 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
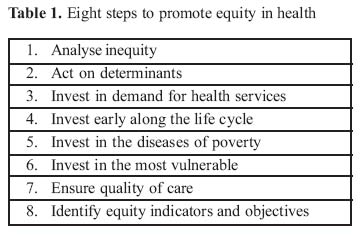
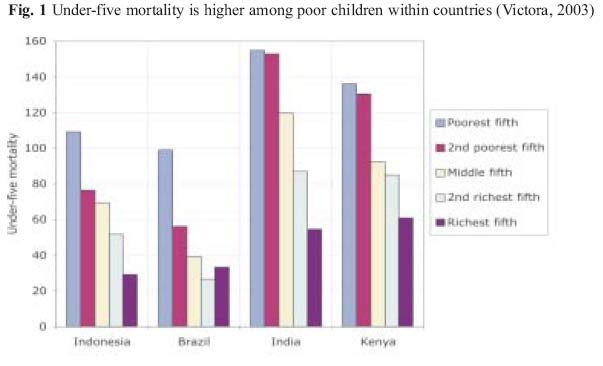
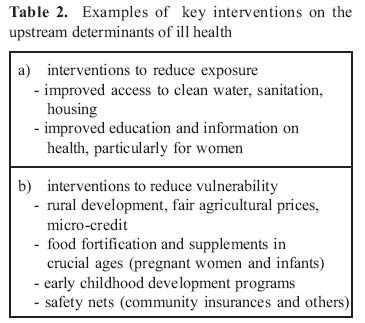
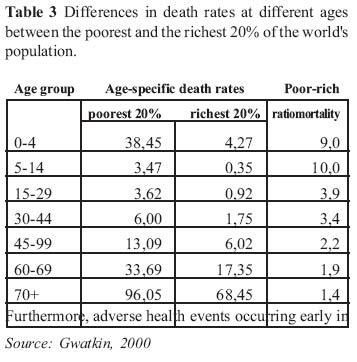
Health Policy and Development Journal, Vol. 2, No. 3, December, 2004, pp.186-191 PROMOTING EQUITY IN HEALTH Giorgio Tamburlini, Institute of Child Health IRCCS Burlo Garofolo, Trieste, Italy Code Number: hp04032 Abstract To promote health equity is to address a great deal of inequities in society. It is not easy but it can be done. It requires that an upstream action is taken. This action consists of eight steps: analyse inequity, act on determinants of inequity, invest in demand for health services, invest in life cycle improvement, invest in diseases of poverty, invest in the most vulnerable, ensure good quality of health care, and assess progress using well identified equity objectives and indicators. The exact details of the strategies to address inequity in health depend on the economic, administrative, political and epidemiological circumstances of each country. Introduction Promoting equity in health is not an easy task. Current trends in the global economy, in the environment and in the scientific and technological development are all conducive to increasing disparities in exposure to risk factors for ill health as well as in access to health services. Indeed, available data point to increasing inequalities in health outcomes among countries and within countries (World Bank, 2004; UNICEF, 2004). Thus, pursuing equity in health requires first of all a strong commitment and a clear awareness of the powerful driving forces that are currently working in the opposite direction. It should also be recognized that seldom in the past an equity lens was applied to the evaluation of the impact of health policies and programs. Most health professionals and policy-makers have been essentially concerned with the output of health programs, sometimes with the actual outcome, but little if any attention has been paid to the distribution of the health benefits across population groups. Better understanding of equity issues in health is a recent achievement. Health indicators that are able to describe health status or even access to health services by population groups have been developed and introduced only recently and their use is far from being widespread although increasing among international agencies - eg. in UNICEF and WHO reports and in World Bank Poverty Assessments - and NGOs. Furthermore, if some good analytical work has allowed a better understanding of the mechanisms which produce inequity in health (Gwatkin, 2000 and 2001), we are certainly far from knowing what really works in promoting equity. The complexity of the issue does not help. First, factors well beyond the health sector, such as macro-economic and sectoral policies, are crucial in determining progressive (i.e. in the direction of a more equitable distribution) or regressive (vice versa) effects on health. Second, policies to promote equity in health vary considerably depending on the body involved. International Agencies may use grants and lending to promote pro - poor and more equitable policies at country level, for example through the Poverty Reduction Strategy Papers promoted by the World Bank; and pay attention to international agreements such as those debated at World Trade Organisation, (Treaty on Intellectual Property Rights, General Agreement on Trade in Services), since they also have obvious implications for equity in access to health services (Ciccio, 2004). Governments should focus on macroeconomic stabilization, fiscal policy, welfare systems - including of course health system financing and provision - as crucial areas to promote equity. Communities may offer a far more different perspective: voice and power, in other words democracy, are essential tools in the struggle for a more equitable distribution of services at community level, while social cohesion and a certain degree of governance and organization are essential ingredients. This paper, which draws from current debate as well as from personal experience, will not discuss these diverse perspectives. Its purpose is essentially that of helping health professionals, as well as NGOs who work in the field, to incorporate the equity issue in evaluating and planning their work. A road to equity is proposed and includes eight major steps (Table 1). 1. Analyse inequity To analyse inequity we must first be able to describe it. Breakdown by socio-economical status (SES) of basic health status indicators, such as life expectancy, Infant Mortality Rate, under 5 Mortality Rate, maternal mortality ratio or disease-specific mortality rates is an essential requisite. Information on household assets can be used to indirectly assess SES and several methods are currently used in periodic surveys carried out by international agencies, such as the Demographic and Health Surveys. Once this information is available, we may want to see whether and to which extent the gap between the health status of the richest and the poorest changes within countries (fig.1), as well as across provinces or districts. The same can be done for indicators of access o health services, bearing in mind that there may be important differences depending on the type of service. For example, striking inequities in access to delivery services are common in many developing countries, while the same may not be true to the same extent with respect to access to Oral Rehydration Salts for diarrhoea. In general, the more health care gets complex and expensive, the greater the inequity. Of course, one should never forget that inequity is not limited to the SES dimension, and may also regard gender, ethnicity, and the rural-urban divide. 2. Act on determinants Once sufficient data are available to quantify differences and identify trends, our analysis must be able to capture the main determinants of inequity. "Bani guangnay, talkatarey hama" (ill health is the granddaughter of poverty) says a proverb from Niger. We all know this, and apparently there is not much health professionals can do about it. If poverty is the grandmother of ill health, who are the parents? In most instances poverty implies greater exposure to lack of safe water and sanitation, inadequate shelter, poor indoor air, and unsafe and insecure environments. It also determines, through poor nutrition and poor care, greater vulnerability to infections, poor cognitive stimulation, stunted growth, and violence. Thus, increased exposure and vulnerability to health hazards can be considered as the parents of ill health. For sure, they are the factors which explain most of the difference in health outcomes between the rich and the poor (or between boys and girls, urban and rural populations etc.). It is only at this point of the causal pathway that disparities in access to health services get into the play and contribute to further differences in outcomes. As a consequence, if promoting equity is our aim, intervening only downstream by improving provision and access to health services may be too little and too late. Understanding this etiological sequence is essential to identify some key priority areas for intervention (table 2). Some of these interventions are within the scope of comprehensive health services (in fact some of the readers might recognise several components of the Primary Health Care as defined at the Alma Ata Conference in 1978), others are beyond. Most of them would need multi-sectoral collaboration, and efforts to give voice to the less privileged and build community cohesion and capacity. 3. Invest in demand for health services "The availability of good health care tends to vary inversely with the need for it in the population served". The inverse care law as originally formulated (Tudor Hart, 1971) is the consequence of the fact that both provision and quality of services are invariably better for the richer, which should imply that if provision of services for the poor is improved, health care will also be better. Unfortunately, in most cases this is neither simple nor entirely true. The inverse equity hypothesis was recently developed to describe the common finding that the extension to the poor people of new health technologies, such as vaccines or specific treatments, is usually delayed by a matter of several years, sometimes decades (Victora, 2000). Now, differences in the supply of services are not sufficient to explain this finding, since in most instances what is lacking is the actual demand of services by poor people. To illustrate this point, let us take the case of attended delivery, one of the areas of care where differences between the poorest and the richest are greatest. There are several reasons on the demand side that might concur to explain why poor women may not have access to attended delivery: the household may not have the financial resources to cover the direct or indirect cost of the service, the information that a safer way to give birth to a child may just not be available, the dominant culture may not include delivery by a skilled attendant, or the problem may be the lack of voice and power of women as opposed to men. Thus, assets, direct costs and opportunity costs, information, education, culture and the status of women may all represent obstacles to access for the poorest, even if the service is in theory provided for all. This prompts us to state that, particularly in contexts characterized by extreme poverty and widespread social exclusion, the demand for health services may be critically limited. In this contexts pro-poor policies cannot be restricted to better supply of services but should entail measures to remove obstacles to demand. Otherwise, no surprise that results will be partial. 4. Invest early along the life cycle Due to unique exposure and most of all to greater vulnerability, risk differentials are maximal during pregnancy and delivery and the early years of life. Maternal mortality can be 100 times higher in poor populations than in the well-off, who can afford high quality prenatal and delivery care. Globally, children in the poorest quintile have about 10 times higher risk of dying than those in the richest quintile (Table 3). Furthermore, adverse health events occurring early in the life cycle - such as disease during pregnancy, complications of delivery, infections poor nutrition and poor care in newborn babies, infants and young children - have higher probability to produce irreversibile and sometimes intergenerational effects. This is why investments in health in early years not only have a higher cost effectiveness than investments in later years, but they have the greatest potential to reduce poverty and inequalities in health outcomes (Hoddinott and Quisumbing, 2003). As a consequence, interventions aimed at improving the health of mothers, babies and young infants should be prioritized among other health programs. 5. Invest in the diseases of poverty Poor people are not only at higher risk of ill health, but, due to the combination of exposures which are more common among poor populations and in poor households, incur more frequently some specific diseases. As a consequence, targeting these diseases with specific programs is considered one of the strategies to improve more selectively the health of the poor and to improve equity . The term diseases of poverty is currently adopted to indicate HIV/AIDS, tuberculosis and malaria and certainly these represent globally some of the biggest killers of poor people. However, we should not forget that perinatal problems, infectious diseases and malnutrition still provide the greater contribution to the burden of disease among poor people in most of the poorest countries. Thus, there is the need to carefully evaluate what are the biggest contributors to ill health among the poor in each specific area. Moreover, the opportunity of concentrating most resources on single disease-programs should be carefully evaluated taking into account the risk of further compromising the capacity of health systems, and particularly of primary care facilities, of providing comprehensive preventive and curative care for all the major diseases. 6. Invest in the most vulnerable Targeting poor people is probably the most direct way of reducing disparities. Providing better infrastructure and services in urban slums and poor rural areas, to households which bear the burden of disabled people or critically vulnerable children such as AIDS orphans, or to marginalised ethnic minorities, may all contribute to counteract the inverse care law. Since, in general, due to the high prevalence of diseases that can be prevented or cured at low cost, greater health benefits can be achieved, spending in preventive and curative for the poor is more efficient in terms of avoidable burden of disease (Claeson, 2000; Commission on Macroeconomics and Health, 2001). However, this kind of ethically and economically sound investments are rarely made. There are several reasons for this. First, the distribution of services and infrastructure is usually a function of political voice and power, which, by definition, marginalised population groups do not have. Second, there is little doubt that providing services in poorer areas entails a number of logistical difficulties (for example, recruitment of personnel). The greater cost-effectiveness does not imply that costs are lower (in fact, it is usually the opposite), rather that the impact on health can be much greater. But few policy makers are concerned about health outcomes, particularly if the short term political benefit is uncertain. Area-based programs should be preferred when vulnerable groups are geographically concentrated, while household-based programs, such as free access or vouchers for specific health services, may be a better choice when there is the possibility to identify those most in need within a specific area. A way of addressing the most vulnerable is providing safety nets to those households and individuals who, due to serious disability or chronic disease, may incur catastrophic spending. There are several kind of insurance schemes, some of which may be set up at community level, that can offer protection from the vicious cycle ill health - poverty which is so common among poor people (and even among the relatively poor when there is no universal access to health care nor welfare benefits for the chronically ill). 7. Ensure quality of care All too often, provision of services has been considered as synonymous of access to quality care, and coverage as implying effective health protection. Unfortunately, one of the several factors that explain the striking inequalities between the rich and the poor, is the difference in the quality of care. There are no health gains without delivery of effective interventions, which are produced by competent staff and appropriate supplies and equipment. In so many health services, including hospital services, quality of care is so low that little or no health gain is to be expected from access to the service (Nolan, 2000), and it may well be that patients incur costs without getting any real benefits (Tamburlini, 2004), sometimes in fact getting in further trouble due to hospital acquired infections or hazardous procedures. The basic requisites for quality of care (i.e. competent staff and sufficient supplies) must be ensured if health benefits have to be achieved from health services. There is nothing worse than deceiving poor people by making them believe that they are getting something which will be helpful for their health, while they are not. This, however, is what happens in most countries to poor people, particularly - but not exclusively - in the private drug market. Once more, quality of care is responsibility of health professionals, health administrators, policy makers but it is also a function of competent demand of services. As a consequence, educated and informed users will usually be able to get more quality from the service or to choose those services that offer better quality. 8. Identify equity indicators and objectives We have so far shown that achieving more equity in health is not easy. The task will never be accomplished unless an explicit clear commitment is made and specific objectives are set. Ultimately, since the objective is to reduce the differences in health outcomes, the best indicators are those describing the distribution of health outcomes by SES groups (usually by income quintiles); breakdown of health indicators by adjunctive variables such as urban/rural, male/female or others may be useful to thoroughly describe health inequities. Process indicators too are useful to monitor what we are doing, and the proportion of attended deliveries, immunised children, patient receiving Directly Observed Treatment Short Course, etc. may be expressed by population groups. According to what we have said about the importance of ensuring quality, the above indicators should be complemented by some tracers of quality such as for example children receiving the right treatment when diagnosed pneumonia at the health centre or severe complicated malaria in hospital. Various combination of outcome, process and quality indicators, depending on the availability of data and prevalent problems, should be used to assess periodically to which extent a specific service or program or health system is promoting equity in health. Conclusions Inequity in health is the product of inequity in society, and as such cannot be effectively addressed without acting upstream, i.e. on the factors which determine greater exposure and vulnerability to health hazards among poor people. Promoting equity in health is a complex endeavour which requires investments beyond the health sector as well as specific commitment of the health sector to target the diseases most prevalent among the poor, provide quality services in poor areas, interact with communities to improve their information and give them voice about health matters. Strategies to achieve better equity in health vary depending on the administrative, political and epidemiological context, and on the available levers, but will invariably require a combination of interventions which have been synthesised in eight steps. Analysis of inequities in health outcomes and clear identification of equity objectives and indicators represent in any case the minimum requirements for effective action. Based on this information, a periodical equity audit should be carried out by professionals in charge of health services and health programs, particularly by those involved in international cooperation projects. References
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}