 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 2, No. 2, Aug, 2004, pp.151-160 AUTONOMY OF APEX HOSPITALS IN UGANDA: TOO LITTLE, TOO SLOW Akello Evelyn, Hospital Administrator, Murchison Bay Prison Hospital, Luzira Code Number: hp04025 Abstract Hospital Autonomy, a sustained and purposeful change to improve the efficiency, equity and effectiveness of the health sector has been initiated to improve publicly-owned hospitals which, in many developing countries, consume large portions of scarce health sector resources and do not always use them effectively and efficiently. While the general consensus seems to be that public hospitals are in need of urgent reform, autonomy seems to be emerging in international debates as the main approach to be followed. Its central idea is the decentralization of management authority and responsibility away from the central or regional managers to a local level, focusing mainly on five main administrative and functional areas: Strategic/General Management, Financial Management, Human Resource Management, Procurement and Administration. In Uganda, the Ministry of Health (MOH) granted the two National Referral Hospitals, Mulago and Butabika, a very limited "self accounting" status of autonomy, with a view to extend greater autonomy to these two and ten other regional referral hospitals by 2003. The focus of this study was to assess the extent of implementation of the autonomy by the two that had been autonomous for over ten years. Introduction Hospital Autonomy is part of health sector reform, which is, itself, a sustained and purposeful change to improve the efficiency, equity and effectiveness of the health sector (Berman, 1995 in Mills 2000). Hospital Autonomy as a reform has been initiated in many countries to improve efficiency and quality of publiclyowned hospitals. In many developing countries, public hospitals consume large portions of scarce health sector resources and do not always use them effectively and efficiently (Collins et al, 1996) The general consensus seems to be that public hospitals are in need of urgent reform. Hospital autonomy is the reform emerging in international debates as the main approach to reforming hospitals so as to improve management performance and efficiency. Its central idea is the decentralization of management authority and responsibility away from the central or regional managers to a local level. In Uganda, measures to increase hospital autonomy were initiated in response to chronic shortages of drugs and supplies, delays in disbursement of funds and the disproportionate share (40%-50%) of the health budget that was being absorbed by Mulago Hospital Complex alone (Atuyambe et al, 2002). The Ministry of Health (MOH) requested consultants to study how to implement hospital autonomy. The consultants proposed the legal and managerial arrangements for autonomy and outlined a plan of implementation. To achieve autonomy, the implementation plan needs to focus on transferring the decision-making authority to hospitals with regards to five main administrative and functional areas: strategic/general management, financial management, human resource management, procurement and, finally, administration. Autonomy granted may be to different degrees: limited autonomy where the hospital managers may take recourse to the central Ministry of Health as opposed to full autonomy where hospital managers can make decisions completely outside the Ministry of Health. In Uganda the MOH granted the two National Referral Hospitals, Mulago Hospital Complex and Butabika Mental Hospital a limited status of autonomy, i.e "self accounting status". The ministry planned to grant the two hospitals and the regional referral hospitals greater autonomy eventually. The full implementation of autonomous status was expected to be completed by 2003 (Hanson et al, 2002). The focus of this study was to assess implementation of hospital autonomy by the two National Referral Hospitals that had been autonomous for over ten years. The aim of the assessment was not to measure the impact of autonomy on quality of care outcomes or provide an opinion on whether or not the hospitals were operating efficiently but rather to better understand the process of autonomy that the hospitals were implementing and to identify problems that would be an obstacle for implementing autonomy. The study also assessed the extent and benefits of autonomy so far attained and determined whether the hospitals could attain full autonomy in the near future. Motivation for Autonomy
Autonomy as a reform was initiated in many countries to improve efficiency and quality of public hospitals. Some of the problems experienced with public hospitals i.e. chronic shortage of drugs and supplies, delays in disbursement of funds and a disproportionate share of the total health budget, could be addressed by moving away from direct central management by the Ministry of Health (Needleman et al, 1996). As a result, many developing countries proposed "hospital autonomy" initiatives as an integral part of a broader sector reform process (Chawla and Govindaraj, 1996). In Uganda, three major studies were commissioned which recommended the autonomy process for Mulago, Butabika, Masaka and Jinja hospitals. The key recommendations of the studies summarized the following issues: introduction of autonomy to the above mentioned four hospitals, legal framework to establish hospital trusts, establishment of hospital boards, memorandum of understanding with Makerere University Medical School, separate arrangement for other health training institutions, transfer of staff from the Public Service Commission to the hospitals including all human resource issues, development of accounting systems and common accounting codes and a request for the MOH to establish an autonomy unit and task force to manage the process. Extent of Hospital Autonomy
The extent of autonomy will depend on the degree to which the government continues to retain control over the various functions of the hospital. It is often left to individual countries to decide, based on their specific needs and circumstances (Shehata and Cripps, 2000). Chawla et al. (1996), in a conceptual framework for hospital autonomy defined extent of autonomy along a zero-one continuum, where a centralized system was ranked closer to zero (low autonomy) and a decentralized system closer to one (high autonomy). Autonomy focuses on five main administrative and functional areas which may be ranked either as low, fair or high. Strategic or General management: Chawla and Govindaraj (1996), found that hospitals in Ghana, India and Indonesia had some autonomy in defining the overall mission of the hospital, setting broad strategic goals, managing the hospital's assets and bearing ultimate responsibility for the hospital's operational policies. Kenyatta National Hospital in Kenya and Parienyatwa hospital in Zimbabwe had very little freedom. Financial management: Chawla and Govindaraj (1996) found that hospitals in all the countries studied had a fair degree of financial autonomy. Virement was done and they constructed their own budgets without regard to the Ministries of Health or the national Treasury controlling allocations to specific line items. Hospital management was encouraged to mobilize resources though many restrictions were put on raising revenue through user fees. Human resource management: As a general rule, recruitment, promotion, disciplinary action and dismissals are the responsibility of the Public Service Commission or Health Service Commission. With autonomy these functions were to be delegated more to the hospitals. Chawla and Govindaraj (1996), found that in all the cases studied, government had retained the power of hiring and firing, even in the case where the hospital staff ceased to be government employees after autonomy. In Indonesia, Ghana and Zimbabwe, hospital employees continued to be civil servants and governed by public service commissions that had restricted the ability of the hospital to redefine its staffing needs and hire or lay off workers in response to those needs. Procurement: Chawla and Govindaraj (1996) found that some of the countries studied, enjoyed considerable autonomy in procurement of supplies and equipment. Autonomous hospitals in India and Indonesia had effectively set up their own procurement protocols, though following government rules and procedures in principle. Procurement was somewhat limited in Zimbabwe and Ghana, where the hospitals still procured from central stores. Administration: Hospitals need to have detailed operational and financial plans covering the services to be delivered, human resource plans and plans for new developments. This involves developing service agreements and performance measurement systems. In studies carried out by Chawla and Govindaraj (1996), most autonomous hospitals enjoyed considerable freedom in routine day-to-day administration. Efficiency Measures related to Hospital Autonomy
There are various measures that have been used to improve efficiency. Contracting out services to a separate organization is likely to improve efficiency because it involves clear specification of the service to be provided with quality standards, monitoring of service provision and competitive tendering for the contract, which should result in lower costs for the service. Procurement and management of drugs is an area where there is often scope for major savings especially if the purchases are made in bulk from a central procurement agency. Clinical unit budgets and management is an efficiency measure that dictates that instead of budgets being managed by central managers, the budgets and responsibility are broken down and allocated to departments. This should lead to improved efficiency because decisions will be made with better information on need and priorities. Changing staffing level and mix can improve efficiency but only if the staff review leads to either a reduction in the number of staff relative to patient throughput or a better mix and deployment of staff. International comparisons can provide a useful benchmark - for example, a World Bank document on hospitals in Africa based its calculations on 60 staff for a 140 bed hospital or a 0.5 staff per bed (World Bank Publication, 1993) Making more efficient use of beds and facilities/ improving throughput: It is now recognized that it is not necessarily beneficial for patients to stay on at the hospital. However it is worth noting that while efficiency improves with this type of change, as more patients are treated, the total cost of provision is likely to increase. (Grant & Walford, 1998). Reducing inappropriate use by ensuring that the hospital performs the purpose for which it was established. Comparisons and value-for-money studies across hospitals: A common finding by Chawla and Govindaraj (1996) was that after autonomy there was no change in the traditional indicators, like bed occupancy rates and average length of stay. However, the hospitals studied recorded significant improvements in management, finance and accounts, inventory control and general maintenance. Benefits associated with Hospital autonomy
It has been suggested that hospital autonomy may lead to gains in both technical and allocative efficiency (Chawla and Govindarj, 1996). Reasons for efficiency gains include assumption of greater responsibility and authority by hospital managers to address and use resources more efficiently. In general, it is argued by proponents of greater autonomy that it would contribute to improving efficiency and quality of care provided by hospitals. (Mills, 2001). Problems faced in implementing Hospital Autonomy
The most important potential drawback of providing autonomy to public hospitals may be equity in the financing as well as delivery of health care (Chawla and Berman, 1995). Ann Mills in a presentation "Achieving efficient and equitable health care in Africa: What is needed?" noted that contracting out (which may be a way of improving the procurement function under autonomy) may be difficult if the private sector is poorly developed. Exemption schemes in the case of user fees were usually difficult to implement and there was lack of accountability leading to exploitation of the patients and the facilities. There was often lack of the required skilled human resource. The information system was inadequate. There was also a mismatch between the organizations' culture and reform requirements. (Mills, 2000) Perception of staff about Hospital Autonomy
One of the key mechanisms for achieving a smooth transition to greater autonomy is communication with those affected about the changes from an early stage in the process, i.e. the staff and public. This helps to prevent misinformation and development of resistance and lobbies against the change. In conclusion, it is noted that a significant amount of research has been done about Hospital Autonomy. However a knowledge gap can be identified with regards to the assessment of the implementation process in Uganda. Preparing hospitals for autonomy
For the hospitals to be legally recognized as autonomous institutions, MOH had mandated each hospital to draft a Bill to cover its own autonomous status. These were prepared but were yet to be approved by MOH before being presented to parliament. Both hospitals had defined and described their missions as well as strategic objectives. They had clearly identified their target populations and were functioning as National Referral Hospitals with three specific objectives: to provide specialized tertiary health care, act as a teaching institution and carry out research. The Executive Directors of the two hospitals were members of Top Management of the MOH implying the hospitals played a role in the setting of national health goals and policies. Financial management The main source of revenue for the hospitals was the Government of Uganda through delegated funds and, to a limited extent, donors who had to be approved by the MOH. Mulago collected revenue from its private wing and other private services rendered. Revenue collected was transferred to the consolidated fund. The funds were then given back to the hospital as part of delegated funds from the central government. Fees to be charged by Mulago were determined by the hospital but had to be approved by the MOH. Butabika did not provide private services and thus had no avenue for charging fees. Each hospital drew up its own budget within ceilings that were set by the MOF. The hospitals were allowed virement of funds only with the permission of the Permanent Secretary MOF, and they could not sell off their assets. The staff members of their Accounts Departments were seconded to the hospitals by the MOF. According to interviews carried out and records reviewed the level of funding from the central government had improved with autonomy. Human Resource Management The responsibility and authority of making personnel decisions lay with the Health Service Commission (HSC) and the Public Service Commission (PSC). The hospitals declared vacancies to the Commissions for filling and defined the requirements for the jobs. During selection the hospital was represented on the interviewing committee of the relevant Commission. Staff of the hospitals remained employees of the Ministry of Public Service. The hospitals had the mandate to suspend or interdict a staff without consulting the Ministry of Public Service (MOPS) or MOH. However, the prerogative of termination of appointment by dismissal, retirement in public interest or on grounds of ill health and redundancy, lay with the HSC or with the President on the advice of the HSC or PSC after full approval of MOH. At the hospital level, promotions were only possible when a position at a higher grade was vacated or if a vacancy existed in any of the other referral hospitals. Salary budgets were drawn by the hospitals and met by Ministry of Finance Planning and Economic Development (MOFPED). However, salaries would not be reallocated to other budget lines. If not used the money was returned to the Treasury. Allowances were paid by the hospitals from their respective votes. Staff pensions and gratuity were paid by the central government's Pensions Authority. Individual and donor sponsorship contributed far more than the hospital towards staff training, especially in formal long courses. Procurement The contracts committees supervised the procurement process with technical assistance from the procurement units. However, they had to function within the Public Procurement and Disposal of Public Assets Act of 2003, provided by the Central Procurement Authority (formerly Central Tender Board), which is an autonomous body supervised by the MOFPED. The hospitals procured drugs from the central store (National Medical Stores). If the drugs were not available at the central store, they were issued with a Certificate of Non-availability after which they could then procure from private pharmacies that had been approved by their respective Contracts Committees. This is the same procedure that operates for other health units of lower level. Administration Hospital Management Committees had remained in charge of the affairs of the hospitals. Over time it was expected that Hospital Management Committees would be dissolved and Boards of Directors would take over governance of the hospitals. In 1997, a Cabinet resolution to appoint Boards to govern Mulago and Butabika Hospitals was passed, but they were only appointed in 2003. The main responsibility of the Interim Boards was to prepare the hospitals for full autonomy within one year. The Interim Boards of Directors were non-statutory and had a mandate of three years. It was expected that within this period, parliament would have enacted the law on autonomy for each of the hospitals. With the law in place, the Interim Boards would be dissolved and a Board of Directors with statutory powers appointed. The Hospitals were able to introduce new services within the National Health Policy, and they had gone ahead to do so. The hospitals were headed by Executive Directors. For Mulago, the Executive Director was assisted by a Deputy Executive Director and "shadow directors"1 in charge of the hospital's directorates. For Butabika the Executive Director was assisted by a Deputy Executive Director, a Senior Hospital Administrator and a Principal Nursing Officer. Chief Executive Officers (CEOs) were yet to be appointed for the hospitals. It was likely that this would take sometime. Mulago was suggesting that instead of the title of CEO, the hospital could adopt the title of Director General. This was still under discussion. In any case a CEO would only be appointed after the Interim Boards had accomplished their Terms of Reference. Efficiency Measures
A number of efficiency measures are presented here below. Although they are also applicable in hospitals that have not been given autonomy, it is expected that autonomy guarantees their application. If not present in an autonomous hospital, it would be assumed that its efficiency was highly compromised. Both hospitals had in place contracts committees. The hospitals were using guidelines provided by the Central Procurement Authority. Due to contracting out, key informants identified areas of improved efficiency as reduced bureaucracy in procurement and "value for money" purchases. Drugs were purchased according to the essential drugs list and using generic names where available. User departments were involved in budgeting for drugs. Mulago was proposing to have directorates instead of departments. The Heads of the proposed directorates were referred to as "shadow directors" in order not to confuse them with the Director who was the head of Mulago. It had a staff total of 1,985 for 1519 actual beds, a ratio of 1.3 staff per bed. Butabika had 242 staff for 450 actual beds, a ratio of 1 staff per 2 beds. With autonomy, staffing level and mix was likely to change. The hospitals have proposed new staff structures that were yet to be approved by the MOPS. Butabika had scaled its number of beds from 970 to 450 in order to improve efficiency. Mulago had an average length of stay of 13 days. The length of stay in Butabika was of little statistical significance due to the unique nature of its patients. None of the hospitals had a Service Level Agreement with the MOH. However going by their mandates they were supposed to be National Referral Hospitals. But as a result of the failure of the referral system, they were not acting in this capacity. They were managing primary care patients as well as tertiary care and referral patients. MOH did not have an autonomy unit to oversee the implementation of autonomy. The task was under the jurisdiction of the Department of planning-MOH, with support from technical departments such as Clinical Services and Quality Assurance. No comparison and value-for-money studies had been carried out to monitor the progress of the autonomy. "It is still too early in the implementation of autonomy to carry out any such studies." (Key Informant). Benefits associated with Hospital autonomy
Respondents of the study identified the following as benefits that could so far be attributed to the two hospitals being granted autonomy. a) Increased efficiency, as the hospitals were able to take their own decisions without having to consult the MOH. b) The interim boards and hospital management had to work together to prepare the hospitals for full autonomy. With the guidance of each other, the members had displayed a high level of collaboration in decision-making and sharing responsibilities. c) The MOH did not have to involve itself in running the hospitals. This had enabled it to focus more on policy matters. The Ministry would only intervene in hospital issues when crises arose, that were beyond the board and hospital management. d) There was noticeable improvement in the quality of services as well as efficiency in management. e) The board of directors was expected to act as a public relations body for the hospital. The composition of the boards ensured that several interests were represented and this was a good way of taking feedback to the public. f) There was reduced bureaucracy in implementing management actions. Problems faced by the hospitals
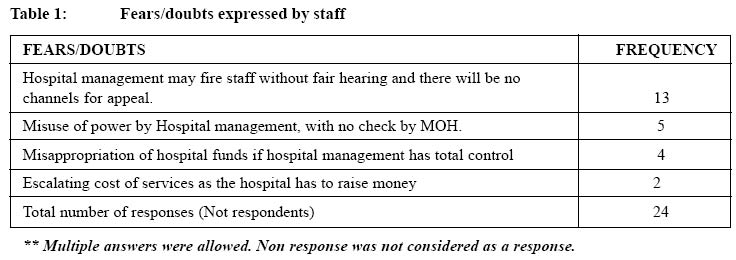
The hospitals do not have adequate funding. With autonomy this was bound to be a big problem. Hospital budgets had been increased by 29% in the Fiscal year 2003/04 and it was expected to increase further when Primary Health Care funding stabilized. Possibilities of raising funds from alternative sources had not been explored by the hospitals and the MOH. They were hoping for increased government funding. The hospital could not use revenue collected at source and according to key informant interviews, this affected their efficiency in quickly responding to problems at source. Equity concerns were expressed. With autonomy the hospitals would have to adhere more to their mandates as referral institutions. Patients would also be charged for services they received. This meant people who could not afford or did not have access to lower health units would have to go without services. Hospital management encountered fear and uncertainty in the staff about the hospitals being autonomous. Key informant interviews attributed this to the delay by MOH to clarify its position on autonomy. The managements of the hospitals were unable to sensitize staff because they themselves had not known what to expect and work towards. This role was just being clarified by the MOH. (Table 1) Perception of staff A total of 96 staff was interviewed. A similar number of 48 in each hospital2. Of the staff of Mulago interviewed, 47.9% (23/48) knew that the hospital was in the process of becoming fully autonomous, compared to Butabika where the percentage was higher; 66.7% (32/48). Of the staff interviewed, more of Butabika staff (30/48 or 62.5%) knew and were able to explain correctly what hospital autonomy meant than those of Mulago (15/48 or 31%). The majority of the staff interviewed (37/48 or 77.1% in Mulago and 30/ 48 or 62.5% in Butabika) had not been involved in any communication forum in which management briefed them on the status of the hospital with regards to autonomy. Most (44/96 or 45%) did not know whether there was need for the hospital to become autonomous. Some of the staff who knew about the hospital becoming fully autonomous had only heard about it from friends in management positions or in the 'corridors' of the hospitals. However, of the respondents who were heads of departments and who were, therefore, key players in the planning for the hospitals and the implementation of autonomy, the majority (8/12 or 57%) were aware of the process and had been involved in either a meeting or workshop on the issue. All heads of departments interviewed could identify some changes that had taken place in their departments as a result of the hospital becoming autonomous. Changes mentioned included increased participation of departmental heads in budgeting and planning activities of the hospital and specific procurements tailored to the needs of the departments. However, the other staff interviewed in the two hospitals (35/48 or 73% of Mulago staff and 28/48 or 53% of Butabika staff interviewed) could not identify tangible changes that had taken place in their hospital that they could attribute to autonomy. Those who could identify some changes were only able to recall the recent changes that were still taking place. Asked for some recommendations on the handling the granting of autonomy to the hospitals, the respondents from Mulago Hospital suggested that the hospital had adequate financial management capacity and that it should therefore be allowed to use its collections at source. In general, the two groups suggested that the process of transfer of personnel from the Health Service and Public Service Commissions to the full control of the hospitals should be done gradually and slowly and that a lot of caution should be taken to ensure that sufficient human resource management capacity has been created at the hospitals before the transfers. They also suggested that the MOH should be more serious in setting up and operationalising the structures to monitor the hospitals to make sure they use the powers entrusted to them by autonomy properly. Extent of autonomy
The two hospitals had a fair degree of autonomy in defining the overall mission, setting strategic goals, managing the hospital's assets and bearing the ultimate responsibility for the hospital's operational policy. The level of autonomy was judged to be fair because much as they were able to define their own mission and objectives they had to do this within the parameters of the National Health Policy and the Health Sector Strategic Plan set by the MOH. This had also been found to be the case in Chawla and Govindaraj (1996), where autonomous hospitals of Ghana, India and Indonesia had fair autonomy in this area but those in Kenya and Zimbabwe had very little freedom. Financial management
This was perhaps one of the areas in which the hospitals had the lowest level of autonomy, despite being self accounting for over ten years. The fact that the hospitals had to stay within the guidelines set by the MOFPED in drafting their budgets, that revenue collected could not be used at source, that virement was not allowed and that they could not sell their assets implies that they have limited freedom in making financial decisions. At the moment it did not seem likely that the hospitals would be able to mobilize additional resources. Other hospitals in similar circumstances had adopted some measures. Kenyatta National Hospital had introduced user fees and raised 20% of costs through fees (Grant and Walford, 1998) while the most successful fundraising scheme for the Andhra Pradesh Vaidya Vidhan Parishad Hospitals in India was donations from the public and from charitable organizations (Chawla and George, 1996). Human Resource Management
This aspect was judged to have the lowest level of autonomy. The very limited autonomy over personnel the hospitals had was not likely to improve in the near future. Yet, hospital managers need the capacity to promote, reward and punish staff if they are to improve staff motivation and performance. The HSC and PSC retained the prerogative for personnel decisions. Employment issues, particularly the transfer of staff from a central civil service to a hospital unit are often the most sensitive and difficult aspect of the autonomy process. It requires careful design and sensitive handling. (Grant and Walford, 1998). The assumption at the moment by the two hospitals is that personnel decisions would remain the responsibility of the HSC and PSC. In the eventuality that this was not the case and human resource management was transferred to the hospitals, there was bound to be a lot of confusion as had happened at Kenyatta National Hospital when, without much planning, personnel were transferred to the hospital (Collins et al, 1996). Procurement
The level of autonomy enjoyed by the hospitals on procurement was judged to be fair, because although they had local procurement units, they had to adhere to procurement protocols laid out by the central government's Public Procurement and Disposal of Public Assets Act (2003), issued to them by the Central Procurement Authority. Making purchases from the NMS limited the procurement freedom of the hospitals. However, centralized purchasing from the NMS enabled the hospitals to take advantage of bulk purchases and they could decided on what purchases to make. Administration
As in the studies carried out by Chawla and Govindaraj (1996), Mulago and Butabika as autonomous hospitals enjoyed considerable freedom in routine day-to-day administration. However, since the Boards are answerable to the Minister of Health, this probably has an implication on their freedom to make decisions independent of influence from the central government. Fears still linger that when Boards of Directors are influenced by the government, many of their decisions may have to be sanctioned before they are implemented. However, if the performance of the current Interim Boards of Directors of the two hospitals is anything to go by, there may be little to fear for this. They have so far proved to be effective buffers between the government and hospital managements. For autonomy to succeed, the boards have to be independent, efficient and competent. Collins et al (1996) noted that when the Board in Kenyatta National Hospital became more independent and involved in management, the private sector became even stronger and able to meet the requirements of the hospital. Efficiency measures related to hospital autonomy
The hospitals were successfully implementing the various measures, which had probably led to improved efficiency. This study does not suggest whether or not efficiency improved due to the hospitals becoming autonomous. However, some of the responses elicited from key informants and staff revealed that indeed efficiency had improved at the hospitals. This was further supported by the fact that in both hospitals, 6 of the 7 suggested efficiency measures were in place and being utilized. Contracting out services enabled the hospitals to improve efficiency because they were able to make clear specifications of the services and goods to be provided stipulating quality standards. With clinical unit budgets, the staff members were able to make their own decisions on needs and priorities. The limited role of staff in the control of resources limited their motivation to improve performance. However to hand over the control of resources, for example enabling departments to retain some of the income generated, is an ambitious plan that needs careful designing. Reviewing staffing levels can improve efficiency. While a World Bank document on hospitals in Africa based its calculations on 0.5 staff per bed and workload calculation in Cambodia gave similar conclusions Mulago had 1.3 staff per bed and Butabika 0.5 staff per bed. It can be argued that increasing the number of staff may improve efficiency, while other may argue for the opposite. This study takes the former position if quality of services is considered. Moreover, the shortage of staff came out as a problem in both hospitals. This could have affected the quality of health care delivery, although this aspect was not the subject of this study. The average length of stay of Mulago had steadily declined over the years. However as in Grant and Walford (1998), this probably implied an increase in the total cost of provision. If post operative stay was shorter then some relatively inexpensive days spent in recuperation would be replaced by operations on other patients which would be more expensive. To solve this beds could be closed if they were likely to create problems. Contentious as the issue may be, Butabika had gone ahead and reduced its number of beds. It is not efficient to use expensive and limited national hospital facilities and staff if lower level health centers and hospitals are adequate and cheaper. In principle service agreements could help by clarifying the services each hospital was expected to provide. However, in the absence of service agreements between the hospitals and MOH, the service packages outlined in the HSSP provided guidance. But the issue of a non functional referral system is difficult to resolve, as it requires improving the referral discipline and other issues such as adequately providing lower level units with the relevant staff, drugs, equipment and infrastructure. Many of the efficiency measures would also be applicable in hospitals, which have not been given management autonomy. Benefits associated with hospital autonomy
There was a general consensus among the heads of departments interviewed that there was need for the hospitals to become autonomous. However the ordinary staff would not tell for sure if there was a need. Respondents were able to identify benefits that were being enjoyed by the hospitals due to autonomy. This would imply that the benefits of autonomy were clear to them. But this was only true for key informants from the MOH and the hospitals and the heads of departments. However, it should be noted that identifying the benefits only is not enough. It is important for the staff to appreciate these benefits. Judging by the tone of response during interviews, the investigator made the conclusion that the key informants and heads of departments appreciated the benefits they had identified. However, it should be noted that these benefits cannot be attributed entirely to Hospital Autonomy. They may be other factors not identified by the study that contributed to the achievement of the benefits. Problems faced by the hospitals
Inadequate funding of the hospitals was a big problem in the implementation of autonomy. Funding ceilings could have to be made more flexible so that the hospitals could seek, negotiate and receive funds from other bodies without affecting government funding. Borrowing a leaf from the APVVP Hospitals of India (Chawla and George, 1996) the hospitals could consider mobilizing donations from the public and charitable organizations. Government partly because of the equity problems it was creating, abolished user fees and allowed fees to be charged only in the private wing. It can be noted that none of the hospitals will be able to finance their operations from fees charged and also ensure access to all those who are in need of the services. The exemption scheme would not be able to solve the equity problem. Closely linked to the equity problem was the inadequately functioning referral system. However for the moment this was a problem that could not be easily solved because it was outside the ability of the hospitals to solve alone. It required the involvement of all stakeholders of the referral system. Accountability concerns lead to MOF stipulating that hospitals remit collections back to the consolidated fund. As much as the hospital managers longed to see this stipulation reversed, key informants from the MOH were of the view that it would continue. But, there are institutions such as Makerere University that on being granted autonomy were allowed to use their collections at source. This would be explored with autonomous hospitals too. Significant investment in preparation was required if autonomy was to be implemented successfully. This included the MOH clearly communicating to the hospitals what autonomy entailed so that the hospitals could also communicate to its staff and reduce on the fears and doubts that were already arising among staff. Perception of about autonomy
Perception of staff was low (46.7%), especially among the staff of Mulago. Hospital management had not taken the initiatives to communicate adequately to the staff. With the exception of heads of departments, majority of the staff (70%) had not been involved in any communication forum about autonomy. One of the key mechanisms for achieving a smooth transition to greater autonomy is communication with those affected about the changes from an early stage in the process. This prevented misinformation and development of resistance and lobbies against the change. The study revealed that the staff already had fears and doubts arising from lack of information about autonomy. Butabika would find it easier to communicate to its staff who were few, as opposed to Mulago that had 1,985 staff. It was likely that level of awareness was higher in Butabika because the staff were few and could easily access information. The low level of awareness subsequently led to a high number of the staff not knowing whether there was need for the hospital to become autonomous. Staff interviewed could not identify changes that had taken place in the hospital due to autonomy. Again the larger number was in Mulago. Mulago hospital managers interviewed attributed this to the fact that the hospital had been semi autonomous for so long (since 1987) that the staff could not really identify any changes which took place then or now. They had been at one level of autonomy (self accounting status) for so long, any additions were just normal states of affairs in the hospital. Conclusion
In conclusion, the extent of autonomy that had so far been granted to the hospitals was relatively low. Implementation of autonomy was being carried out at a much slower pace than recommended by the consultants. Going by the findings of the study, the possibility of the hospitals becoming fully autonomous soon was limited. However with time it was possible for them to achieve full autonomy. Recommendations
References:
|

{kind=link}