 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Health Policy and Development Journal, Vol. 2, No. 2, Aug, 2004, pp.161-167 CONTINUING MEDICAL EDUCATION : LESSONS FROM BUTAMBALA HEALTH SUB-DISTRICT Lule Haruna, Gombe Hospital- Mpigi District Code Number: hp04026 Abstract Continuing medical education (CME) is one way of keeping health workers updated with the new developments and new insights in treatment and approaches to health issues. It also helps them remember what is forgotten. This study, conducted in Butambala Health Sub-district (HSD) by interviewing all the health workers on duty found that health workers knew the importance of CME. However in 2002/2003, CME activities were not properly planned for while the selection of topics, participants and co-ordination of CME activities in the HSD left unmet needs in some areas of the medical field as well as ignoring some cadres of health workers. Despite all this, the general trend of events regarding CME in the HSD was positive. The study recommended proper and participatory planning for CME preceded by training needs assessment, increase of budgetary allocations for CME and the creation of a CME registry for the HSD, as some ways to further improve the situation. Introduction Continuing Medical Education (CME) or In-service Training (IST) for medical workers is a process in which the competencies of health workers continue to be maintained, improved and new ones acquired following the completion of basic training. CME can be accessed through workshops, seminars, clinical audits, formal lectures, radio and television programmes and support supervision, among others. Psychologists have demonstrated that human beings learn through repetition and that skills are easily recalled if regularly reviewed. In one study, Herman Ebbinghaus (1885) studied the relationship between regular reviewing of notes and information recall of a group of students followed for nine weeks. The study revealed that at the end of the nine weeks, those who reviewed their notes within a day of study recalled about 75% of the information while those who never did, were unable to recall even 50% after one day and only a little more than 20% of the information after nine weeks. These results, shown in Figure 1 below, later came to be known as the now famous "Forgetting Curve" of Ebbinghaus. Thus healthcare providers, being the most important asset of any healthcare system, also need a structured process of continuous training, exposure, learning and improvement in order to continually apply their skills and knowledge correctly. Without such opportunities, health workers, particularly those in rural areas, will experience a decline in the skills and knowledge, professional dissatisfaction, low morale, disillusion, lack of commitment and reduced interest in their work. Ultimately, this affects the quality of the care they give to the patients and communities. On the contrary, however, apart from attending the training activity to acquire new skills or improve on skills already possessed, it is motivating for a health worker to be selected for a given course for he/she feels recognized by his/her seniors. Countries all over the world have developed CME programs, which are reviewed from time to time. In October 2002, a regional consultation on CME in East Africa was held in Kampala, Uganda. This meeting arose out of the realization that the East African region required a CME program that addresses all cadres of healthcare providers with special attention to improving performance in order to ensure quality health service delivery. This meeting recommended that in order to improve CME delivery in the region, they had to, among other things, consider distance education to avoid health workers leaving their work stations, establish satellite centers for CME accessible to all health workers, have focal persons for all CME activities, offer regular support supervision, educate all stakeholders to appreciate and prioritize CME activities, integrate CME in all activities, enlist the active participation of Universities and other training institutions as well as providing health workers with opportunities to identify their own CME needs. The National In-service Training Strategy (ISTS) in recognition of the national health policy and its implementation through the health sector strategic plan, focuses on enabling the majority of health workers deliver the elements of the Uganda National Minimum Health Care Package (UNMHCP). One of the roles of the districts and the health sub-districts is, therefore, to ensure that all health units at all levels offer services included in the UNMHCP. Some of the strategies to achieve this were to recruit new health workers, as well as exposing those already in service to Continuing Education. This led to many health workers (in both public and NGO units) undergoing various short term and midterm training like the Integrated Management of Childhood Illnesses (IMCI). Besides attending workshops, health workers receive continuing education through support supervision and other health unit-based team/ ward discussions. For the health unit-based Continuing Medical Education (CME), health workers organize meetings where selected topics can be presented and discussed, giving each participant a chance to contribute. The health sub-district (HSD), one of the forms of the health sector reforms of the late 1990s, was mainly aimed at transferring service delivery from the district health offices to the lower levels, increasing equity of access to essential health services and fostering community participation in health service delivery. So, one of the supervisory roles of the health sub-district to the lower health units is to co-ordinate continuing education for health workers (both public and private) in its area of jurisdiction. Butambala HSD
Butambala health sub-district is one of the four-health sub-districts found in Mpigi district, the other three being Mawokota North, Mawokota South and Gomba. . It is made up of five sub-counties with 25 parishes and has a total population of 87,958 in 17,742 households (National Census 2002). It has a total of 16 health units (1 hospital, 7 HC IIIs, 8 HC IIs) with a workforce of 150 health workers. The health units are uniformly distributed throughout the health sub-district and Gombe Hospital houses the headquarters of the health sub-district and the lower level health units are distributed among the five sub-counties as follows: Budde (2), Bulo (2), Kalamba (5), Kibibi (3) and Ngando (3). Most of the Health Centres are government owned. Up to now, it is still difficult to ascertain the total number of private clinics and drug shops because some are not registered. The top five diseases of the HSD (2001/2002) included: Malaria, Acute respiratory diseases, intestinal worms and dental diseases in that in order. The average Bed Occupancy Rate (2001/2002) was 69.7%. There were a total of 150 health workers in the 17 health units as at 31st, December 2002 (HSD supervision report, Dec.2002). The main economic activity in the health Sub-district is subsistence farming. Other activities include pitsawing, charcoal burning and brick-laying. What was known about CME
It was known that many health workers in Butambala health sub-district had attended various Continuing Education activities in the last three years (2000-2003). On the one hand, information available on the issue was limited and did not indicate who attended, what training was attended, where and when the training took place, whether there was follow-up etc. There was lack of a well-documented inventory on health personnel in the in-service training activities at all levels in the health sub-district. This made it difficult for the managers to select health workers for on going training since there was no database to refer to in identifying which one was due for which training. Since some courses were attended not out of demand or interest of health workers, but just for the sake of monetary benefits attached or being in close circles of the selectors, the implementation of skills obtained after the training has been poor. It was felt that this would subsequently affect the quality of services in the health sub-district for, if status quo was to be maintained, it was likely to create a few islands of "over-trained" but poor implementers and majority demotivated and under-trained health personnel in the health sub-district. There was thus a need to carry out an inventory of continuing education activities that would provide baseline information for subsequent co-ordination and planning of continuing education in health sub-district. The study therefore sought to look for the Continuing Medical Education courses attended by Butambala Health sub-district service providers from the year 2000 to 2003; how the activities were organized and coordinated; the opinions about the training of those who attended, those who did not attend and the managers. It also intended to avail the HSD Management updated information on the training of health workers, which could be used in establishing a registry for the health workers' training. The Registry could help the HSD and the individual health units in the planning of continuing education in future. The information could also be used by managers in the selection of health workers to attend courses. This would probably reduce the problem of having the same workers attending the same courses more than once. The training based on individual needs and service demands may contribute to improved performance of health workers with eventual improvement in the quality of the services offered to the community and hence improved health status in the health sub district (other factors kept constant). Methodology The study was a descriptive cross-sectional one and a census of all the workers' history of post-basic training in the 3 years under study was taken. The study population was made up of all health workers in the functioning 16 health units (including Profit-not-for profit, PNFP) in HSD. Only those health workers who were on duty at the time of data collection were interviewed. Those on annual, study or other leave and those off duty were excluded. CME activities lasting between 1 day and 9 months attended by health workers from the 1st of July 2000 to the 30th of June 2003 (inclusive) were considered. The health workers in private-for-profit facilities and drug shops were not included. Sixteen (16) staff responsible for health units and one hundred thirty five (135) health workers were targeted using two different types of questionnaires respectively. The questionnaires were intervieweradministered. A review of supervision reports, visitors' books, CME records, HMIS records and financial records was carried out. Data were analyzed manually and with Microsoft excel, SPSS and Epi. Info 6.04. computer programmes. The findings of the study are as outlined in below. Results:
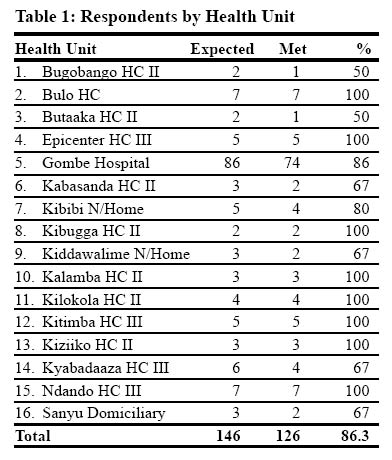
Respondents by health unit
A total of 16 functional units were visited and all health workers found at the station were interviewed. The following table shows workers interviewed by health unit compared to expected staff according to the stated staff enrollment. The response rate was 86.3% (126/146) of those expected, and it was considered satisfactory, being well above the set target of (85%). The majority of the respondents (74/126, or 58.7%) were from Gombe Hospital. (Table 1) Venue of training A total of 790 CME activities were held. The majority of these (431 or 54.6%) were internal or unit-based. The external CMEs were a total of up to 359 (45.4%). Gombe hospital contributed over 70% of the internal CME activities attended during the period under study. CME activities attended per year.
The total number of CMEs attended per year showed an ascending trend from 2000 to 2003 as in Graph 1. The increasing trend would imply that CMEs were being increasingly organized and attended by health providers. An analysis of the different courses attended was made and the following section discusses the findings. Course attendance
The most attended course was Malaria Case Management, by 94 out of 126 (74.6%) of the respondents. It was followed by Dental Health (42.8%), IMCI (41.3%), HIV/AIDS (40.5%) and Infection Control (40.5%). Notably, Management of a Rural Health Facility was the least held/attended with only (11.1%) of the respondents having attended the course. Only 2 management-oriented courses i.e. Health Information System and Management of a Rural Health Facility were held. See table 2 below. CME attendance by cadre An attempt was made to relate attendance of CME with cadre of health workers. The results show that the nursing aides/assistants had the least number of CMEs attended. However even within the same cadre, some members had more CMEs attended than others. (See table 3 below). Technical Support Supervision
Support supervision is one way of assisting health providers refresh their skills while at places of work and as such, serves as a form of CME. This study tried to find out the number of support supervision visits that were received by the different health workers during the period of study. Results show that the majority of the respondents (68/ 126 or 54%) had had between 1-5 follow-ups and only 10 (8%) had received more than 5 follow up visits. The 38% who did not receive any follow up were those who mainly attended internal CME. CME Organisation and Coordination The study looked at how CME activities were organized within the HSD and Units. Different health workers responsible for health units were asked how they organized CMEs in their units. They were asked on how they selected their staff for courses and how unit based CMEs were conducted. Table 4 below gives some of the findings. The study also looked at how unit-based CME activities were organized. Among the issues looked at included; who the organizers were, what the frequency was, how the topics for discussion were selected and what expenses were involved. Most of the staff in charge of health units interviewed showed that the decision to hold CME and who should attend was at times neither theirs nor the other workers'. Organizers of CME in HSD
The Ministry of Health headquarters and the District level rarely organized internal sessions. They were mainly organized by the health sub district and the health units themselves. Save for Gombe Hospital, all lower health unit CME activities were funded by the health sub-district, district or the MOH. However, no lower unit had money allocated for CME activities in their budgets. Although the district had money allocated and spent for CME activities, it was not easy to tease out what went to Butambala health workers specifically. Opinions of the H/workers on the selection process We found a relative balance between those who said the process was in order (56/126 or 44.4%) and those who needed a few improvements. Twenty seven (27/ 126 or 21%) felt that health workers should be selected basing on need and that Training Needs have to be identified before selection of course participants is done. On the other hand, 36 (29%) respondents thought that other changes needed to be effected in the selection process. The rest, 7(6%), did not respond to this question. How CME could be improved.
The respondents were asked of their opinions on how the process of CME can be improved. Most (52/126 or 41.3%) proposed that all staff cadres, and not just a few, need to attend training as a way to improve the process. Others suggested an increase in the number of CME sessions (28/126 or 22.2%), regular support supervision visits (20/126 or 15.9%) and regular refresher courses (17/126 or 13.5%) as a means for changing the whole process of CME. The findings showed that, during the period, unit-based (internal) training activities were more attended than external ones. This is in line with new CME policy of reducing or completely discouraging external inservice training activities because they tend to keep health workers away from station hence creating a vacuum. However, in reality the concept of unit-based CME was still weak in lower level health units. From the results, a deduction is made that on average the health workers in the HSD received inadequate CME yearly (Average 6 sessions per staff in three years). This finding is in agreement with a study done by Hardie (1981) where it was found that one of the common problem brought to the surface by health workers interviewed then was inadequate CME. The study also discovered that over 90% of health workers had attended at least one training activity, suggesting that CME was considered important in the HSD. However, the seemingly high coverage above went down to 67% when we increased the number of CME sessions attended per person to =3. The fact that this figure varies significantly from the general average of 6 sessions per staff indicates that some people attended more CMEs than others and confirms the complaint reported by some respondents that some of their colleagues were unfairly given more training opportunities than others. The National in-service training strategy was used to cover elements of the UMHCP. The results show that in Butambala HSD, this strategy is being adhered to, as 91% of the health workers interviewed had had at least one training session covering one or more elements of the package. Already about 60% of the nursing aides in the HSD completed the course. This implied that a considerable number of nursing assistants were exposed to the elements of the UMHCP and assumed to be delivering services within that framework. Although the majority of health workers reported to have been supervised at least once after their training, most of the supervision was done for one course IMCI. This could have been due to the way the course was designed, whereby a trainee was followed up for 4 weeks after training. The other explanation could be the big number of trained IMCI supervisors in the HSD (7). These could easily team up and carry out supervision visits. Management-oriented training was relegated to the rear and yet there is a manifest need for improved skills in management of the health services to avoid wastage and mishandling of resources. The observation that health workers were also not involved in planning their training and in selection of participants to the training explains the reports that health workers attended courses, not in their professional interests but purely for monetary purposes, given the allowances given to course participants. It could also explain the little effect the training seems to have had on those who attended it. Though unit-based CME was reported to have been organized, the sessions were not regular, and in fact, save for Gombe Hospital, most of the CME was held away from the units. This reflects the attitude that unitbased CME was not considered necessary by managers and their staff, especially those in the lower health units. Nursing assistants/nursing aides formed the bulk of the health workers in the HSD. The National In-Service Training Strategy (2001) emphasizes the importance of giving priority for continuing medical education to this group of health workers for, if they are not trained they will lack the skills to implement PHC essential packages. Conclusion
Although in-service training was found to be highly appreciated by the health workers in the HSD, the average number of sessions attended per person per year by health workers in the health sub district, is still inadequate. Despite the inadequate CME per individual per year, the attendance was also inequitable. The nursing assistant/aide cadre attendance was on average lower than other cadres. Although unit-based CME was more attended than external CME, in line with the new national CME strategy, there was generally less training in lower level units compared to the hospital and this was attributed to the little funding allocated for this exercise in the district budget. Support supervision was still inadequate, irregular and did not target the main causes of morbidity and mortality in the HSD, like malaria. The ordinary health workers were not involved in the organization of CME in the HSD and there was no bottom-up approach to planning of in-service training. Thus the health workers did not own the process of CME in the HSD. There was no report of any Training Needs Assessment conducted recently in the health sub district in the recent past. Recommendations
It was recommended that the staff responsible for the units could start drawing up CME plans at the beginning of each financial year and involve all the stakeholders in their units. This would increase the attitude of ownership of Internal CME by the staff and possibly improve upon their attendance. To increase the chances of every health worker attending training, the unit-based CME could be held at least once every week and the topics to be discussed could be identified by the health workers themselves. Alone or in conjunction with the District level, the head of the HSD could determine the training needs of the personnel each financial year, for consideration when training opportunities arise. In addition, the budget for CME could be increased such that at they hold more regular HSD-level CME. The heads of the HSD and the health units could each open up a registry for identified training needs, the CME activities carried out and the training attended by each health worker whether outside the HSD or at the HSD or at health unit level. This would ease the planning of CME by easing the choice of topics, venues and participants and also minimise the disaffection of the staff to the CME exercises due to the current (perceived or real) partiality in the selection of participants. The heads of the HSD and health units could jointly plan routine support supervision visits to the health units and make sure that a topic prior decided upon is discussed at each visit. Finally, the head of the HSD could, in conjunction with the district, strengthen collaboration with nearby training institutions like the Department of Health Sciences of Uganda Martyrs University -Nkozi which could help them to carry out more management-oriented CME in the HSD. References
Copyright 2004 - Department of Health Sciences of Uganda Martyrs University |

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}