 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 2, No. 2, Aug, 2004, pp. 105-111 THEME TWO: DDT and malaria IS DDT SAFE? CONSIDERING ITS USE FOR MALARIA CONTROL IN UGANDARichard Tren1, Jasson Urbach1, Jennifer Zambone2 and Roger Bate2. 1 Africa Fighting Malaria, Sandton, South Africa. 2 Africa Fighting Malaria, Washington DC, United States. Code Number: hp04022 The insecticide DDT has been very successfully used for many years in malaria control programmes around the world. We assess the validity of the allegations that DDT is harmful to human health and the environment and find that they lack credibility. This is particularly true when one considers the way in which DDT is used in malaria control and the risks that people face from malaria. Indoor Residual Spraying programmes can be sustained for many decades and have been shown to have a considerable impact on malaria morbidity and mortality. However any country considering using DDT or any other insecticide in an Indoor Residual Spraying programme to control malaria should ensure that the right regulatory mechanisms are in place and that the programme is well controlled with scientific and medical oversight. IntroductionMalaria is the leading cause of death among children in Africa and causes catastrophic harm to the continent's development, even though it is a preventable and curable disease. The World Health Organisation (WHO) estimates that the disease claims over 1 million lives every year. Approximately 93% of Uganda's population is at risk from malaria, and according to the Centres for Disease Control (CDC) the incidence of the disease has increased from approximately 5 million cases in 1997 to 16.5 million in 2003. In malarial countries, the disease is estimated to reduce per capita economic growth by 1.3% per year (Gallup and Sachs 2000). Thus, controlling malaria is important not only because of the human misery the disease causes, but also due to its economic burden, which creates further human misery. One of the most effective ways of controlling malaria is the targeted use of residual insecticides. When sprayed on the inside walls of dwellings, these insecticides kill the adult Anopheles mosquito that transmits the malaria parasite. Indoor Residual Spraying (IRS) programmes eradicated malaria from Europe and North America and dramatically reduced malaria in many other parts of the world. One of the most effective insecticides for IRS programmes is dichlorodiphenyltrichloroethane, or DDT. The Ugandan Ministry of Health has announced that it is preparing to introduce DDT into IRS programmes, and Members of Parliament have asked the Ugandan government to secure funds for DDT procurement (Nangulo 2004). Malaria control programmes have at their disposal a range of interventions, and no one intervention should exclude any other. DDT is only one insecticide that IRS programmes can use. In turn, IRS is only one way to control the malaria vector, the Anopheles mosquito. Successful malaria control programmes use evidence based decision making to determine the best possible range of interventions under the specific conditions that face different regions. Successful malaria control programmes in southern Africa have shown IRS, and more specifically IRS using DDT, to be an essential element. This success had caused other African countries to either re-introduce DDT to malaria control or to consider seriously the move. Given that DDT, when used properly as part of a well managed IRS programme, is highly effective at controlling malaria and is safe for humans and the environment, this move should be welcomed. Yet DDT is a controversial insecticide, and many fears and misunderstandings exist surrounding its use in malaria control. This paper attempts to address some of those fears and improve the understanding of DDT use in malaria control, which we hope will lead to better malaria control and healthier people. DDT use in public health programmes
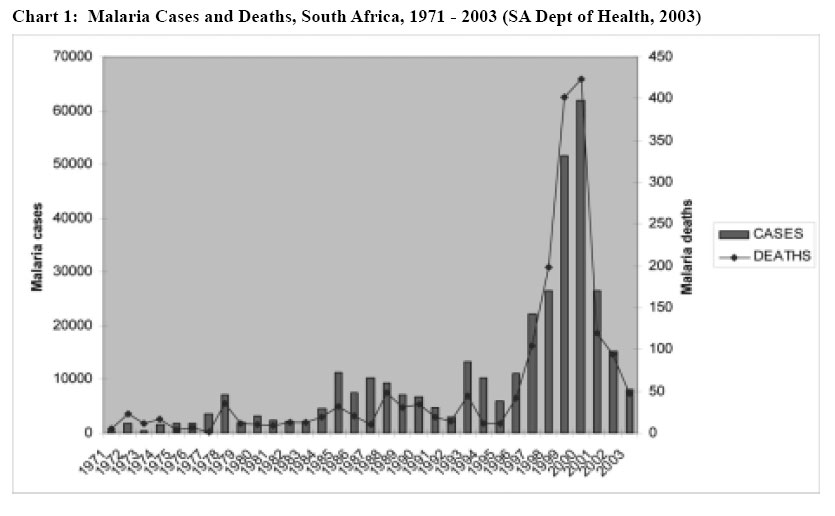
The Allied Forces first used DDT during the Second World War to control the vector borne diseases typhus, dusting civilians and troops with DDT powder, which was highly effective at killing the body lice that transmitted the disease. Scientists soon noted that because of its ease of application and long lasting residual action, DDT would be useful in controlling another vector borne disease, malaria. When it is used in malaria control, sprayers apply small amounts of DDT, usually 2g of active ingredient per square meter, on the inside walls of houses and in some cases under the eaves of houses. Because of its long lasting action - up to 1 year - DDT vastly improved malaria control, as previously shorter acting insecticides had to be applied to dwellings every 1 to 2 weeks. DDT works in three ways; it is acutely toxic to the Anopheles mosquitoes and therefore very effective at killing them; it also acts to repel mosquitoes so that they may never enter a dwelling in the first place; lastly it acts as an irritant which may cause mosquitoes to exit a dwelling without biting. With DDT, malaria control officers had within their grasp a tool that could potentially eradicate malaria. After the Second World War, Southern European countries were the first to attempt IRS programmes using DDT. Within a few short years DDT spraying had eradicated malaria from Europe. The United States government adopted DDT spraying soon after the war, and its use successfully eradicated malaria in 1952. Chile eradicated malaria as did several island states in the Caribbean in the early 1950s. In 1946 South Africa adopted DDT in its malaria control programme and within a few years had reduced the number of cases to just 10% of those reported in 1942/43 (SA Dept of Health, 1997). In 1951, India's malaria control programme began to use DDT and managed to reduce malaria cases from an estimated 75 million per annum to just 50 000 per annum (Harrison 1978:243). In 1955, based on the success of DDT spraying around the world, the WHO launched its malaria eradication programme. The overriding opinion at the time was that a short period of intense DDT spraying could reduce malaria cases to such a degree that eradication would be a possibility. This was not to be however, and for a number of reasons the WHO called off the eradication programme in 1972. In some countries the development of insecticide resistance meant DDT was ineffective. In other areas climatic conditions favourable for mosquito breeding meant the malaria vector bred faster than they could be eradicated. In some countries, such as India, operational problems and a lack of scientific oversight beset the programmes. Yet despite these problems, many countries maintained carefully controlled DDT spraying programmes and were rewarded with low and declining malaria cases. Soon after World War II, agriculture widely adopted DDT and this led to widespread environmental contamination. However as the public health use of DDT involves the targeted spraying of tiny amounts of insecticide inside houses, there can be no comparison between the agricultural use of DDT, which gave it its bad name, and the public health use of DDT. In this regard Roberts et al estimate that treating a 4km2 cotton field - which is the size of a single farm in some locations - takes as much DDT as all the high-risk houses in a tropical country the size of Guyana would take. (Guyana has an area of 214 969 sq km, about the size of Great Britain) (Roberts et al. 1997). South Africa maintained its IRS programme using DDT from 1946 to 1996. In 1996 the Department of Health replaced DDT with synthetic pyrethroid insecticides. As DDT is best sprayed on traditional mud structures, and an increasing number of houses in rural malarial areas are made in the western style with plastered and painted walls, the government was correct to attempt to introduce alternative insecticides. However, largely because agriculture uses synthetic pyrethroid insecticides, insecticide resistance soon became a problem. A highly efficient malaria vector, Anopheles funestus, believed to have been eradicated in the 1970s, soon reappeared in South Africa (Hargreaves et al. 2002). What followed was one of the worst malaria epidemics in the country's history. Malaria cases rose from around 6000 in 1995 to over 60 000 in 2000 (SA Dept of Health 2003). In early 2000, South Africa reintroduced DDT to malaria control in KwaZulu Natal Province, the province worst hit by the epidemic. In 2001, South Africa further introduced new artemesinin-based combination therapies to treat malaria patients. The combination of effective insecticides and drugs ensured that malaria cases fell by almost 80% by the end of 2001. In 2000 a privately funded IRS programme in the Zambian Copperbelt Province began using DDT in its IRS programme. The DDT spraying was solely responsible for 50% decline in malaria cases after just 1 spraying season (Sharp et al, 2002). The success of this programme continues and has influenced national malaria control policy such that other parts of Zambia have implemented DDT IRS programmes. Other southern African countries that have successfully used DDT to control malaria include Swaziland, Namibia, Zimbabwe and Madagascar. These countries ensure that well structured, vertical malaria control programmes use DDT, programmes that have good scientific oversight and control and monitor the use of the chemical. These factors, which in fact should be in place for the use of any insecticide in IRS, are an important pre-requisite for a DDT IRS programme. IRS is the single most important malaria control intervention in most southern African countries. DDT in turn is one of the most effective and important of the range of different insecticides that are used in IRS. Those countries in southern Africa that have successfully controlled malaria use IRS and largely rely on DDT. The insecticide is incontrovertibly responsible for saving millions of lives. Yet fears persist that DDT is harmful to human health and the environment and that its use in malaria control will somehow threaten agricultural exports. An oft cited argument against IRS in general is that it is unsustainable and therefore should not be entertained as a policy option. These concerns are dealt with in turn. (Chart 1) DDT and Human Health
DDT and its effects on human health have been a highly contentious issue since at least the 1950s. Those that are against public health programmes using DDT argue, amongst other things, that DDT is highly toxic and is also known to cause cancer in humans. Since the discovery of DDT countless millions of people have been exposed to DDT in one way or another. In this respect Smith states, "in the 1940s many people were deliberately exposed to high concentrations of DDT through dusting programmes or impregnation of clothes, without any apparent ill effect" (Smith 2000). Furthermore, since the 1940s, thousands of tonnes have been produced and distributed throughout the world and millions of people have come into direct contact with DDT. Initially, the distribution was restricted to soldiers in WWII and then to the general public in the aftermath of WWII. When demand for DDT escalated in the post WWII period, a plethora of studies were conducted with regards to DDT's safety for humans. Indeed, Smith notes, "If the huge amounts of DDT used are taken into account, the safety record for human beings is extremely good."(ibid) DDT and Toxicity
Scientists have studied very few chemicals as extensively as DDT, either experimentally or in human beings. Opponents of DDT have made many claims about the toxicity of DDT to humans but most claims have not withstood careful investigation. According to Curtis a thorough study of the health of men who had worked with DDT for years as spray-men "showed no significant excess prevalence of any disease in them compared to parallel studies conducted at the same time" (Curtis 2002). Furthermore, a controlled study conducted on the long term effects of DDT exposure in the early 1950's, which was funded by the United States Public Health Service, found that despite the volunteers in the sample consuming as much as 35 milligrams of DDT every day for 18 months, no adverse effects were found, either at the time of the study or during the follow up investigation ten years later (Hayes et al 1956, 1971). Indeed, Smith notes, "Ingestion of DDT, even when repeated, by volunteers or people attempting suicide has indicated low lethality, and large acute exposures can lead to vomiting, with ejection of the chemical" (Smith 1991). However, because malaria control involves indoor residual spraying, the emphasis here should be on the effects of DDT on the human through inhalation and not consumption. Considered in this light an assessment from the Agency for Toxic Substances and Disease Registry contains the following conclusions for non-occupational inhalation exposure: "No studies were located regarding death in humans or animals after inhalation exposure to DDT or any of its derivatives DDE, and DDD". Furthermore, they note that "No studies were located regarding cardiovascular, gastrointestinal, haematological, musculoskeletal, hepatic, renal or dermal effects in humans or animals after inhalation exposure to DDT, or its derivatives DDE and DDD" (ATSDR 2002). Smith also notes, "there are few toxicological effects due to inhalation of DDT" (Smith 1991). Thus in terms of the toxicity of DDT and its derivatives to indoor residual spraying on both an acute and chronic basis, the results tend to suggest that DDT is relatively harmless to humans and animals. DDT and Cancer
Early research in the 1950s found that DDT and its derivatives accumulated in human and animal tissue fat. In this connection one of the most common allegations against DDT is that it is carcinogenic. Although this allegation has been publicised widely by various organisations and commentators, there is little substance to the claim. Proponents of DDT carcinogenicity base DDT's link to cancer on finding significantly more of the DDT derivative, DDE, in the serum of patients dying of cancer compared with healthy controls. Recent evidence, however, has tended to suggest that DDT is not as potent a carcinogenic as originally thought. The International Agency for Research on Cancer (IARC), classifies DDT as "a possible carcinogen". Although, this statement is not definitive by any means, it should be noted that DDT shares this classification with a number of other common household consumables, such as peanut butter, beer and coffee. Furthermore, one must consider that DDT was used extensively for a number of decades and yet there is still no conclusive evidence that links DDT to cancer. Indeed, "no reputable authority declares unequivocally that DDT causes human cancer."(Smith 2000) Furthermore in all the years that DDT has been used, not a single case control study has been able to affirmatively replicate DDT carcinogenicity in humans (Attaran et al. 2000). Nevertheless, one of the most common concerns about DDT is that it causes breast cancer. The concern over DDT and breast-cancer is that it can act like a weak estrogen, and it is believed that the more estrogens a women is exposed to, the greater her risk of breast cancer. In earlier studies into the effects of DDT on breast cancer, researchers thought that they discovered a statistically increased risk of breast cancer and attempted to replicate these studies. However, since then, researchers have conducted numerous studies, but as of yet, none of them have managed to confirm the earlier results. A recent long-term study conducted by the Harvard School of Public Health found no relationship between the level of DDT in women's blood and their likelihood of subsequently developing breast cancer (Hunter 1997). Furthermore, the Agency for Toxic Substances and Disease Registry notes, "The possible association between exposure to DDT and various types of cancers has been studied extensively, particularly breast cancer. Thus far, there is no conclusive evidence linking DDT and related compounds to cancer in humans" (ASTDR 2000). DDT and Maternal Lactation
DDT is fat-soluble and accumulates in fatty tissues of humans and animals. Numerous studies have found that DDT and its metabolites are present in breast milk. A study of homes in South African villages that IRS programmes had sprayed with DDT showed a much higher level of DDT and DDE in breast milk in treated villages than in villages without IRS spraying (Bouwman et al 1990). The intake of 0.100mg/kg/day of DDT+DDE by babies consuming this milk exceeds by 5 times the Food and Agricultural Organisation (FAO) defined allowable daily intake (ADI). Although this may seem worrisome, it is not clear whether these levels actually do any harm. Furthermore, it should be noted, "the ADI levels are specified on the assumption that they would continue throughout life" (Curtis, 2002:458). Even researchers who find DDT in breast milk and claim that it leads to early weaning in children confess that there is a "lack of any detectable effect on children's health." (Attaran et al 2000) South Africa's public health professionals and politicians concluded that the hazards from malaria far outweighed any associated with DDT exposure - specifically including the breast milk issue. Furthermore, it must be borne in mind that DDT is not absorbed through the skin, and thus the concern here should be whether or not DDT causes ill health effects through inhalation. However it has been shown that the inhalation of DDT has little to no effect on humans. Therefore, in light of this, small amounts sprayed on the walls of dwellings are unlikely to pose any serious threats. Although the concerns that DDT may affect human health should not be dismissed, these fears should in no way prevent DDT from being used in malaria control programmes. The scientific evidence that DDT is harmful to humans is weak at best, and yet DDT's public health benefits are well known and very significant. Based on the real, immediate and deadly risks that people face from malaria and the lack of evidence against DDT, despite decades of use and numerous studies, any decision on whether or not to use DDT based on human health effects would rule in favour of DDT. DDT and the Environment
When agriculture used DDT in large quantities, spraying it almost indiscriminately, it caused certain harmful environmental effects. As DDT and its isomers are stable and persistent, they remain in the upper layers of soils and in the lower sediments of waterways for some time. (Most of the studies into the persistence of DDT have been conducted in the cooler climates of the northern hemisphere. In warmer tropical climates, DDT does not persist as long in the environment.) DDT's environmental impacts however should be seen in context. IRS requires small amounts, typically less than a pound (approximately 450 grams), for a very large house, which is sprayed directly onto the inside walls of the dwelling. Therefore, in malaria-prevention programmes little or no DDT gets tracked outside. Even if DDT does somehow escape into the wider environment, the amounts are so minuscule, and the time frame so staggered, that it seems unlikely to do any significant damage to the immediate environment, let alone far-off distant places. In this connection a study conducted by Bouwman et al concluded, "there are no significant variations in the levels of DDT in the environment before and after spraying" (Bouwman et al 1990). Furthermore, the World Health Organisation notes, "The safeguards inherent in the WHO recommendations and guidelines on the use of DDT for disease vector control present a much diminished environmental and/or health risk, if any." (WHO 2004) While the human health and environmental concerns surrounding the use of DDT are not credible arguments against its use in malaria control, issues concerning the management and funding of IRS programmes do deserve discussion. Economic and Managerial Issues
'Sustainability'
Numerous countries in southern Africa, such as Swaziland, South Africa, Namibia and Botswana have maintained and sustained successful IRS programmes for many decades. Part of the reason for this success is the scientific oversight and tight controls within these vertically run programmes. However IRS programmes are not the preserve of countries with higher per capita gross domestic product (GDP) or with small numbers of malaria cases. For many years Madagascar, which has a per capita GDP well below the average for Sub-Saharan Africa, has maintained a well-run IRS programme in the highland areas using DDT. Zambia has recently restarted its IRS programmes in the districts of Ndola, Kitwe, Kabwe, Livingston and Lusaka. Both of these countries receive funds for their programmes from the Global Fund for AIDS, TB and Malaria (GFATM) and from their national fiscus. In the case of Zambia, the private sector has also made a significant contribution to malaria control (Sharp et al 2002). The success of many of the GFATM interventions and the prospect that the mechanism will continue for many years will ensure long term funding options for IRS programmes. The argument that IRS programmes are not sustainable is often made. Yet it lacks credibility when one considers the numerous successful, long-term programmes that are in place. The corollary of the argument that IRS is unsustainable is that other programmes, such as the social marketing of insecticide treated nets (ITNs), are sustainable. ITNs are an important component of any malaria control programme, however programmes that rely too heavily on this intervention, such as Roll Back Malaria, have not demonstrated any reduction in malaria cases or deaths (Mandavili 2004). Issues such as the pricing of nets, the logistics of distribution and re-treatment are controversial and continue to hamper the effective roll out of this intervention. Thus, it is not clear that ITNs are in any way a more 'sustainable' solution than IRS, particularly when one considers the lack of any large-scale successful implementation of ITNs. The factors influencing malaria control differ from country to country. Therefore Uganda should conduct its own, in situ, studies to determine which intervention is likely to achieve the best results. Management of IRS
There are valid concerns that without good planning and controls, DDT will be diverted from public health programmes into the agricultural sector. However this is not an argument against DDT use, but rather an argument in favour of setting up the right institutions to manage its use. As noted above, Konkola Copper Mines reintroduced DDT into Zambia in 2000 after Zambia had discontinued its various IRS programmes, mostly due to a lack of finance, in the 1980s. Before any DDT spraying could begin, however, the Environmental Council of Zambia (ECZ) evaluated the need for DDT and set out the conditions and regulations of such use. The ECZ granted authorisation only if the agents using DDT, in this case mine employees, could guarantee that they would transport, store and use it responsibly and according to WHO guidelines. The programme managers also had to ensure that systems were in place to ensure that no DDT is diverted from the malaria control programme to the agricultural sector. Those same controls and oversight also apply to the use of DDT by the Department of Health in the various other IRS programmes that use DDT in other parts of the country. Ensuring that programmes use DDT, indeed any insecticide, properly and according to best practices and guidelines is important for malaria control. Malaria control programmes will fail if officials divert resources away from public health programmes for their own profit. Spray programmes have to apply DDT or any other on the inside walls of houses in the correct manner and in quantities that will be lethal to the adult Anopheles mosquitoes. Failure to do this could lead to insecticide resistance, which would clearly be problematic for any control programme. The fact that little or no resistance to DDT has developed in Southern Africa is a testament to the many years of rigorous control and good scientific oversight. When Uganda begins to use DDT in its IRS programme, it is essential that it instils measures to track and monitor the use of insecticides. Failure to do this will not only compromise malaria control but could also jeopardise exports. The various sanitary and phytosanitary regulations that affect agricultural exports are often onerous and could block agricultural, floral and fisheries exports from Uganda if traces of DDT are found on the products. No agricultural or environmental contamination of DDT should result as a result of IRS activities as IRS involves spraying small amounts of insecticide inside houses and under the eaves of houses. Concerns over DDT harming Uganda's trade have little to do with the merits or demerits of DDT itself, but rather with the organisations that control and monitor the use of DDT. As with every other country that uses DDT, it is incumbent on Uganda to ensure the correct institutions are in place before IRS begins. Conclusions
DDT has a long and proven track record in malaria control. When used in public health programmes, DDT is responsible for saving countless millions of lives from malaria and other vector borne diseases such as typhus and yellow fever. While one should not dismiss the studies conducted into the human health and environmental effects of DDT, they should be seen in context. In addition, any evaluation of the need for DDT must recognise the controlled and careful way in which DDT is used in malaria control. Essentially policy makers need to compare the real risks that people face from malaria with the often uncertain and hypothetical risks that people would face from DDT. Given close correlation that DDT has with reduced mortality and morbidity and the lack of credible evidence with regard to harm to human health and the environment, policy makers cannot but argue in favour of DDT. That said, any country that wishes to implement an IRS strategy, whether it uses DDT or any other insecticide, has to ensure that the right regulatory controls are in place and that the programme is conducted according to WHO guidelines and has strong scientific oversight. Uganda has an important opportunity to improve malaria control and save lives by using DDT in a carefully controlled programme. As that programme begins, it is essential for officials, the private sector, academia and civil society to approach the issue with due regard to science and good medicine and without emotion or regard to politics; anything less will compromise malaria control and cost lives. References
Copyright 2004 - Department of Health Sciences of Uganda Martyrs University |

{kind=link}