanzibar. In addition, nine more African countries introduced the use of ACT in their malaria treatment policy: Benin, Cameroon, Comoros, Gabon, Ghana, Equatorial Guinea, Kenya, Sao Tomé and Principe and the United Republic of Tanzania (WHO 2004) Human rights activists and NGOs, around the world, mobilised themselves to push down the prices of antiretroviral drugs to treat AIDS. They didn't do the same to push down the prices of ACTs. At a meeting organised in New York by the Columbia University School of Public Health, in May this year, Professor Jeffrey Sachs, Director of Columbia University Earth Institute, said that "Donors have never taken malaria seriously. One to three million [malaria] deaths per year is a mass neglect" (Yamey 2004 II). However, something seems to be moving on this front with attention being drawn to the problem. In January 2004 the Lancet published a Viewpoint fiercely critical of WHO and GFATM (Global Fund against Aids, Tuberculosis and Malaria) attitudes and stand on the issue of anti-malarial drugs (Attaran et al. 2004). The debate reached a wider audience than the "scientific community" since the BBC discussed the Lancet article in a report with a provocative title: "WHO is failing malaria patients" (BBC 2004). In it, WHO and GFATM were accused, by various experts interviewed, to be still pushing for the use of cheap but ineffective antimalarials instead of fighting for the wider availability of ACTs. As a matter of fact, WHO has been advocating wider availability of ACTs for some time now (WHO 2003). But, as the Lancet article points out, "WHO violates its own policy standard regularly". WHO and GFATM officers replied to the accusations and the debate goes on. What matters here, is the fact that the problem of long term accessibility to effective anti-malarials is, although slowly, gaining attention. The second measure to combat malaria, we want to refer to, is the use of DDT (Dichlorodyphenil Trichloroethane) for IRS. This gained even more attention, around the world and, in the last few months, also in Uganda. The DDT debate in Uganda
On April 15th 2004, at a press conference, the Uganda Minister of Health stated the intention of his Ministry to resume Indoor Residual Spraying (IRS) with DDT to combat malaria. Just stating this intention, stirred a very heated debate on newspapers, FM radios, Universities and schools. The National Environment Management Authority (NEMA) asked the Ministry of Health (MOH) to carry out an Environmental Impact Assessment of the proposed use of DDT. It also asked for wide consultations on the idea and for a thorough consideration of all the alternatives (Wendo, 2004). The majority of the reactions to the Minister proposal were fiercely negative. More often than not, the debate was more emotional than rational. It was based more on preconceived (baseless) ideas than on scientifically proven facts. Scientific evidence is very much in support of the Minister's stated idea. On August 10th the Social services Committee of the Uganda Parliament approved the MOH proposal to use DDT for IRS in malaria control. Now it is up to the Ministry to produce a detailed plan on how it intends to proceed. DDT DDT was first synthesised in 1854. Its insecticidal properties were discovered much later, in 1939, by the Swiss Paul Muller. DDT was used for the first time, for indoor spraying of walls, in Naples, Italy, in 1944. Since then, for at least two decades, it was widely used to control malaria, around the world, with stunningly successful results. Insecticide Residual Spraying (IRS) with DDT was never used a single measure in malaria control. Other measures, like prompt treatment with effective drugs, environmental changes, health education, were essential components of the control strategies mainly coordinated by WHO. Many African countries, still under colonial rule, were not part of the campaign. They lacked structures and expertise and, even more important, the colonial authorities did not make the needed efforts to develop them. Malaria disappeared from most of North America and Europe and its incidence and prevalence fell dramatically in the Mediterranean Basin, in the Middle East, in the Far East and in those few countries in Southern Africa who, almost autonomously, set up eradication campaigns (South Africa, Swaziland, Rhodesia). The successful campaigns against malaria conducted between the 1940s and the 1960s, DDT was not the only weapon. But it was an extremely effective and important one. The abandonment of the use of DDT has been cited as one of the major reasons for the resurgence of malaria mainly in Africa and Latin America (Roberts 1997, Mouchet, 1998). Some authors go as far as stating that: "Although many factors contribute to increasing malaria, the strongest correlation is with decreasing numbers of houses sprayed with DDT" (Roberts, 2000). Unlearned Lessons
Recent history also teaches us something. Or, at least, it should. All malaria endemic countries that stopped the use of DDT for IRS, saw disastrous increases in malaria morbidity and mortality almost immediately afterwards. Those that resumed the use of DDT, like Madagascar, South Africa, Sri Lanka, Swaziland, saw equally dramatic falls in malaria morbidity and mortality afterwards. In particular, Madagascar, after suspending the use of DDT, experienced a dramatic malaria epidemic between 1986 and 1988: more than 100,000 people died. The government decided to resume indoor spraying with DDT. Malaria incidence declined by more than 90%, after just two spraying cycles (Mouchet 1998). In the Unguja and Pemba islands (Zanzibar) a successful IRS campaign with DDT was carried out between 1958 and 1968. The population of the main vector, Anopheles Funestus, was brought down to undetectable levels. The prevalence of Plasmodium Falciparum parasites in the blood of infants was reduced to less than 5% (Delfini 1969). No ITN programme in endemic areas has ever achieved such low levels of parasitemia so far (Curtis et al. 2000). After the suspension of the IRS programme, Zanzibar saw malaria going back to holoendemic levels. There are many other similar examples of lessons not learned because they were not reflected upon with a mind free from preconceived ideas. DDT toxicity for human beings
Over the years, various claims have been made about DDT toxicity for human beings. The substance has been linked to increased incidence of some forms of breast, liver, or pancreas cancer. None of these links has been proven (Garabrant et al. 1992, Key et al. 1994, Schecter et al. 1997). Professor Len Ritter, Executive Director of the Canadian Network of Toxicology Centers, headed a panel of scientists researching on the relationship between pesticides and cancer. In its report (Ritter, 1997) he rules out any relationship between DDT and cancer and any harmful effect of DDT as a disrupter of the human immune system, of the blood level of several hormones and as a cause of birth defects. Acute poisoning with DDT is also a remote possibility. The eminent British scientist and environmentalist Kenneth Mellanby, in his book "The DDT Story" (Mellanby, 1992), writes "I myself, when lecturing about DDT during the years immediately after World War II, frequently consumed a substantial pinch of DDT, to the consternation of the audience, but with no apparent harm to myself, either then or during the next 40 years". DDT has been used and misused in huge amounts around the world. Numerous studies and experiments have been done to find out its potential negative effects on human beings. If such harmful effects were there, by now, they would be known. As a commentary titled "How toxic is DDT" (published by the Lancet on July 22nd 2000) puts it " … the safety record [of DDT] for human beings is extremely good". Millions, probably billions of people have been exposed to DDT either because of their work or because they lived in houses or environments were it was sprayed. To date, there isn't one single peer reviewed, independently replicated, scientific study providing evidence of links between DDT and negative consequences for human health (Attaran et al. 2000). True, traces of DDT were found in human breast milk. But the same authors that pointed this out, had to admit the "… lack of any detectable effect on children's health" (Waliszewski et al. 1996). In 1999, over 380 scientists, from 57 countries, wrote an open letter to UNEP (United Nations Environmental Programme) supporting the use of DDT for IRS for malaria control. Among them there were three Nobel laureates in medicine. UNEP is engaged in negotiations and discussions for the global ban of DDT. The demise of DDT and its main causes
If DDT is so effective (and it is), if its toxicity, when correctly used for IRS, is non existent (and it is), if it is so cheap (and it is), why is it that only mentioning it raises fierce and heated reactions and strong opposition? DDT is very stable in the environment (where it can last for up to 15 years and more ), it can enter the food chain and it can damage animal and plants. Over the years, DDT has been grossly misused. Not for malaria control activities, but to protect cotton and other crops from all sorts of pests. The use of DDT in agriculture involved the dumping of massive quantities of it in the environment. No serious precautions were taken and no adequate safety measures were adopted. When scientists and public opinion woke up to realize the extent of this misuse, it was too late. DDT became one of the first widely popularised examples of the evils linked to the dangerous human tendency to "play God with nature". It became an ugly icon, a repugnant symbol of the human arrogance and disrespect for nature. In 1962, Rachel Carson published a book entitled "Silent Spring". In it, she denounced the detrimental results of DDT accumulation in the environment due to the dumping of enormous quantities of it on towns and fields. The book had an enormous impact on the public opinion. According to a widely circulated article recently published by the New York Times, "Few books have done more to change the world" (Rosenberg, 2004). The book is still revered. In 2002, a special "40th anniversary edition" of it was published to stress its continuing importance and influence. Pressure from environmentalists and from the public mounted and, in 1972, DDT was banned in the United States. Shortly after it was banned in Canada. By the end of the 1970s, it was banned in many West European countries too. By then, these countries had not seen a malaria case for a long time (apart from some imported ones). Yet, the use of DDT was suspended even in countries where malaria was and still is a major public health problem. The agricultural use of DDT was inconsiderate and harmful. The use of DDT for IRS against malaria was life saving and harmless to human health. Unfortunately, and unwisely, the ban hit all possible uses of DDT. Disastrous consequences of an illogical ban
In a blatant example of a very harmful "cultural hoax", the environmental fundamentalists of the rich world succeeded in disqualifying DDT in the eyes of the public opinion in poor as well as in rich countries. Facts are distorted. Situations are twisted around. Today, donor countries and major donor agencies are very reluctant to provide funds for the purchase and use of DDT for malaria control. Yet, the quantities of DDT involved in IRS are minimal (2 grams for 1 square meter of wall surface every six months). Well studied and clear procedure for storage, distribution and use, can make it impossible for the substance to reach the environment. Contrary to its reputation, as bad as it is undeserved, DDT has many virtues. We already discussed its effectiveness in killing mosquitoes and its lack of proven detrimental effects on human health. Another virtue is its low cost. The patent for it expired many years ago and its production costs are very low. Among the various insecticides that can be used for IRS in controlling malaria, DDT is the cheapest one: about 20%-30% cheaper than the Pyrethroids (the next cheapest alternative) and much cheaper than all the others (Hanson et al., 2004, WHO, 1995). In addition, it is more effective. The weak arguments against DDT.
We have already mentioned the supposed harmful effects on human health. This argument doesn't stand. Another argument is that several strains of mosquitoes are resistant to DDT. In fact, the agricultural use of DDT led to the appearance of the first strains of Anopheles Mosquitoes resistant to it in the mid 1960s. In Africa, resistance was detected in West Africa and in Egypt (Roberts 2000). Massive use and misuse of an insecticide is a powerful mechanism for the appearance of resistance to it. After many years of non use, the situation is likely to be different. In any case, even if there are some strains of mosquitoes resistant to DDT in some parts of the Continent, why shouldn't we use it were resistance is not there (including Uganda)? Many of its opponents say that the use of DDT is pushed by multinationals firms producing it. The opposite is true. Multinationals are not interested in a wide scale revival of the cheap DDT. They are against it. It is much more convenient, for them, to produce and sell less effective and much more expensive alternatives. A question is often asked. Why should poor countries use a substance that is banned in rich countries? Rich countries don't use DDT because of the reasons we have seen before and, mainly, for an even simpler reason: they don't need it. They don't have malaria any more. The "cultural hoax" against DDT is multifaceted. Donor countries and donor agencies don't want to be associated to DDT in the eyes of public opinion. Therefore, they don't provide funds for its production, purchase, distribution and use. There are very few exceptions. For instance, Eritrea is using DDT for IRS with money coming from the World Bank. A project envisaging the use of DDT for IRS in Somalia is in its final phases of negotiations and funds should come from the GFATM. GFATM is also funding some projects using DDT in other African countries like Zambia. Few other African countries are using DDT for IRS in controlling malaria: Ethiopia, Madagascar, South Africa. They are doing it, mainly, using government funds (Hanson et al., 2004). The RBM does not recommend the use of DDT, although WHO acknowledges its usefulness in several documents. The Africa Malaria Report 2003 does not even mention DDT. The shyness with which this substance is treated is well exemplified in this Report. A Table, at page 47, (Table 5.1) shows four historical examples of serious malaria epidemics. Among them, reference is made to the malaria epidemic that struck Madagascar between 1986 and 1988, to which we referred elsewhere in this paper. The cause for this epidemic is reported as "Abandonment of IRS and shortage of antimalarials". DDT is not mentioned and there is no mention of the dramatic improvements brought about by the resumption of IRS with DDT in Madagascar. The Stockholm Convention on Persistent Organic Pollutants
The Stockholm Convention is a global treaty aimed at protecting human health ant the environment from the negative effects of a group of substances called Persistent Organic Pollutants (POPs). POPs are organic compounds that can resist biodegradation and can persist in the environment for long periods of time (up to ten years or more). They can enter the human food chain and they can accumulate in the fat tissues. DDT is a POP. The Convention was written in 2001 and entered into force on May 17th 2004. It bans the production and use of POPs. With the notable exception of DDT, whose production and use are allowed "… for disease vector control according to the WHO guidelines" (UNEP 2001). The DDT exception incorporated in the Stockholm Convention should make the DDT opponents think harder before jumping to their vocal and unsubstantiated conclusions. The official position of WHO
In front of the persistent and heated debate on the use of DDT for malaria vector control, WHO clarified its official position in a two page document WHO position on DDT use in disease vector control under the Stockholm Convention on Persistent Organic Pollutants (WHO, 2004 II). In this document, the world leading organization on health matters reiterates its support for the continued use of DDT for disease vector control. It also warns against any premature shift from DDT to "less effective or most costly" alternatives. Such a move would be unsustainable and would increase the disease burden in the malaria endemic countries. As we have already seen, the premature abandonment of DDT already led to an increased disease burden in poor countries. IRS with DDT
WHO defines Indoor Residual Spraying as " … the application of a liquid insecticide with long lasting residual properties which dries to form a crystalline deposit on the sprayed surface A lethal dose of the insecticide is absorbed by insects that come into contact with the surface. The insecticide is applied to the indoor resting places of the vectors" (WHO, 2000 -II-, WHO, 2004 III). Complex problems, like malaria, don't have simple solutions. Magic bullets don't exist and DDT is not a magic bullet. Including DDT, there are 12 insecticides that can be used for IRS in malaria control. Of all of them, DDT is the most effective, the one whose effective action lasts longer and it is the cheapest one. It is useful to add that advocating the use of DDT for IRS doesn't mean advocating its use blindly and mindlessly as many opponents to this control strategy superficially imply. Well known criteria exist to decide when, where and why to use DDT for IRS (Najera et al. 2002). In addition, IRS with DDT must be carried out following precise guidelines and safety procedures that are clearly described by, among others, the WHO itself (WHO, 2000 II). DDT should be used for IRS only in areas infested by Anopheles mosquitoes that bite and rest indoor (not all Anopheles species do) and that are not resistant to it. The susceptibility of mosquitoes to DDT should be carefully studied and monitored along time. IRS with DDT must be carried out following well known safety procedures by well trained personnel. DDT must be stored, transported and used in ways that prevent its release in the environment both accidental and/or intentional (for uses other than IRS for vector control). A clear regulatory system must be in place for DDT purchase and use and it must be effectively enforced. The success of IRS with DDT, as the one of all public health measures, depend on its wide coverage. In turn, this depends on its understanding and acceptance by the concerned communities. Households can reject house spraying for a series of reasons. Misunderstandings and false information spread by a detrimental propaganda are important and effective reasons. There are others. DDT kills mosquitoes and other insects. It doesn't kill bedbugs. It can make them more active. DDT leaves a whitish deposit on walls and can leave, for some time, an unpleasant odour. When compared with children deaths, these do not seem major problems. They did not hinder the enormous successes obtained with DDT in the past. They don't hinder the good results currently obtained where IRS with DDT is used. They don't: if the right information is given and understood. Information, education and communication campaigns are of utmost importance. In this respect, the collaboration of well informed and responsible politicians and civil society organizations is essential. An ill conceived and misinformed propaganda against a possible campaign of IRS with DDT could have disastrous consequences and it could lead to the campaign failure. This would not only mean a waste of scarce resources. Immensely more important, it would mean a missed opportunity of saving lives. All these aspects are essential and all must be carefully considered. This may be difficult in many circumstances. In a decentralised setting (like the Ugandan one) it may require additional efforts. Conclusions
It is about time we forget myths and face facts. Hundred of thousands of children are dying while precious time and energies are wasted in discussions that often ignore very well known scientific evidence. It is about time that serious decisions are taken, rooted on rational, evidence based, considerations rather than on weak and baseless emotions or blind preconceived ideas. It is about time for politicians and intellectuals to take the hard path of educating the public opinion rather than taking the easy path of following it in search of cheap and quick popularity. It is about time for all those concerned to start working seriously to develop appropriate national policies, procedures, guidelines, for the introduction of IRS with DDT to control malaria, for its adequate monitoring, for its careful evaluation. There are no simple solutions to complex problems. Magic bullets don't exist. DDT is not one. DDT will not eradicate malaria in Africa (or in Uganda). Nobody is saying this. DDT can significantly help to reduce malaria morbidity and mortality, together with other necessary measures like availability, accessibility and correct use of effective drugs, availability, accessibility and correct use of impregnated bed nets, environmental modifications, health education and other measures. Open minds, correct information, strong analysis, sound reflections and committed political will are what is needed. Now. References
Copyright 2004 - Department of Health Sciences of Uganda Martyrs University |

{kind=link}